Download presentation
Presentation is loading. Please wait.

1
Diabetes

2
Complication of diabetes:

3
Complication of diabetes:
Acute Complication Chronic Complication Hyperosmolar Hyperglycemic Non-Ketotic syndrome Diabetic Ketoacidosis Hypoglycemia Micro vascular Complication Macro vascular Complication Diabetic Nephropathy Coronary Artery Disease Diabetic Neuropathy Peripheral Vascular Disease Diabetic Retinopathy Cerebro Vascular Disease

4
1.) Hyperosmolar hyperglycemic non- Ketotic syndrome (HHNK):
It is defined as an extremely high blood glucose level, absence of or only small amount of ketones and profound dehydration. Glucose levels generally range from greater than 600 to 2000mg/dl. Patient who have HHNK syndrome have sufficient insulin to prevent lipolysis and ketosis. This condition occur rarely in older patient with type 2 diabetes.

5
Sign and symptoms: Blood sugar level over 600mg/dl. Dry, parched mouth. Extreme thirst. Warm, dry skin that does not sweat. High fever. Sleeping or confusion Hallucinations. Weakness or paralysis on one side of the body. loss of vision. profound dehydration (10%-15% loss of body water) Treatment: Intravenous fluid. Small amount of insulin is given to correct hyperglycemia.
 Treatment: Intravenous fluid. Small amount of insulin is given to correct hyperglycemia.")
6
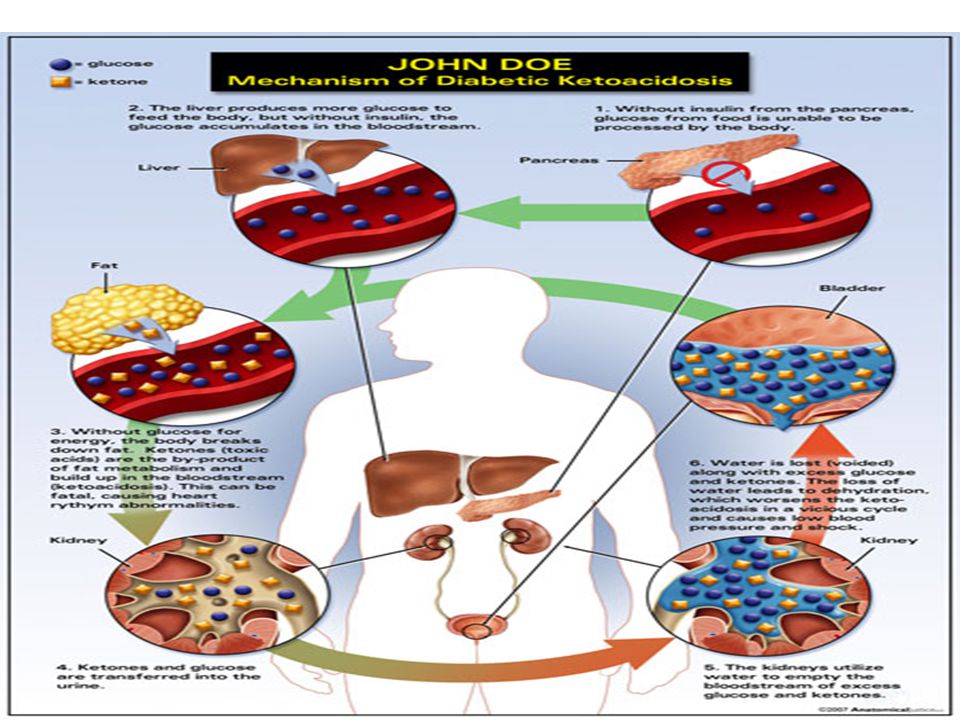
2.) Hyperglycemia/diabetic ketoacidosis (DKA)
Diabetic ketoacidosis (DKA), a life-threatening complication characterized by severe disturbances in carbohydrate, protein, and fat metabolism. DKA is always the result of inadequate insulin for glucose use. As a result, the body depends on fat for Energy and ketones are formed. Acidosis results from increased production and decreased use of acetoaceticacid and 3-B- hydroxybutyric acid from fatty acids. These ketones spill into the urine; hence the reliance on testing for ketones.
, a life-threatening complication characterized by severe disturbances in carbohydrate, protein, and fat metabolism. DKA is always the result of inadequate insulin for glucose use. As a result, the body depends on fat for Energy and ketones are formed. Acidosis results from increased production and decreased use of acetoaceticacid and 3-B- hydroxybutyric acid from fatty acids. These ketones spill into the urine; hence the reliance on testing for ketones.")
7
DKA is characterized by elevated blood glucose levels (>250 mg/dl but generally <600 mgldl) and the presence of ketones in the blood and urine. Acute illnesses such as flu, colds, vomiting, and diarrhea, if not managed appropriately, can lead to the development of DKA. If DKA left untreated, It can lead to coma and death.

9
. Symptoms include: Headache Anorexia Nausea Dehydration Polydipsia
. Symptoms include: Headache Anorexia Nausea Dehydration Polydipsia The fruity odor of ketones Fatigue Low blood pressure Constipation Muscle cramps Altered vision Treatment: Increase regular insulin dose by at least 20%. Fluid and electrolyte replacement. Medical monitoring

10
3.) Hypoglycemia: This is a condition of low blood glucose levels as a result of- overdose of insulin, failure to eat food after a dose of insulin, loss of food through vomiting or diarrhea or exercise without modifying the insulin dose. Blood glucose level fall to as low as 50mg/100ml. Hypoglycemia is a common side effect of insulin therapy.

11
Symptoms of hypoglycemia:

12
Causes of Hypoglycemia
Deliberate errors in insulin doses Excessive insulin or oral secretagogue medications Improper timing of insulin in relation to food intake Omitted or inadequate meals or snacks Delayed meals or snacks Unplanned or increased physical activities or exercise Alcohol intake without food.

