Download presentation
Presentation is loading. Please wait.

1
Significance of HLA in Transfusion and Transplantation
Terry Aly Clinical Pathology Conference February 8, 2008

2
Main Topics HLA System Overview HLA and Transfusion
Alloimmunization Refractoriness to platelets Graft rejection Transfusion-Associated Graft-Versus-Host Disease (TA-GVHD) Transfusion-Related Acute Lung Injury (TRALI) HLA and Transplantation Bone marrow Cord blood Solid organ
 Transfusion-Related Acute Lung Injury (TRALI) HLA and Transplantation. Bone marrow. Cord blood. Solid organ.")
3
The Human Leukocyte Antigen (HLA) System
Essential to immune function: HLA molecules present peptide antigens to the immune system (T-cells) Important for self versus non-self distinction
 Important for self versus non-self distinction.")
4
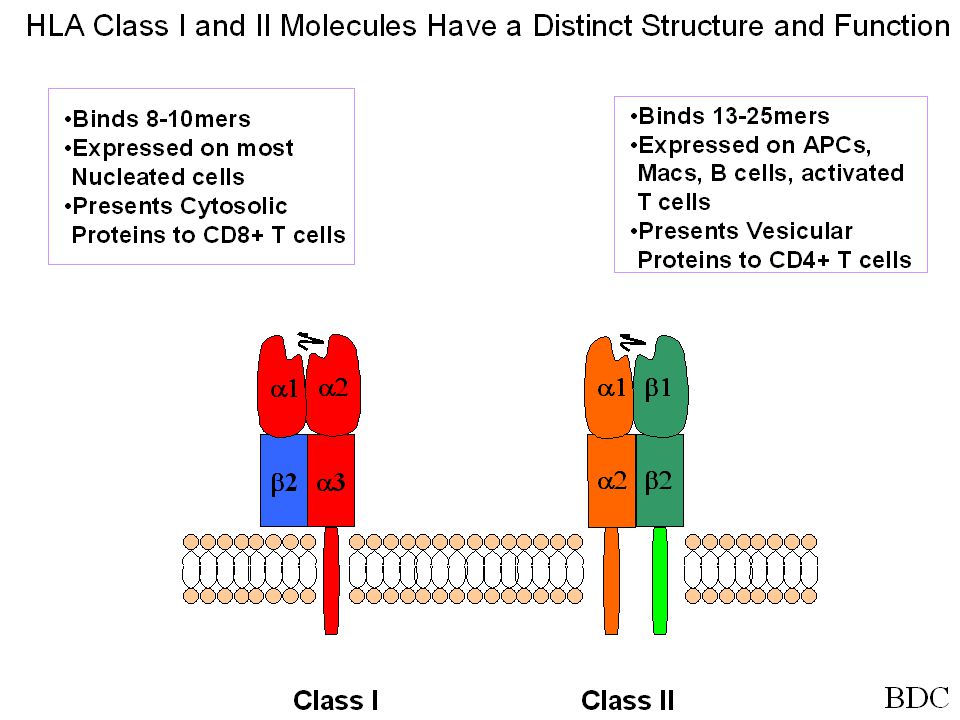
HLA Class I Monitors Inside of the Cell
Tapasin CR CN The MHC class I and class II molecules present antigens from different sources. Class I molecules present intracellular antigens that are processed in the cytoplasm and pumped into the endoplasmic reticulum, where new HLA molecules are being assembled. Processing of the antigens is performed by the proteosome, a multimeric enzyme composed of 28 subunits. Two subunits are encoded by the LMP genes found within the HLA region of the chromosome. The subunits may change in response to IFN-. LMP2, LMP7 and a third component, MECL-1, are induced by IFN- and displace the constitutive components and favor the processing of new peptides, thus insuring that newly synthesized viral proteins will be amply represented on the cell surface. The proteosome also favors the cleavage of proteins into 8-10 amino acids with hydrophobic or basic carboxy termini that fit nicely into the peptide binding groove of the HLA molecule. Peptides that are processed in this manner are transported into the endoplasmic reticulum by TAP (transporter associated with antigen), which is comprised of two subunits, TAP-1 and TAP-2. TAP-2 as an ATP binding site, which regulates the active transport of peptides into the lumen of the ER. The TAP transporter has some specificity, preferring peptides of >8 amino acids with hydrophobic or basic amino acids at the carboxy terminus. This is the preferred peptide for binding in the MHC groove. The newly synthesized HLA molecule is maintained in a partially folded conformation by calnexin (not shown). When 2-microglobulin binds to the HLA molecule, the complex dissociates from calnexin and binds a complex of calreticulin and tapasin, which then bind to TAP-1. The proper binding of a peptide to the HLA molecule dissociates the complex, and the HLA molecule is then transported through the Golgi complex to the cell surface. Dr. Brian Freed
