Download presentation
Presentation is loading. Please wait.

2
Prognostic Value of Programmed Electrical Stimulation Among Implantable Cardioverter-Defibrillator Recipients Real-World Data from the Israeli National ICD Registry Jorge E. Schliamser MD, Guy Amit MD, Moti Haim MD, Mahmoud Suleiman MD, Arie Militianu MD, Nissan Ben Dov MD, Aharon Glick MD, Vladimir Khalameizer MD, Natalie Gavrielov-Yusim MSc, Ilan Goldenberg MD, Michael Glikson, MD On Behalf of the Israeli Working Group on Pacing and Electrophysiology Jorge E. Schliamser MD, Guy Amit MD, Moti Haim MD, Mahmoud Suleiman MD, Arie Militianu MD, Nissan Ben Dov MD, Aharon Glick MD, Vladimir Khalameizer MD, Natalie Gavrielov-Yusim MSc, Ilan Goldenberg MD, Michael Glikson, MD On Behalf of the Israeli Working Group on Pacing and Electrophysiology

3
DisclosureDisclosure The study was supported by an unrestricted research grant from Boston Scientific to the Israeli Heart Society and the Israeli Association for Cardiovascular Trials The study was supported by an unrestricted research grant from Boston Scientific to the Israeli Heart Society and the Israeli Association for Cardiovascular Trials

4
BackgroundBackground Inducibility of ventricular arrhythmias with programmed electrical stimulation (PES) suggests an increased risk for sudden arrhythmic death Inducibility of ventricular arrhythmias with programmed electrical stimulation (PES) suggests an increased risk for sudden arrhythmic death MADIT I, MUSTT, MADIT II, DEFINITE Inducibility of ventricular arrhythmias with programmed electrical stimulation (PES) suggests an increased risk for sudden arrhythmic death Inducibility of ventricular arrhythmias with programmed electrical stimulation (PES) suggests an increased risk for sudden arrhythmic death MADIT I, MUSTT, MADIT II, DEFINITE
 suggests an increased risk for sudden arrhythmic death Inducibility of ventricular arrhythmias with programmed electrical stimulation (PES) suggests an increased risk for sudden arrhythmic death MADIT I, MUSTT, MADIT II, DEFINITE Inducibility of ventricular arrhythmias with programmed electrical stimulation (PES) suggests an increased risk for sudden arrhythmic death Inducibility of ventricular arrhythmias with programmed electrical stimulation (PES) suggests an increased risk for sudden arrhythmic death MADIT I, MUSTT, MADIT II, DEFINITE")
5
BackgroundBackground While earlier trials used PES for risk stratification of SCD, mainly in patients with coronary artery disease, recent data from RCTs, support a benefit of ICDs in patients with reduced LVEF without performing PES While earlier trials used PES for risk stratification of SCD, mainly in patients with coronary artery disease, recent data from RCTs, support a benefit of ICDs in patients with reduced LVEF without performing PES MADIT II, SCDHeFT While earlier trials used PES for risk stratification of SCD, mainly in patients with coronary artery disease, recent data from RCTs, support a benefit of ICDs in patients with reduced LVEF without performing PES While earlier trials used PES for risk stratification of SCD, mainly in patients with coronary artery disease, recent data from RCTs, support a benefit of ICDs in patients with reduced LVEF without performing PES MADIT II, SCDHeFT

6
PurposePurpose To evaluate the clinical characteristics and outcomes of patients enrolled in the Israeli National ICD Registry who underwent PES prior to device implantation To evaluate the clinical characteristics and outcomes of patients enrolled in the Israeli National ICD Registry who underwent PES prior to device implantation