13
Treatment of hypoglycemia:
If the blood glucose level falls,15 g of carbohydrate should be given. If the patient is so stuporous that he can’t swallow, given an intravenous injection of 25 g of glucose. As patient is able to swallow, he should be given 30 g of sugar by mouth. The patient must be educated that unpunctual meals and unaccustomed exercise may precipitate hypoglycemia and they must always carry some tablets of glucose or some sugar for use in an emergency. Patients need to be reminded of the need to treat hypoglycemia , even in the absence of symptoms.

14
HYPERGLYCEMIA AFTER HYPOGLYCEMIA
Hypoglycemia followed by “ rebound” hyperglycemia is called the somogyi effect. This phenomenon originates during hypoglycemia with the secretion of counter regulatory hormones and is usually caused by excessive exogenous insulin doses. Hepatic glucose production is stimulated thus raising blood glucose levels. If rebound hyperglycemia goes unrecognized and insulin doses are increased, a cycle of over insulinization may result.

15
Chronic or long term complication:
1.) Macrovascular diseases involve diseases of large blood vessel. In this blood vessel walls become thicken, and closed by plaque then blood flow is reduced or blocked. Macrovascular diseases including: coronary heart disease (CHD), peripheral vascular disease (PVD), and cerebro vascular disease (CVD).
 Macrovascular diseases involve diseases of large blood vessel. In this blood vessel walls become thicken, and closed by plaque then blood flow is reduced or blocked. Macrovascular diseases including: coronary heart disease (CHD), peripheral vascular disease (PVD), and. cerebro vascular disease (CVD).")
16
i.) Coronary artery disease:
In this condition blood vessel of the heart become narrowed or blocked by plaque, and the blood supply to heart is reduced or cut off, resulting in a heart attack. Symptoms: Dyspnea (Difficulty in breathing). Fatigue Chest pain Weakness Paroxysmal nocturnal (Shortness of breath).
. Fatigue. Chest pain. Weakness. Paroxysmal nocturnal (Shortness of breath).")
17
ii.) Cerebral vascular disease:
It is caused by narrowing, blocking, or hardening of brain blood vessel or by high blood pressure. It affects the blood flow to the brain, leading to stroke. Stroke: A stroke result when blood supply to the brain is suddenly cut off, which can occur when a blood vessel in the brain or neck is blocked or bursts. Brain cells are then deprived of oxygen and die.

18
Symptoms of cerebro vascular disease: Dysarthria (Disorder of speech)
Unilateral weakness Vision difficulty in one or both eyes Severe headaches

19
iii.) Peripheral vascular disease:
In this condition, blood vessel in the legs are narrowed or blocked by plaque, blood flow is decreased to the legs and feet. Poor circulation in the legs and feet raises the risk of amputation. Symptoms: Foot ulcer Pain in buttocks, thighs and calf.

20
Causes of macro vascular disease:
High triglyceride level High LDL Cholesterol level Lower HDL cholesterol levels High blood pressure Smoking Poor blood glucose control Obesity Little exercise

21
Management of Macro vascular disease:
Decrease blood pressure to a desirable value 130/80mm. Reducing LDL cholesterol concentrations to less than 100mg/dl. Decrease daily fat intake Control blood glucose level. Diet and exercise are important for obesity and hypertension.

22
Hypertension: Treatment of hypertension:
Hypertension is a common comorbidity of diabetes, about73% of adults with diabetes having blood pressure of 130/80 mm Hg or higher. Treatment of hypertension: Blood pressure should be measured at every routine visit. Medical nutrition therapy. Drug therapy.

23
2.) Micro vascular disease:
Micro-vascular diseases associated with diabetes involve the small blood vessels. It include: Diabetic Retinopathy Diabetic Nephropathy Diabetic Neuropathy

24
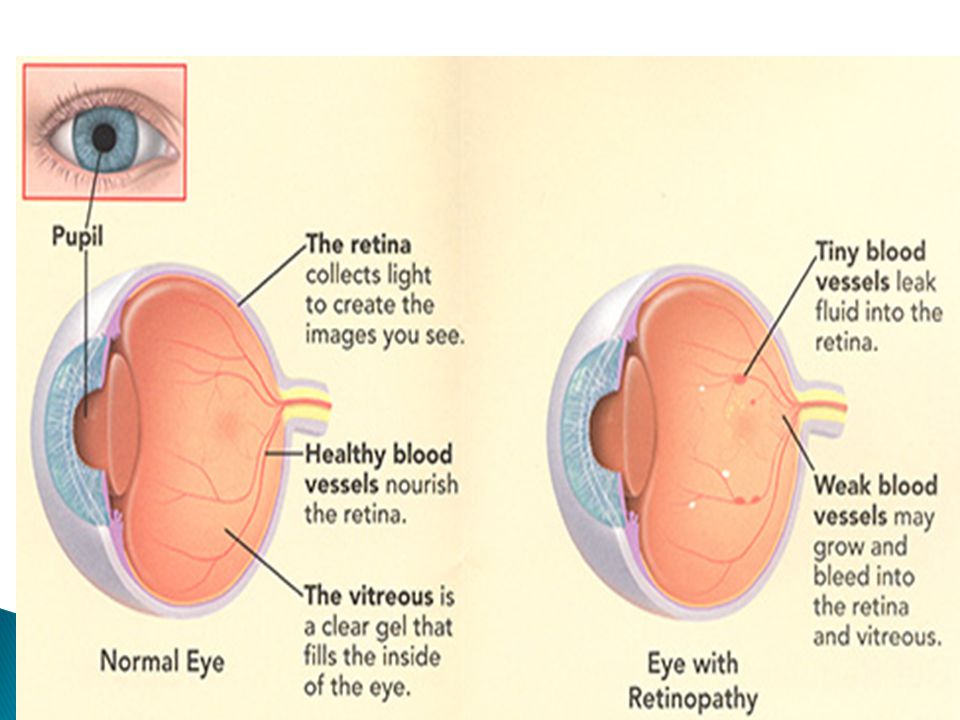
1.) Diabetic retinopathy: Diabetic retinopathy (DR) can be defined as damage to micro vascular system in the retina due to prolonged hyperglycaemia. After 20 years of diabetes, nearly all patients with type 1 diabetes and more than 60% of patients with type 2 diabetes have some degree of retinopathy.
 can be defined as damage to micro vascular system in the retina due to prolonged hyperglycaemia. After 20 years of diabetes, nearly all patients with type 1 diabetes and more than 60% of patients with type 2 diabetes have some degree of retinopathy.")
26
There are two stages of diabetic retinopathy:
Non proliferative Diabetic Retinopathy Proliferative Diabetic Retinopathy.