, which is comprised of two subunits, TAP-1 and TAP-2. TAP-2 as an ATP binding site, which regulates the active transport of peptides into the lumen of the ER. The TAP transporter has some specificity, preferring peptides of >8 amino acids with hydrophobic or basic amino acids at the carboxy terminus. This is the preferred peptide for binding in the MHC groove. The newly synthesized HLA molecule is maintained in a partially folded conformation by calnexin (not shown). When 2-microglobulin binds to the HLA molecule, the complex dissociates from calnexin and binds a complex of calreticulin and tapasin, which then bind to TAP-1. The proper binding of a peptide to the HLA molecule dissociates the complex, and the HLA molecule is then transported through the Golgi complex to the cell surface. Dr. Brian Freed.")
5
HLA Class II Monitors Outside of Cell
Peptides Extra-cellular Proteins DM monitors peptide specificity for DR The presentation of peptides on MHC class II molecules is quite different. HLA-DR and related class II molecules are also assembled in the endoplasmic reticulum, but the associate with a third protein known as the invariant chain, which prevents peptide binding. The invariant chain is processed within endosomes to CLIP (class II-associated invariant chain peptide). In the presence of HLA-DM molecules, CLIP dissociates from HLA-DR or DQ molecules and allows binding of new peptides that have been endocytosed from the extracellular environment. Thus, MHC class II molecules differ from MHC class I molecules in that they preferentially present extracellular antigens rather intracellular ones. HLA-DM serves to ‘edit’ peptide binding, promoting association with high affinity peptides over lower affinity peptides. DM Dr. Brian Freed
. In the presence of HLA-DM molecules, CLIP dissociates from HLA-DR or DQ molecules and allows binding of new peptides that have been endocytosed from the extracellular environment. Thus, MHC class II molecules differ from MHC class I molecules in that they preferentially present extracellular antigens rather intracellular ones. HLA-DM serves to ‘edit’ peptide binding, promoting association with high affinity peptides over lower affinity peptides. DM. Dr. Brian Freed.")
7
Antigen–presenting cells (APCs):
monocytes, macrophages, dendritic cells, B cells Teaching slides:

8
Humoral Versus Cellular Immune Response

9
Class I (1.1 Mb) Class II (2.2 Mb)
Class III (0.7 Mb) Complement & cytokines Class II (2.2 Mb)
 Complement. & cytokines. Class II (2.2 Mb)")
10
HLA Genetic Nomenclature
Gene low high resolution typing “subtype”=01 Allele: HLA-DRB1*0401 Haplotype: HLA-DRB1*0401 HLA-DQB1*0302 HLA-DRB1*0301 HLA-DQB1*0201 DRB1*02 Genotype: HLA-DRB1*04 HLA-DQB1*0302 J. Noble

11
Why care about HLA type for transfusions?
Alloimmunization with increased risk for platelet refractoriness and humoral transplant rejection Recipient can make antibody against donor HLA antigen, most common Transfusion-Related Acute Lung Injury donor HLA antibodies react against recipient antigens Transfusion-Associated Graft-Vs-Host Disease

12
Alloimmunization Alloimmunization: Development of antibodies after exposure to non-self human antigen HLA on leukocytes or platelet specific antigens May occur with transfusions (PRBC>platelet because PRBC contain more leukocytes), pregnancies, or transplants
, pregnancies, or transplants.")
13
Antigen exposure associated with leukocytes in
transfusion, pregnancy, or transplantation Alloimmunization Resolves Spontaneously (Transfusion Ab resolve more than pregnancy Ab) Refractoriness to platelets* Humoral transplant rejection *Antibodies can react with Class I HLA (most common), ABH antigens, or platelet antigens that exist on surface of platelets
 Refractoriness. to platelets* Humoral. transplant. rejection. *Antibodies can react with Class I HLA (most common), ABH antigens, or platelet antigens that exist on surface of platelets.")
14
How to prevent alloimmunization
How to prevent alloimmunization? Trial to Reduce Alloimmunization to Platelets (TRAP) study Leukoreduction (LR) effect Removes 99.9% of leukocytes, leaving < 5*106 per unit Only 19% of AML patients receiving leukoreduced platelets developed lymphocytotoxic antibodies vs. 45%* receiving unmodified platelets *alloimmunization rate likely higher: current methods detect more alloantibodies than previously The Trial to Reduce Alloimmunization to Platelets Study Group. N Engl J Med
 study. Leukoreduction (LR) effect. Removes 99.9% of leukocytes, leaving < 5*106 per unit. Only 19% of AML patients receiving leukoreduced platelets developed lymphocytotoxic antibodies vs. 45%* receiving unmodified platelets. *alloimmunization rate likely higher: current methods detect more alloantibodies than previously. The Trial to Reduce Alloimmunization to Platelets Study Group. N Engl J Med")
15
How to prevent alloimmunization?
UV irradiation was equally effective in TRAP study (prevents lymphocytes from proliferating or stimulating), but blood banks typically use Gamma instead of UV b/c can penetrate plastic bags LR or irradiation decreased alloimmunization from 13% to 3-4% in previously unexposed patients The Trial to Reduce Alloimmunization to Platelets Study Group. N Engl J Med
, but blood banks typically use Gamma instead of UV b/c can penetrate plastic bags. LR or irradiation decreased alloimmunization from 13% to 3-4% in previously unexposed patients. The Trial to Reduce Alloimmunization to Platelets Study Group. N Engl J Med")
16
UVB-PC: UV B-irradiated, pooled platelet concentrates, random donors
F-PC: Filtered pooled platelet concentrates, random donors F-AP: Filtered apheresis, single random donor 16% 10% 8% Leukocyte reduction and ultraviolet B irradiation of platelets to prevent alloimmunization and refractoriness to platelet transfusions. The Trial to Reduce Alloimmunization to Platelets Study Group. N Engl J Med