7
Study Population Non inducible patients who did not receive a device, were not included in the registry Non inducible patients who did not receive a device, were not included in the registry 1188 registry patients (age 66.2±10.9, 89% male) who underwent device implantation were prospectively followed for a median period of 323 days 1188 registry patients (age 66.2±10.9, 89% male) who underwent device implantation were prospectively followed for a median period of 323 days Non inducible patients who did not receive a device, were not included in the registry Non inducible patients who did not receive a device, were not included in the registry 1188 registry patients (age 66.2±10.9, 89% male) who underwent device implantation were prospectively followed for a median period of 323 days 1188 registry patients (age 66.2±10.9, 89% male) who underwent device implantation were prospectively followed for a median period of 323 days
 who underwent device implantation were prospectively followed for a median period of 323 days 1188 registry patients (age 66.2±10.9, 89% male) who underwent device implantation were prospectively followed for a median period of 323 days Non inducible patients who did not receive a device, were not included in the registry Non inducible patients who did not receive a device, were not included in the registry 1188 registry patients (age 66.2±10.9, 89% male) who underwent device implantation were prospectively followed for a median period of 323 days 1188 registry patients (age 66.2±10.9, 89% male) who underwent device implantation were prospectively followed for a median period of 323 days")
8
Programmed Electrical Stimulation No particular PES protocol was adopted No particular PES protocol was adopted Inducibility was reported by the implanting physician if monomorphic/polymorphic VT or VF was obtained at PES Inducibility was reported by the implanting physician if monomorphic/polymorphic VT or VF was obtained at PES No particular PES protocol was adopted No particular PES protocol was adopted Inducibility was reported by the implanting physician if monomorphic/polymorphic VT or VF was obtained at PES Inducibility was reported by the implanting physician if monomorphic/polymorphic VT or VF was obtained at PES

9
OutcomesOutcomes First occurrence of appropriate ICD therapy for VT/VF and/or death

10
Arrhythmic Events Arrhythmic events were defined as ICD shocks or anti-tachycardia pacing for ventricular tachycardia or fibrillation (VT/VF) Arrhythmic events were defined as ICD shocks or anti-tachycardia pacing for ventricular tachycardia or fibrillation (VT/VF) Detection and therapy programming was up to the physician’s discretion Detection and therapy programming was up to the physician’s discretion Arrhythmic events were defined as ICD shocks or anti-tachycardia pacing for ventricular tachycardia or fibrillation (VT/VF) Arrhythmic events were defined as ICD shocks or anti-tachycardia pacing for ventricular tachycardia or fibrillation (VT/VF) Detection and therapy programming was up to the physician’s discretion Detection and therapy programming was up to the physician’s discretion
 Arrhythmic events were defined as ICD shocks or anti-tachycardia pacing for ventricular tachycardia or fibrillation (VT/VF) Detection and therapy programming was up to the physician’s discretion Detection and therapy programming was up to the physician’s discretion Arrhythmic events were defined as ICD shocks or anti-tachycardia pacing for ventricular tachycardia or fibrillation (VT/VF) Arrhythmic events were defined as ICD shocks or anti-tachycardia pacing for ventricular tachycardia or fibrillation (VT/VF) Detection and therapy programming was up to the physician’s discretion Detection and therapy programming was up to the physician’s discretion")
11
ResultsResults Of 2971 patients undergoing ICD implantation, 504 (17%) patients had PES prior to ICD implantation Of 2971 patients undergoing ICD implantation, 504 (17%) patients had PES prior to ICD implantation 413/504 (82%) patients belong to the primary prevention group 413/504 (82%) patients belong to the primary prevention group Among patients who underwent PES, 460 (91%) were inducible for VT/VF Among patients who underwent PES, 460 (91%) were inducible for VT/VF Of 2971 patients undergoing ICD implantation, 504 (17%) patients had PES prior to ICD implantation Of 2971 patients undergoing ICD implantation, 504 (17%) patients had PES prior to ICD implantation 413/504 (82%) patients belong to the primary prevention group 413/504 (82%) patients belong to the primary prevention group Among patients who underwent PES, 460 (91%) were inducible for VT/VF Among patients who underwent PES, 460 (91%) were inducible for VT/VF
 patients had PES prior to ICD implantation Of 2971 patients undergoing ICD implantation, 504 (17%) patients had PES prior to ICD implantation 413/504 (82%) patients belong to the primary prevention group 413/504 (82%) patients belong to the primary prevention group Among patients who underwent PES, 460 (91%) were inducible for VT/VF Among patients who underwent PES, 460 (91%) were inducible for VT/VF Of 2971 patients undergoing ICD implantation, 504 (17%) patients had PES prior to ICD implantation Of 2971 patients undergoing ICD implantation, 504 (17%) patients had PES prior to ICD implantation 413/504 (82%) patients belong to the primary prevention group 413/504 (82%) patients belong to the primary prevention group Among patients who underwent PES, 460 (91%) were inducible for VT/VF Among patients who underwent PES, 460 (91%) were inducible for VT/VF")
12
Baseline Clinical Characteristics