27
1.) Non proliferative Diabetic Retinopathy:
The early stage is non proliferative diabetic retinopathy (NPDR). It has three stages: Mild Non proliferative Retinopathy: At this earliest stage, microaneurysms occur. They are small areas of balloon- like swelling in the retina's tiny blood vessels. Moderate Non proliferative Retinopathy: As the disease progresses, some blood vessels that nourish the retina are blocked.
. It has three stages: Mild Non proliferative Retinopathy: At this earliest stage, microaneurysms occur. They are small areas of balloon- like swelling in the retina s tiny blood vessels. Moderate Non proliferative Retinopathy: As the disease progresses, some blood vessels that nourish the retina are blocked.")
28
Severe Non proliferative Retinopathy: Many more blood vessels are blocked, it results more areas of the Retina being deprived of nourishment and oxygen. A lack of sufficient oxygen supply to the Retina results in a condition called “Retinal Ischemia”. These areas of the retina send signals to the body to grow new blood vessels for nourishment.

29
2.) Proliferative Diabetic Retinopathy (PDR):
It is the most advanced and most vision- threatening stage of diabetic retinopathy. At this advanced stage, the signals sent by the retina for nourishment cause the growth of new blood vessels. The new blood vessels grow along the retina and along the surface of the clear, vitreous gel that fills inside of the eye. The new vessels are fragile and prone to bleeding, resulting in vitreous hemorrhage and retinal detachment. These changes interfere with vision and may ultimately lead to blindness.

31
3.) Diabetic macular edema
Diabetic macular edema, involves thickening of the central (macular) portion of the retina, and glaucoma, in which fibrous scar tissue increases intraocular pressure. Macular edema may cause reduced or distorted vision. Diabetic macular edema can be present at any stage of the disease, but is more common in patients with proliferative diabetic retinopathy.
 portion of the retina, and glaucoma, in which fibrous scar tissue increases intraocular pressure. Macular edema may cause reduced or distorted vision. Diabetic macular edema can be present at any stage of the disease, but is more common in patients with proliferative diabetic retinopathy.")
33
Symptoms : Risk factor: Blurry or double vision.
Flashing lights or blank spots. Dark or floating spots. Pain or pressure in one or both eyes. Difficulty in seeing the things out of the corner of eyes. Risk factor: Poor blood sugar control. High blood pressure Raised level of fat in blood. Longer you have had diabetic.

34
Management of Diabetic Retinopathy:
Keep your blood glucose and blood pressure as close to normal as you can. Examine your eye once a year. Treatment: Laser treatment: Laser treatment is used to stop the leakage of blood and fluid into the retina. A laser beam of light can be used to create small burns in areas of the retina with abnormal blood vessels to try to seal the leaks.

35
Vitrectomy: when you have a lot of blood in the centre of eye need vitrectomy to restore your sight. A tiny incision is made in eyes, then a small instrument is used to remove viterous gel that is clouded with blood . The viterous gel is replaced with a salt solution.

36
2.) Diabetic Nephropathy:
Functional changes occur in the nephrons of the kidney. The basement membrane of the glomeruli thickens which may lead to diabetic glomerulosclerosis. Which of two types : Diffuse and Nodular Diffuse is more common with generalized thickening of capillary walls. while in case of the nodular, rounded masses of acellular, hyaline material are superimposed on the diffuse lesion of the glomeruli. These are called kimmelstiel - wilson nodules. These changes lead to proteinuria with increasing renal failure and uraemia, if diabetes is uncontrolled. About 20 to 40% of patients with diabetes develop evidence of nephropathy.

37
Clinical evidence of nephropathy is the appearance of low but abnormal urine albumin levels (30 to 299 mg/24 hr), referred to as microalbuminuria. Microalbuminuria is rare during the First five year after onset of diabetes. Microalbuminuria is also a marker of increased cardiovascular disease risk. When diabetic nephropathy has continued for some time, the condition will develop into something called End- Stage Renal Disease (ESRD). At this point, the kidney will have completely stopped functioning, and a kidney transplant or dialysis will become necessary.
. At this point, the kidney will have completely stopped functioning, and a kidney transplant or dialysis will become necessary.")
39
Symptoms: Ankle and leg swelling (Pedal edema)
Weight gain Elevated blood urea nitrogen (BUN) and creatinine levels Uncontrolled hypertension Uremia due to accumulation of metabolic wastes Ankle and leg swelling (Pedal edema) Reduced urination (<400ml/day-oliguria) Anorexia and weakness Nausea and vomiting Itching Breathlessness Palpitation
 and creatinine levels. Uncontrolled hypertension. Uremia due to accumulation of metabolic wastes. Ankle and leg swelling (Pedal edema) Reduced urination (<400ml/day-oliguria) Anorexia and weakness. Nausea and vomiting. Itching. Breathlessness. Palpitation.")
40
Management: Test regularly for microalbuminuria
Exercise daily and loss weight to maintain ideal body weight. Avoid tobacco and alcohol. Avoid nephrotoxic drugs like NSAIDS Glycemic control of HbA1c<7% Blood pressure control of <130/80mm hg Appropriate diet Test regularly for microalbuminuria

41
Diabetic Neuropathy: Damage to the nerve is called neuropathy. Neuropathy as a result of diabetes is called diabetic neuropathy. Chronic high levels of blood glucose are associated with nerve damage and affect 60 to 70% of patients with both type I and type 2 diabetes. Damage nerves cannot pass the signals to and from the brain properly. As a result, either have loss of sensation or pain in the affected parts.