17
Who needs alloimmunization prevention?
Give LR or irradiated blood products to patients who are: chronically transfused (20-70% become refractory) immunoincompetent pre- and post-transplant All transplant patients? Include kidney? Time-frame? everyone??
 immunoincompetent. pre- and post-transplant. All transplant patients Include kidney Time-frame everyone")
18
Prestorage Universal Leukoreduction in Canada
Universal prestorage leukoreduction (ULR) of red cell and platelet products has been performed in Canada since August 1999 (and UK too) Seftel MD, Growe GH, Petraszko T, et al. Universal prestorage leukoreduction in Canada decreases platelet alloimmunization and refractoriness. Blood Jan 1;103(1):333-9.
 of red cell and platelet products has been performed in Canada since August 1999 (and UK too) Seftel MD, Growe GH, Petraszko T, et al. Universal prestorage. leukoreduction in Canada decreases platelet alloimmunization and. refractoriness. Blood Jan 1;103(1):")
19
Prestorage Universal Leukoreduction (ULR)—Canada study
Retrospective analysis of 13,902 platelet transfusions in 617 patients undergoing chemotherapy for ALL or stem cell transplantation before (n=315) and after (n=302) ULR instituted Alloimmunization was significantly reduced (19% to 7%, P <.001) in the post-ULR group. Alloimmune platelet refractoriness was similarly reduced (14% to 4%, P <.001).
 and after (n=302) ULR instituted. Alloimmunization was significantly reduced (19% to 7%, P <.001) in the post-ULR group. Alloimmune platelet refractoriness was similarly reduced (14% to 4%, P <.001).")
20
Prestorage Universal Leukoreduction (ULR)—UK study
ULR reduced TA-GVHD rate in immunocompetent individuals from 13 prior to ULR to 0 after ULR ULR reduced post-transfusion purpura rate from 10.3 per year to 2.3 per year Alloimmunization was significantly reduced (19% to 7%, P <.001) in the post-ULR group. Alloimmune platelet refractoriness was similarly reduced (14% to 4%, P <.001).
 in the post-ULR group. Alloimmune platelet refractoriness was similarly reduced (14% to 4%, P <.001).")
21
Refractoriness Repeated failure to achieve the expected increment in platelet count after 2 or more platelet transfusions % Maximum increment = ([pretransfusion count – posttransfusion count in platelets/µL] X blood volume in mL) ÷ (number of platelets transfused, ie, number of U X 6 X 105) Slichter SJ. Evidence-Based Platelet Transfusion Guidelines Hematology 2007
 ÷ (number of platelets transfused, ie, number of U X 6 X 105) Slichter SJ. Evidence-Based Platelet Transfusion Guidelines Hematology")
22
Refractoriness Can be due to:
Alloimmunization to HLA or platelet antigen ABO mismatch Non-immune factors such as insufficient dosing, poor platelet quality, hypersplenism, accelerated consumption, sepsis, DIC, GVHD, and bleeding Slichter SJ. Evidence-Based Platelet Transfusion Guidelines Hematology 2007

23
Management of Refractoriness
Stage 1: Check dosing Stage II: Try ABO matched platelets <48 hours old Stage III: If urgent, give cross-matched platelets. Screen for anti-HLA and anti-platelet antibodies Antibody-mediated or not? Solid-phase assay HLA antibody mediated or not? Panel reactive antibody (PRA) as general screen for HLA Ab positivity. If positive, single antigen testing with microparticle beads to ID which antigen(s) to avoid in donors Slichter SJ. Evidence-Based Platelet Transfusion Guidelines Hematology 2007
 as general screen for HLA Ab positivity. If positive, single antigen testing with microparticle beads to ID which antigen(s) to avoid in donors. Slichter SJ. Evidence-Based Platelet Transfusion Guidelines Hematology")
24
ABO matching prevents platelet refractoriness
Table 1 -- Refractoriness and alloimmunization rates after transfusing ABO matched versus mismatched platelets New antibodies Platelet transfusions Enrolled Female patients Possible prior sensitization[a] Platelet transfusions[b] Platelet refractoriness[c] Anti A/B[d] Anti-HLA Platelet-specific ABO matched 13 10 (77%) 9 (69%) 7 (5–9) 1 (8%) ABO mismatched 2 (15%) 4 (31%) 9 (4–30) 7 (54%) 5 (38%) P value 0.001 Data from Carr R, Hutton JL, Jenkins JA, et al. Transfusion of ABO-mismatched platelets leads to early platelet refractoriness. Br J Haematol 1990;75:408–13
 9 (69%) 7 (5–9) 1 (8%) ABO mismatched. 2 (15%) 4 (31%) 9 (4–30) 7 (54%) 5 (38%) P value Data from Carr R, Hutton JL, Jenkins JA, et al. Transfusion of ABO-mismatched platelets leads to early platelet refractoriness. Br J Haematol 1990;75:408–13.")
25
Problems with HLA Typing and Matching
HLA matching requires the availability of large numbers of HLA-typed donors. A registry of about 18 000–25 000 HLA-typed people is needed to provide at least five HLA-A and HLA-B matched donors for 80% of white patients. HLA-matched platelets requires the recruitment of specific donors, such platelets can only be obtained by apheresis Expensive K Takahashi, T Juji and H Miyazaki, Determination of an appropriate size of unrelated donor pool to be registered for HLA-matched platelet transfusion, Transfusion, 1987.