13
Factors Independently Associated with the Performance of PES

14
Baseline Clinical Characteristics Thus, a lower baseline NYHA class, a higher baseline left ventricular ejection fraction (LVEF), lack of atrial fibrillation, and lack of treatment with diuretics were all independently associated with the performance of PES among registry patients, suggesting that patients selected for this procedure had less advanced heart failure Thus, a lower baseline NYHA class, a higher baseline left ventricular ejection fraction (LVEF), lack of atrial fibrillation, and lack of treatment with diuretics were all independently associated with the performance of PES among registry patients, suggesting that patients selected for this procedure had less advanced heart failure
, lack of atrial fibrillation, and lack of treatment with diuretics were all independently associated with the performance of PES among registry patients, suggesting that patients selected for this procedure had less advanced heart failure Thus, a lower baseline NYHA class, a higher baseline left ventricular ejection fraction (LVEF), lack of atrial fibrillation, and lack of treatment with diuretics were all independently associated with the performance of PES among registry patients, suggesting that patients selected for this procedure had less advanced heart failure")
15
Why Lower Risk Patients? Mainly, due to the need to proof pre- implantion inducibility in case of borderline clinical characteristics, as mandated by the major Israeli Health Care Provider (Clalit Health Services) Mainly, due to the need to proof pre- implantion inducibility in case of borderline clinical characteristics, as mandated by the major Israeli Health Care Provider (Clalit Health Services)
 Mainly, due to the need to proof pre- implantion inducibility in case of borderline clinical characteristics, as mandated by the major Israeli Health Care Provider (Clalit Health Services).")
16
Clinical Outcomes by Performance of PES Clinical Outcomes by Performance of PES Among 1188 registry patients with available follow-up (positive PES 15%, no PES 76%) the rate of appropriate ICD therapy for VT/VF was similar between patients with a positive PES and those who underwent device implantation on the basis of LVEF alone Among 1188 registry patients with available follow-up (positive PES 15%, no PES 76%) the rate of appropriate ICD therapy for VT/VF was similar between patients with a positive PES and those who underwent device implantation on the basis of LVEF alone Regardless of non inducibility at PES, 9% of patients still received a device Regardless of non inducibility at PES, 9% of patients still received a device Among 1188 registry patients with available follow-up (positive PES 15%, no PES 76%) the rate of appropriate ICD therapy for VT/VF was similar between patients with a positive PES and those who underwent device implantation on the basis of LVEF alone Among 1188 registry patients with available follow-up (positive PES 15%, no PES 76%) the rate of appropriate ICD therapy for VT/VF was similar between patients with a positive PES and those who underwent device implantation on the basis of LVEF alone Regardless of non inducibility at PES, 9% of patients still received a device Regardless of non inducibility at PES, 9% of patients still received a device