42
Symptoms of Neuropathy:
Numbness, tingling or pain in toes, feet, legs, arms and fingers Wasting of muscle of feet or hands Nausea or vomiting Diarrhea or constipation Weakness Dizziness or fainting

43
Chronic Peripheral Neuropathy Autonomic Neuropathy Proximal Neuropathy
Type of Diabetic Neuropathy: Chronic Peripheral Neuropathy Autonomic Neuropathy Proximal Neuropathy Focal Neuropathy

44
I.) Chronic Peripheral neuropathy:
It is also called distal symmetric neuropathy or sensorymotor neuropathy. It affects the nerves of Toes, feet , legs, hands and arms. Peripheral neuropathy may cause muscle weakness and foot deformities. This form is common in elderly diabetics with long- standing disease, but rare in diabetics under 20 year of age.

45
Symptoms: Numbness Tingling or burning sensation
Loss of balance and coordination. Extreme sensitivity to touch Sharp pain or cramps Loss of vibration sense at the ankle or knee.

46
2.) Autonomic Neuropathy:
Autonomic neuropathy affects nerve that control heart, regulate Blood pressure and control blood glucose level. It also affects- Bladder,Intestine,Sex organ and Lungs.

47
Autonomic nervous system cause:
Diarrhea, Impotence and postural hypotension Disturbances of sweating

48
3.) Proximal Neuropathy:
It is also called diabetic amyotrophy. In this pain is occur in hips, buttocks, thighs and legs , usually on one side of body. It can lead to weakness in legs. This type of neuropathy is more common in those with type 2 diabetes and in older adults with diabetes.

49
Focal Neuropathy: Focal neuropathy appear suddenly and it affects specific nerves most often in the head or legs. Focal neuropathy may cause: Double vision Paralysis on one side of face called bell’s palsy. Severe pain in the lower back or pelvic. Stomach, chest or side pain Pain inside the foot

50
Management of Neuropathy:
Bring blood glucose level with in the normal range Adequate diet Foot care Medication

51
Diabetic foot: Diabetes are affected by a peculiar disability which severely damages the tissues of the foot. It is seen in the form of chronic ulceration, sepsis and gangrene. It may necessitate amputation of the foot. Foot ulcer is the main problem in diabetes.

52
Three major factors have been identified which lead to the diabetic foot. they are:
Chronic diabetic neuropathy Atherosclerotic obstruction of the arteries that supply the lower limbs Bacterial infection

53
High risks of developing diabetic foot problems:
Damage to the nerves of the feet. Diseases of the blood vessels of the legs. Having foot ulcer in the past. Deformity of the foot. Presence of callus. Blind or with poor vision, kidney diseases, especially chronic kidney failure. Poor control of blood sugar levels. Reduced sensation in the feet.

54
General guidelines for preventing the foot ulcer:
Inspect your feet everyday in order to detect ulcer, if any, at the earliest. Check your shoes both inside and outside before wearing them to detect stones or other similar objects. Keep the feet away from heat, hot water, etc. Avoid walking barefoot. Avoiding soaking your feet, dry them with soft towel and carefully between your toes. Cut your toes nails each week or when needed. Prevent skin irritation by wearing thick, soft and seamless socks. Wear shoes that fit well and allow your toe to move.

55
Management of diabetes:
Diabetes can be managed by: Diet Oral hypoglycemic drug Insulin therapy

56
Diet Alone: Diet must be nutritionally adequate for the patients needs: Energy: calories according to the body’s daily requirement. The total calories advised will vary for each patient. An obese middle aged or elderly patient with mild diabetes, kcal daily given. An elderly diabetic but not overweight kcal daily given. A young active diabetic kcal daily given. Person engaged in physical activity, the recommended calorie intake may be increased as per needs. Carbohydrates: A Moderate restriction of carbohydrate calories is made to about 50 – 60% of total calories. Carbohydrate intake should not exceed 250g per day. Complex carbohydrates such as wheat, rice, jowar, bajra should be eaten rather than simple carbohydrate.

57
Protein: The normal RDA for protein is 0. 8 g/kg IBW
Protein: The normal RDA for protein is 0.8 g/kg IBW. slightly higher than normal protein are given. Protein should provide 15 – 20% of the total energy. In IDDM children g/kg body weight is recommended. Fat: Total fat intake is lowered to 20% or less of the day’s energy intake in case of obese and adult diabetics. polyunsaturated fats should be given rather than saturated one’s. Daily Intake of cholesterol should be limited to 300mg or less. Fiber: Diabetics must consume g fiber daily. Diet high in soluble fiber (pectin, gums, roots, tubers) help to reduce serum levels of glucose and insulin. Fenugreeks seeds which contain high fiber are useful. Sodium: The daily intake must not exceed 3000mg sodium per day. Some may recommended 2400 mg sodium per day, especially for people having congestive heart failure, nephropathy or hypertension.
 help to reduce serum levels of glucose and insulin. Fenugreeks seeds which contain high fiber are useful. Sodium: The daily intake must not exceed 3000mg sodium per day. Some may recommended 2400 mg sodium per day, especially for people having congestive heart failure, nephropathy or hypertension.")
58
Calculation of diabetic diet:
If a person is 25 year old, 170 cm tall, and his desirable weight is 60kg. Calories: 30 kcal per kilogram of desirable body weight . 60 x 30=1800 kcal per day Protein: 12 to 20 % of total calories 1800 x 15 % = 270 kcal 270 kcal ÷ 4=67.5 g protein daily Carbohydrates: 50 to 60 % of total calories 1800 x 55%=990 kcal 990÷4=247.5 g carbohydrate per day