 the rate of appropriate ICD therapy for VT/VF was similar between patients with a positive PES and those who underwent device implantation on the basis of LVEF alone Among 1188 registry patients with available follow-up (positive PES 15%, no PES 76%) the rate of appropriate ICD therapy for VT/VF was similar between patients with a positive PES and those who underwent device implantation on the basis of LVEF alone Regardless of non inducibility at PES, 9% of patients still received a device Regardless of non inducibility at PES, 9% of patients still received a device Among 1188 registry patients with available follow-up (positive PES 15%, no PES 76%) the rate of appropriate ICD therapy for VT/VF was similar between patients with a positive PES and those who underwent device implantation on the basis of LVEF alone Among 1188 registry patients with available follow-up (positive PES 15%, no PES 76%) the rate of appropriate ICD therapy for VT/VF was similar between patients with a positive PES and those who underwent device implantation on the basis of LVEF alone Regardless of non inducibility at PES, 9% of patients still received a device Regardless of non inducibility at PES, 9% of patients still received a device")
17
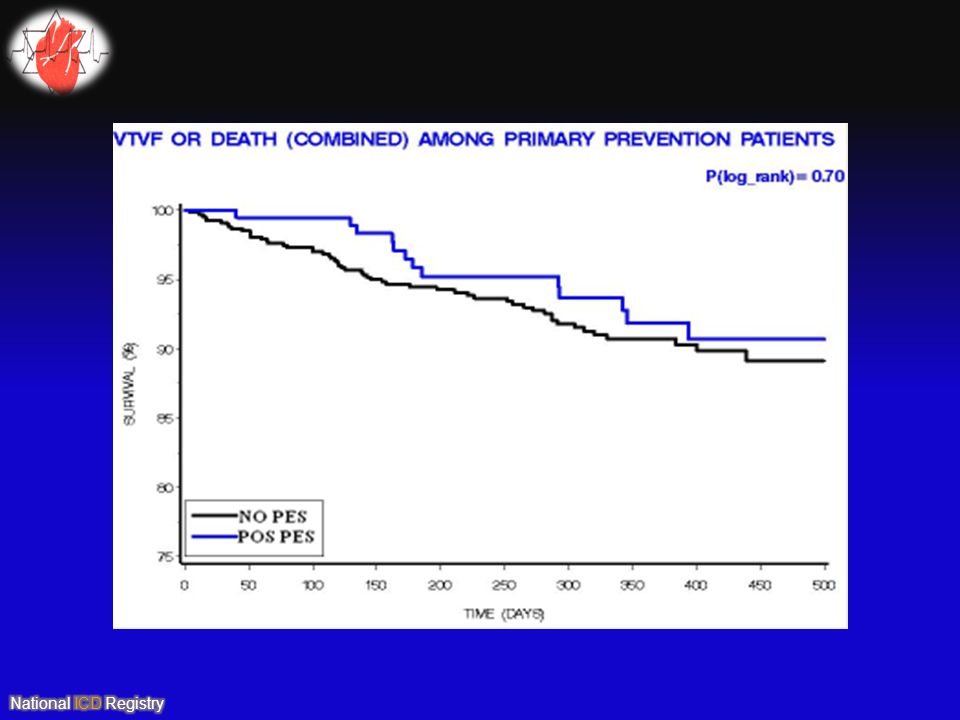
Clinical Outcomes by Performance of PES Clinical Outcomes by Performance of PES The cumulative probability of VT/VF was 7% among patients with a positive PES prior to ICD implantation and 8% among patients in whom PES was not performed prior to device implantation, log-rank p-value=0.92 The cumulative probability of VT/VF was 7% among patients with a positive PES prior to ICD implantation and 8% among patients in whom PES was not performed prior to device implantation, log-rank p-value=0.92 Consistently, multivariate analysis showed similar VT/VF risk between the 2 groups (HR=0.95 [95%CI 0.71 – 1.28]; p=0.49) after adjustment for age, gender, type of prevention, NYHA, and LVEF Consistently, multivariate analysis showed similar VT/VF risk between the 2 groups (HR=0.95 [95%CI 0.71 – 1.28]; p=0.49) after adjustment for age, gender, type of prevention, NYHA, and LVEF The cumulative probability of VT/VF was 7% among patients with a positive PES prior to ICD implantation and 8% among patients in whom PES was not performed prior to device implantation, log-rank p-value=0.92 The cumulative probability of VT/VF was 7% among patients with a positive PES prior to ICD implantation and 8% among patients in whom PES was not performed prior to device implantation, log-rank p-value=0.92 Consistently, multivariate analysis showed similar VT/VF risk between the 2 groups (HR=0.95 [95%CI 0.71 – 1.28]; p=0.49) after adjustment for age, gender, type of prevention, NYHA, and LVEF Consistently, multivariate analysis showed similar VT/VF risk between the 2 groups (HR=0.95 [95%CI 0.71 – 1.28]; p=0.49) after adjustment for age, gender, type of prevention, NYHA, and LVEF
![Clinical Outcomes by Performance of PES Clinical Outcomes by Performance of PES The cumulative probability of VT/VF was 7% among patients with a positive PES prior to ICD implantation and 8% among patients in whom PES was not performed prior to device implantation, log-rank p-value=0.92 The cumulative probability of VT/VF was 7% among patients with a positive PES prior to ICD implantation and 8% among patients in whom PES was not performed prior to device implantation, log-rank p-value=0.92 Consistently, multivariate analysis showed similar VT/VF risk between the 2 groups (HR=0.95 [95%CI 0.71 – 1.28]; p=0.49) after adjustment for age, gender, type of prevention, NYHA, and LVEF Consistently, multivariate analysis showed similar VT/VF risk between the 2 groups (HR=0.95 [95%CI 0.71 – 1.28]; p=0.49) after adjustment for age, gender, type of prevention, NYHA, and LVEF The cumulative probability of VT/VF was 7% among patients with a positive PES prior to ICD implantation and 8% among patients in whom PES was not performed prior to device implantation, log-rank p-value=0.92 The cumulative probability of VT/VF was 7% among patients with a positive PES prior to ICD implantation and 8% among patients in whom PES was not performed prior to device implantation, log-rank p-value=0.92 Consistently, multivariate analysis showed similar VT/VF risk between the 2 groups (HR=0.95 [95%CI 0.71 – 1.28]; p=0.49) after adjustment for age, gender, type of prevention, NYHA, and LVEF Consistently, multivariate analysis showed similar VT/VF risk between the 2 groups (HR=0.95 [95%CI 0.71 – 1.28]; p=0.49) after adjustment for age, gender, type of prevention, NYHA, and LVEF](http://images.slideplayer.com/19/5731950/slides/slide_17.jpg "Clinical Outcomes by Performance of PES Clinical Outcomes by Performance of PES The cumulative probability of VT/VF was 7% among patients with a positive PES prior to ICD implantation and 8% among patients in whom PES was not performed prior to device implantation, log-rank p-value=0.92 The cumulative probability of VT/VF was 7% among patients with a positive PES prior to ICD implantation and 8% among patients in whom PES was not performed prior to device implantation, log-rank p-value=0.92 Consistently, multivariate analysis showed similar VT/VF risk between the 2 groups (HR=0.95 [95%CI 0.71 – 1.28]; p=0.49) after adjustment for age, gender, type of prevention, NYHA, and LVEF Consistently, multivariate analysis showed similar VT/VF risk between the 2 groups (HR=0.95 [95%CI 0.71 – 1.28]; p=0.49) after adjustment for age, gender, type of prevention, NYHA, and LVEF The cumulative probability of VT/VF was 7% among patients with a positive PES prior to ICD implantation and 8% among patients in whom PES was not performed prior to device implantation, log-rank p-value=0.92 The cumulative probability of VT/VF was 7% among patients with a positive PES prior to ICD implantation and 8% among patients in whom PES was not performed prior to device implantation, log-rank p-value=0.92 Consistently, multivariate analysis showed similar VT/VF risk between the 2 groups (HR=0.95 [95%CI 0.71 – 1.28]; p=0.49) after adjustment for age, gender, type of prevention, NYHA, and LVEF Consistently, multivariate analysis showed similar VT/VF risk between the 2 groups (HR=0.95 [95%CI 0.71 – 1.28]; p=0.49) after adjustment for age, gender, type of prevention, NYHA, and LVEF")
18
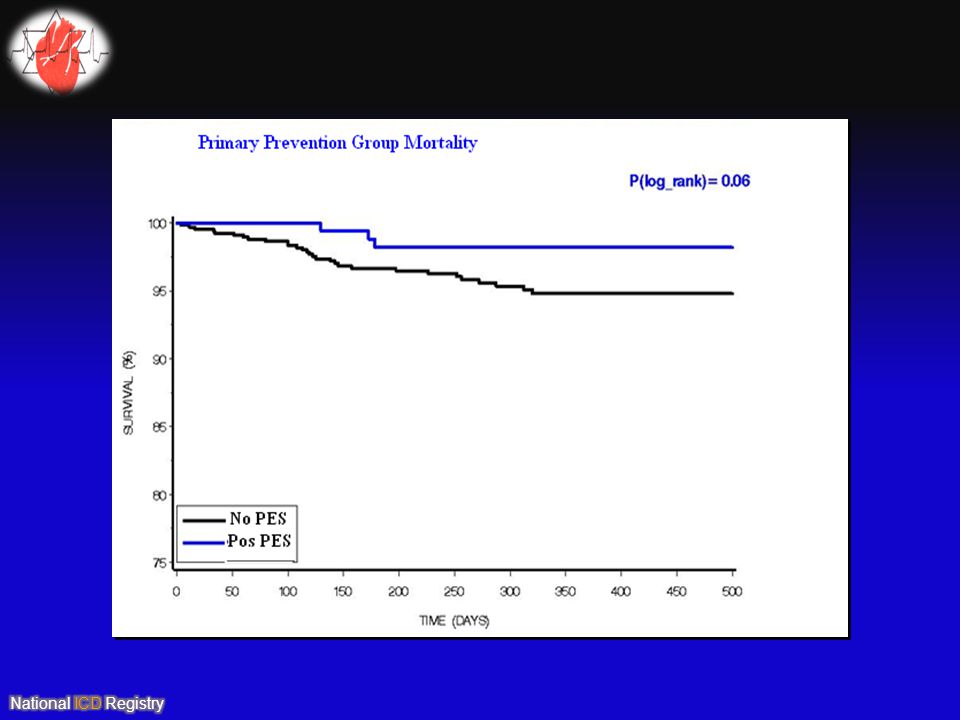
What About Primary Prevention? What About Primary Prevention?