59
Fat: Total calories – (Protein calories + Carbohydrate calorie).
1800 – ( ) = 540 kcal Fat calories divided by 9 to convert kcal into gram 540 ÷ 9 = 60 g fat per day
 = 540 kcal. Fat calories divided by 9 to convert kcal into gram. 540 ÷ 9 = 60 g fat per day.")
60
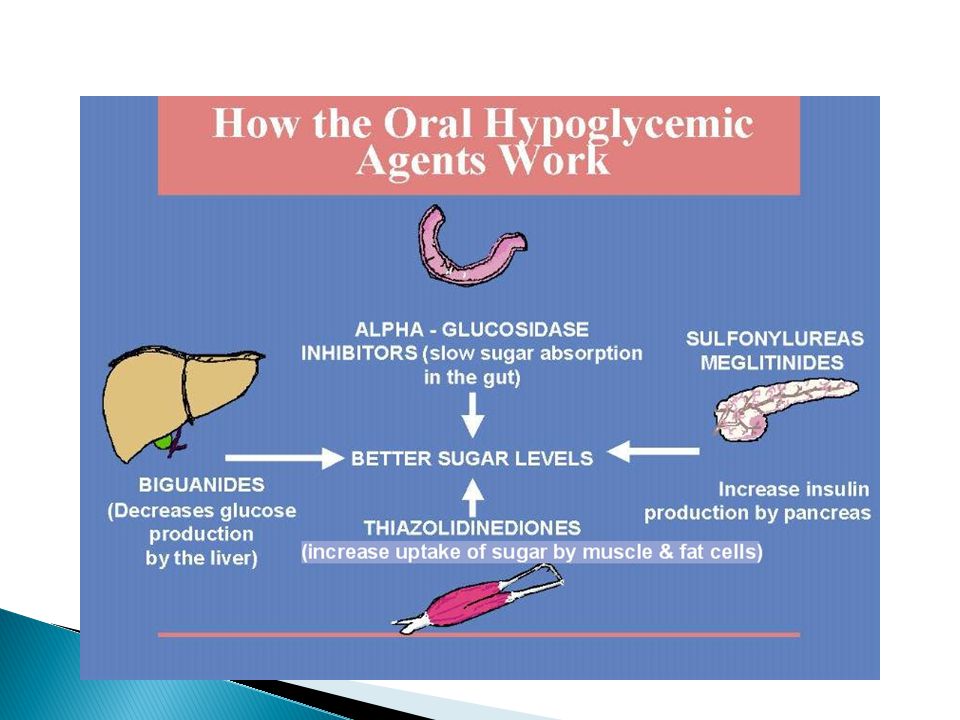
Oral hypoglycemic drugs:
Patient of normal weight may be started on oral hypoglycemic drug as soon as it is clear that dietary measures alone are inadequate. These help in lowering the deviated blood glucose and so are used in treatment of hyperglycemia in NIDDM patients. They act by stimulating the pancreas to produce more endogenous insulin and enhance peripheral sensitivity to insulin.

61
Oral hypoglycemic drugs belong to the group of:
Sulphonylureas Beguanides

62
Sulphonylureas: These are valuable in the treatment of Patient with Type II diabetes who fail to respond to simple dietary restrictions and who are not overweight. These should not be given to obese patient as by stimulating the production of endogenous insulin, these drugs lead to increase in weight.

63
Tolbutamide: It is the mildest and probably the safest sulphonylureas. Its effective action is 6 to 8 hours and should be taken 2 to 3 times a day. Required to maintain normal blood glucose level. The doses varies between 1 to 2 g/ day. It is well tolerated and toxic reaction like skin rashes are rare but relapse rate is relatively high.

64
Chlorpropamide: It has a biological half life of about 36 hours. It is able to maintain blood glucose by a single dose of 100 to 375 mg/day. Large doses lead to toxic effect such as jaundice and skin rashes. Once glycosuria has been abolished, the dose should be reduce according to the doctor advice or otherwise it might lead to hypoglycemia.

65
Biguanides: Biguanides are less widely used than the sulphonylureas because of higher incidence of adverse effect, particularly gastreointestinal symptoms. Biguanides reduce the conversion of fats and proteins into glucose in the liver. These are normally recommended for people who are obese, are insulin resistant and have relatively less high blood sugar. It is given in combination with sulphonylurea if the latter does not control high blood sugar levels effectively. They are normally not recommended if you have heart, liver or kidney diseases.

66
Metformin of this group is more acceptable
Metformin of this group is more acceptable.It is less likely to cause gastreointestinal side effects than phenformin. Metformin is given with food in 2 or 3 daily doses of 0.5 to 1.0g each. Phenformin : the usual dose of this is 50 to 150 mg/day.

67
Side effect of Biguanides:
Unpleasant, bitter or metallic taste loss of appetite nausea discomfort into the abdomen lethargy weakness of the muscle excessive weight loss in some people These side effect can be reduced by taking the medicine with or just before meals.

68
Alpha – glucoside inhibitors:
Acarbose is the medicines of this group. It delays absorption of carbohydrates from the intestines and is normally recommended for those who have high carbohydrate intake. It is also sometimes recommended for obese people who do not follow the recommended diet for diabetes. Acarbose may result, malabsorption in high doses. Mild side effects such as increased gas in the stomach, feeling of a bloating sensation in the abdomen and diarrhoea.

69
General precautions to be taken for oral medicines for diabetes:
In case you have acidity or other stomach disturbances, take the medicines with meals. Avoid drinking alcohol while on these medicines as it may react with the medicines and cause unpleasantness and flushing of the face. Some medicines increase the action of sulfonylurea and it is therefore desirable that you avoid taking any medicines without consulting your doctor. Inform your doctor if you are pregnant as some medicines are not recommended during pregnancy. In case you develop symptoms such as pain in the muscles. Stop the medicine and consult your doctor immediately. Stop taking the medicine in case allergic reactions develop.