22
ConclusionsConclusions

23
LimitationsLimitations Registry and not a randomized clinical trial Registry and not a randomized clinical trial Relatively short follow-up period Relatively short follow-up period PES has a low positive predictive value and a higher negative predictive value, and in fact, one of the study limitations is that the outcome of an indeterminate number of non-inducible patients in whom a device was not implanted and as a consequence not included in the registry, remains unknown, thereby, the net benefit of performing PES prior to implantation remains unascertained for this cohort and is beyond the scope of this analysis PES has a low positive predictive value and a higher negative predictive value, and in fact, one of the study limitations is that the outcome of an indeterminate number of non-inducible patients in whom a device was not implanted and as a consequence not included in the registry, remains unknown, thereby, the net benefit of performing PES prior to implantation remains unascertained for this cohort and is beyond the scope of this analysis Registry and not a randomized clinical trial Registry and not a randomized clinical trial Relatively short follow-up period Relatively short follow-up period PES has a low positive predictive value and a higher negative predictive value, and in fact, one of the study limitations is that the outcome of an indeterminate number of non-inducible patients in whom a device was not implanted and as a consequence not included in the registry, remains unknown, thereby, the net benefit of performing PES prior to implantation remains unascertained for this cohort and is beyond the scope of this analysis PES has a low positive predictive value and a higher negative predictive value, and in fact, one of the study limitations is that the outcome of an indeterminate number of non-inducible patients in whom a device was not implanted and as a consequence not included in the registry, remains unknown, thereby, the net benefit of performing PES prior to implantation remains unascertained for this cohort and is beyond the scope of this analysis

24
THANK YOU FOR YOUR ATTENTION

Similar presentations





 Arthur J. Moss, MD for the MADIT-RIT Executive Committee AHA Late Breaking Trials November.>")



>")






 Implantation indications and outcomes Guy Amit, MD; Mahmoud Suleiman, MD; Mark Kazatsker,>")