71
Insulin Therapy: Insulin is used in the treatment of patients with diabetes of all types. The need for insulin depends upon the balance between insulin secretion and insulin resistance. For a patient, requiring less than 60 units of insulin per day, a single daily injection of one of the modified insulin such as protamine zinc insulin or zinc suspension suffices. Insulin can only be given as an injection. The meal pattern of a diabetic on insulin alone is determined according to the time at which the insulin is administered.

72
Short acting insulin: A short- acting insulin is given before breakfast and dinner to provide bolus insulin replacement. Medium acting or intermediate acting insulin: It is given once or twice a day in the morning, usually before breakfast.NPH is widely used. Long acting insulin: They may be given alone or may also be administered with regular insulin at breakfast. The pre-breakfast doses consist of about one third regular and two third NPH. These types of regimens allow increased flexibility in the type and timing of meals.

73
Requirement of insulin:
Adult with normal weight to height are prescribed 15 – 20 units of insulin per day. Obese require at least 25 – 30 units per day. The doses are increased gradually not more than 10 – 15% of total dose, generally not more than 6 units per day.

74
Distribution of calories and carbohydrates while using insulin:
The distribution of carbohydrate in various meals is determined by whether or not the patient is on insulin therapy. The carbohydrate is divided equally between breakfast, lunch and dinner. The distribution, however, may be varied according to the specific case, type of insulin and the advice of the doctor.

75
Distribution of calories and carbohydrates while using insulin:
Type of Insulin Breakfast Lunch Snacks Dinner Bedtime Short-acting: (Regular, semilente) 2/5 1/5 - None Intermediate acting: (NPH,Lente, globin) 1/7 2/7 Long- acting: (PZI,Ultralente) 20-40g CHO Regular insulin at breakfast 1/3
 2/5. 1/5. - None. Intermediate acting: (NPH,Lente, globin) 1/7. 2/7. Long- acting: (PZI,Ultralente) 20-40g CHO. Regular insulin at breakfast. 1/3.")
76
Insulin type and their duration time:
Onset (hour) Peak ( hour) Maximum duration (hour) short acting insulin: Lyspro 1-1.5 2-3 Regular 4-6 Medium acting insulin: NPH 2-4 4-10 14-18 Lente 3-4 4-12 16-20 Long acting insulin: Ultralente 6-10 Peakless 20-30 Mixed insulin: 70/30 2-3; 4-10 The Action of insulin and the peak absorption of carbohydrate should be at the same time.
 Peak ( hour) Maximum duration (hour) short acting insulin: Lyspro Regular Medium acting insulin: NPH Lente Long acting insulin: Ultralente Peakless Mixed insulin: 70/ ; The Action of insulin and the peak absorption of carbohydrate should be at the same time.")
77
Insulin is recommended for five main conditions:
Diabetes in children Diabetes among people who are underweight and malnourished. Tendency to develop ketoacidosis among diabetics. In emergencies such as surgery, pregnancy, high fever or diabetic coma. If other methods of blood sugar level such as medicines, diet and exercise have not been effective.

78
Devices used to inject insulin are:
1.) Insulin syringes 2.Insulin Pens
 Insulin syringes 2.Insulin Pens")
79
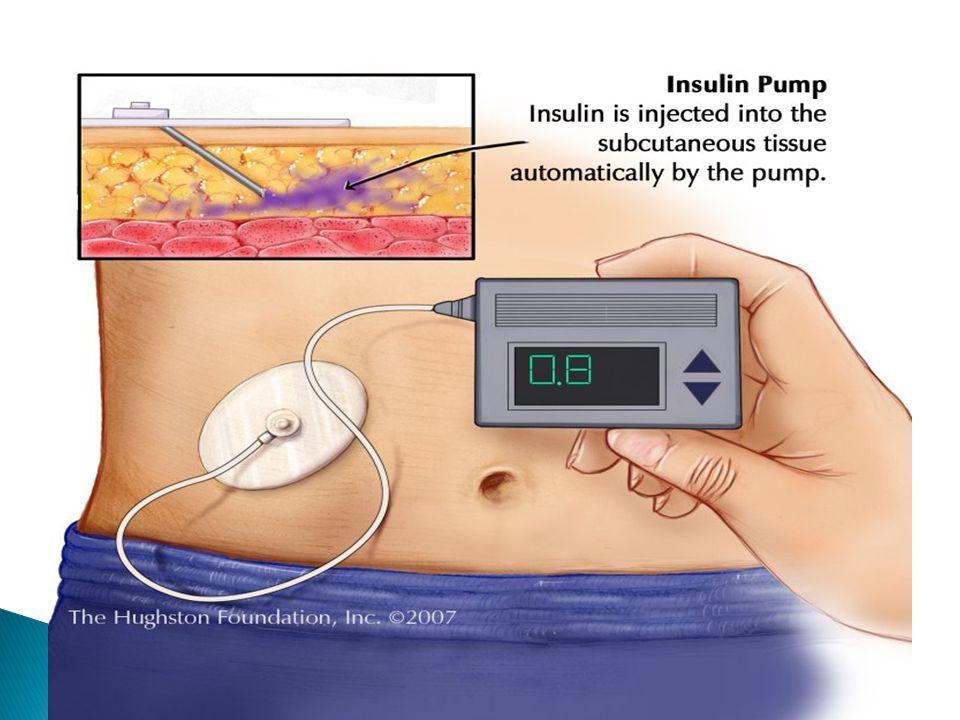
3.) Insulin pump therapy:
 Insulin pump therapy:")
80
Insulin pump therapy provides basal rapid-acting or short-acting insulin pumped continuously by a mechanical device in micro amounts through a subcutaneous catheter that is monitored 24 hours a day. It has a small portable pump with an infusion set that ends in a needle or cannula. The needle or cannula is put below the skin and changed once in 24 to 72 hours. Pump therapy requires a committed and motivated person who is willing to do a minimum of four blood glucose tests per day, keep blood glucose and food records, and learn the technical features of pump use.

82
Benefits of Insulin Pump Therapy
Insulin pump therapy provides more flexibility for your lifestyle while giving you greater control of your diabetes. More flexibility by not having to follow a strict schedule for eating, activity, and insulin injections Fewer injections Improved A1C Fewer hypoglycemic episodes (low blood sugars) Reduced long-term complications related to diabetes Better predictability for insulin absorption
 Reduced long-term complications related to diabetes. Better predictability for insulin absorption.")
83
common side effects insulin therapy:
Hypoglycemia Allergic reaction Insulin resistance Edema

84
Physical activity/Exercise:
Physical activity should be an integral part of the treatment plan for persons with diabetes. Aerobic exercise such as jogging, swimming, taking long walks, are recommended. Even light exercise can be important in a management programmed to control blood glucose and lipid levels. In IDDM individuals, the more vigorous exercises should be undertaken only if blood glucose is between mg/100ml and there is no ketosis present.

85
Benefits of exercise: Improve blood glucose control.
Decreased insulin resistance and Increased insulin sensitivity Reduce cardiovascular risk factors Control weight Improve metabolism Increase well-being Lowering in triglycerides and very – low- density lipoprotein (VLDL), Decrease in total cholesterol and low density lipoprotein (LDL) An increase in high density lipoprotein (HDL). Lowers blood pressure.
, Decrease in total cholesterol and low density lipoprotein (LDL) An increase in high density lipoprotein (HDL). Lowers blood pressure.")
86
Patient Education: Education is also important in control and management of diabetes. It involves making the patient aware of his disease, its various control measures which include knowledge of hypoglycemic agents as well as the importance of diet.

87
Education of the diabetes involves the following:
Knowledge about the disease – its nature, symptoms and care. The diet – a basic idea about the food values and individual diet plan as well as exchange list. Hypoglycemic agents involved in the control, and dietary management in relation to these agents. Household methods for testing urine for sugar and acetone. Importance of exercise in controlling diabetes and its relation to balance with insulin and food. Skin care and personal hygiene is important for good hygiene and circulation of blood. Personal identification – The need to always carry a personal tag or identity card to identify his name, address, doctor’s name and address, and his emergency needs especially if he is receiving insulin therapy. Emphasize the need to always carry a candy or sugar product at hand.

88
Resistant starch: Most starches are digested and absorbed into the body through the small intestine, but some resist “ digestion and pass to the large intestine where, through fermentation, they are digested. This type of starch is called resistant starch.

89
Types of resistant starch:
Starch that is difficult for the digestive process to reach, often due to a fibrous "shell". Grains and legumes which are cooked intact are an example. Some foods, such as unripe bananas, raw potatoes, and plantains, have a type of starch which our digestive enzymes can't break down. Small amounts of resistant starch (about 5% of the total) are produced when some starchy cooked foods, such as potatoes and rice, are allowed to cool before eating. Manufactured resistant starch, made by various chemical processes. It is not known whether these starches have the same benefits as those in the other three groups.
 are produced when some starchy cooked foods, such as potatoes and rice, are allowed to cool before eating. Manufactured resistant starch, made by various chemical processes. It is not known whether these starches have the same benefits as those in the other three groups.")
90
Benefits of resistant starch :
Dietary fiber intake is increased. Lowering blood glucose levels Resistant starch may help lower cholesterol levels and decrease the risk of cardiovascular disease. Satiety and a sense of fullness increase and may, therefore, help with weight control. Energy fluctuations are minimized. Glycemic levels are more stable and insulin sensitivity increases, while insulin resistance decreases. Promotes “good” bacteria, and suppresses “bad” bacteria and their toxic products. Promotes bowel regularity. Resistant starch in a meal is associated with less fat storage after that meal.

91
Grams of Resistant Starch
Food Serving Size Grams of Resistant Starch Navy Beans ½ cup cooked 9.8 Banana raw 1 medium, peeled 4.7 Cold potato ½” Diameter 3.2 Lentils 2.5 Pearl Barley 1.6 Oatmeal 1 cup cooked 0.7 Whole grain bread 2 slices 0.5 Corn ½ cup 0.3 Split peas 3.1

92
Foods to be avoided Foods to be eaten in moderation only Food to be permitted Simple sugars like: Honey Syrup Glucose Dried fruits Sweets Candies Fried foods Alcohol Nuts Jaggery Sweetened juice Fats Cereals Potato Peas and baked beans Egg Meat Fruits Artificial sweetener Green leafy vegetables Fruits except banana Lemon Clear soups Onion Mint Spices Salads Skimmed and butter milk

93
Glycemic Index: Glycemic index measures how fast a food is likely to raise the blood sugar or is a ranking system for carbohydrates based on their immediate effect on blood glucose The glycemic index was invented originally to help diabetes patients, manage their blood- sugar levels.

94
How to Calculate Glycemic Index of food:
A group of at least 10 healthy individuals are fed 50 g of the carbohydrate being tested and then they have their blood sugar levels tested at regular intervals over a two-hour period. A few days later, the same individuals consume 50 g of pure glucose and have their blood sugar levels tested at the same timed intervals. Each individual's response is calculated by dividing their blood sugar levels after consuming the test food by their blood sugar levels after having pure glucose. Then all of the responses are averaged to determine a food's GI value.

95
Glycemic index = Incremental area under the 2 hour plasma glucose curve after eating 50 g of Carbohydrates from test food x after taking 50 g of Glucose in water

96
The glycemic index separates carbohydrates containing food into three categories:

97
Factor affecting the glycemic index:
Fiber content: Fiber shields the starchy carbohydrates in food from the immediate and rapid attack by digestive enzymes. This slows the release of sugar molecules into the blood stream. Ripeness: ripe fruits and vegetables tend to have more sugar than unripe ones, and so tend to have a higher glycemic index. Type of starch: Starch comes in many different configurations. Some are easier to break into sugar molecules than others.The starch in potatoes, for example, is digested and absorbed into bloodstream quickly. Fat and acid content: The more fat or acid a food contains, the slower its carbohydrates are converted to sugar and absorbed into the bloodstream. Physical form: Finely ground grain is more rapidly digested, and so has a higher glycemic index, than more coarsely ground grain.

98
Glycemic load: Glycemic load determines how much impact of carbohydrate food may have on blood glucose levels, depending on the number of grams of carbohydrate in a serving. Glycemic load: GI x carbohydrate grams/serving. 100 The Glycemic load not only measure the level of glucose in the blood, but also the insulin demand produced by a normal serving of the food.

100
Artificial sweeteners:
An ideal sweetener is as sweet as or sweeter than sucrose, has a pleasant taste with no after taste. It is colorless, odorless, readily soluble, stable, functional and economically feasible. It is also nontoxic, does not promote dental cavities It is either metabolized normally or excreted from the body unchanged without contributing to any metabolic abnormalities. when multiple sweeteners are used together they have a synergistic effect. They improve the product taste and stability.

101
Sale of Artificial Sweeteners:

102
Low – calorie sweeteners:
Polyols: Sugar alcohols ( xylitol, sorbitol, mannitol, maltitol, isomalt) known as polyols. They are white crystalline, slightly hygroscopic, water soluble powders. They are less sweet and 50% of energy of polyols is available to human body. Average caloric value is 2.4 kcal/g. Polyols are suitable for diabetics because rapid glycemic response is avoided. Due to induced digestibility of polyols, their intake should be restricted to g/day for adults and 30g/day for children in order to avoid gastrointestinal discomfort
 known as polyols. They are white crystalline, slightly hygroscopic, water soluble powders. They are less sweet and 50% of energy of polyols is available to human body. Average caloric value is 2.4 kcal/g. Polyols are suitable for diabetics because rapid glycemic response is avoided. Due to induced digestibility of polyols, their intake should be restricted to g/day for adults and 30g/day for children in order to avoid gastrointestinal discomfort.")
103
Non- caloric Sweeteners:
Cyclamate: It is thirty times sweeter than sucrose. It tastes much like sugar and is heat stable. It was banned following a report that some rats receiving very large doses had developed tumors of the urinary bladder. Alitame: It is a depeptide based amide and has a sweet taste similar to sugar. It is more than times sweeter than sucrose.

104
Acelsulfame-K: Acelsulfame-K is a synthetic derivative of acetoacetic acid. It is not metabolized in the body and is excreted unchanged. Acelsulfame-K, the potassium salt of acesulfame is upto 200 times sweeter than a 3 percent sucrose solution and it gives zero calories. It has a clean, fresh taste but it may have a bitter taste when used in large amounts. In mixtures of acelsulfame-k and aspartame (1:1by weight) there is a strong synergistic enhancement of sweetness. Acelsulfame – K is heat stable hence can be used in cooked and baked products.
 there is a strong synergistic enhancement of sweetness. Acelsulfame – K is heat stable hence can be used in cooked and baked products.")
105
Aspartame: It is made by combing two amino acids- Aspartic acid and phenylalnine and adding methyl alcohol to form a methyl ester. Aspartame is a white, odourless, crystalline powder that has a sugar like taste and sweetness potency 180 to 200 times that of sucrose without any bitter aftertaste. It is not stable to heat and changes chemically and loses sweetness. It contain 4 kcal/g but because of its intense sweeetening ability provides negligible calories. Aspartame actual daily intake in persons with diabetes is 2 to 4 mg/kg of body weight daily. It does not alter glycemic control and is metabolized in the gastrointestinal tract.

106
Saccharin: It is sodium ortho benzene sulphonamide or the calcium salt. It is 300 times sweeter than sucrose. It is stable in a wide variety of products under extreme processing conditions it can be synthesized with relatively few impurities and is inexpensive. It gives bitter after taste at higher concentration. But when used in combination with aspartame or cyclamate, sweetness is enhanced and bitterness is decreased. It does not contribute calories.

107
Sucrolose: It is a white crystalline solid produced by the selective addition of chlorine atoms to sucrose. It is 600 times sweeter than sugar and no bitter aftertaste. It is very soluble in water and stable at high temperatures and therefore can be used in baked goods. Sucrolose does not interact with any other food components.

108
Soft drinks contribute to artificial sweetener.
Excessive intake of any sweetener requires individual counseling which will take into consideration the factors of any other sweetener used, the overall diet, and its nutritional adequacy. Use of sweeteners by a diabetic patient is not encouraged as it does not help the patient to wean away from sweet foods.

109
Relative Sweetness of sugars and Artificial sweeteners:
Substance Sweetness value ( as compared to sucrose) Natural Sweeteners: Fructose 173 Sucrose 100 Glucose 74 Sorbitol 60 Mannitol 50 Artificial Sweeteners: Cyclamate 30 Aspartame 180 Acesulfame – K 200 Saccharin 300 Sucralose 600 Alitame 2000
 Natural Sweeteners: Fructose Sucrose Glucose. 74. Sorbitol. 60. Mannitol. 50. Artificial Sweeteners: Cyclamate. 30. Aspartame Acesulfame – K Saccharin Sucralose Alitame")
110
Reference: Kumud khanna, nutrition and Dietetics
Davidson, passmore, Human Nutrition and Dietetics Anita, F.P., clinical Dietetics and Nutrition Krause’s, food Nutrition and Diet Therapy, 10th Edition Rajalakshmi, Applied Nurtition x 26 type 2 diabetes. html html.com . Info/encylopedia/islets of langerhens. html India. Com / diabetes/educational/dm- metabolic. Insulin home. html. Com Com / formula for life/ body fat.html of hope.com/ medical / pancreas-html www. Diabetes.com/product. html

Similar presentations




















 in the liver and muscles and quickly converted back.>")

 Diabetes Mellitus.>")