26
Problem with cross-matching to find compatible platelets
Limited to units available for testing 5 day life to platelets, future transfusions will require re-crossmatching

27
Antibody Specificity Prediction
The antibody specificity prediction (ASP) method of donor selection for refractory alloimmunized patients appears as effective as HLA matching or crossmatching. Far more donors are identified in a file of HLA-typed donors by the ASP method than by HLA matching, and this indicates that the ASP method provides important advantages regarding the availability of compatible platelet components.
 method of donor selection for refractory alloimmunized patients appears as effective as HLA matching or crossmatching. Far more donors are identified in a file of HLA-typed donors by the ASP method than by HLA matching, and this indicates that the ASP method provides important advantages regarding the availability of compatible platelet components.")
28
Percentage of platelet recovery is similar for HLA-matched, cross-matched, and antibody specificity prediction method matched donor platelets Petz LD. Selecting donors of platelets for refractory patients on the basis of HLA antibody specificity. Transfusion

29
PRA=panel reactive antibodies

30
Cross-Reactive Groups
Systems have been developed to match donor and recipient by assigning HLA-A and HLA-B antigens with shared public epitopes to clusters called cross-reactive groups (CREGs). When one or two mismatches of HLA-A or HLA-B antigens in CREGs is permitted, a pool of 1000–3000 donors will meet the transfusion needs of most white patients
. When one or two mismatches of HLA-A or HLA-B antigens in CREGs is permitted, a pool of 1000–3000 donors will meet the transfusion needs of most white patients.")
31
HLA Matchmaker Based on the principle that short three-amino acid sequences characterize polymorphic sites of the HLA molecules, and are the critical components of allo-sensitizing epitopes Retrospective study has shown that platelets selected with this algorithm result in higher post-transfusion count rises than those selected using traditional HLA matching strategies A Nambiar, RJ Duquesnoy and S Adams et al., HLAMatchmaker-driven analysis of responses to HLA-typed platelet transfusions in alloimmunized thrombocytopenic patients, Blood 107 (2006), pp. 1680–1687.
, pp. 1680–1687.")
32
Clinimmune Testing available for:
Clinical Transplantation- solid organ and hematopoietic stem cell Platelet Transfusion support

33
Clinimmune HLA-A, B, Cw, DRB, DQB1, DPB1 loci HLA Antibody Detection
Low to high resolution testing for HLA-A, B, Cw, DRB1,DRB3/4/5, DQB1 Intermediate to high resolution testing for HLA-DPB1 Serological and molecular testing HLA Antibody Detection PRA=Panel Reactive Antibody, including HLA Specificity Analysis Luminex ELISA Complement Dependent Cytotoxicity, including AHG (anti-human globulin) Titration/Quantitation studies for pre-transplant immunotherapy protocols Crossmatching for transplant compatibility Flow cytometry From Clinimmune website
 Titration/Quantitation studies for pre-transplant immunotherapy protocols. Crossmatching for transplant compatibility. Flow cytometry. From Clinimmune website.")
34
Other options to treat refractoriness?
For highly alloimmunized patients and those with rare HLA types, finding compatible platelets can be difficult. Several immune-modulatory therapies tried: intravenous immune globulin; cyclosporin A; vinblastine; staphyloccal protein A; removal of HLA antigens with citric acid. Despite anecdotal positive outcomes, these strategies are usually not successful or practical

35
Transfusion-associated graft-vs-host disease
Depends on immune system function in recipient lymphocytes in transfused component degree of HLA similarity between donor and recipient Donor lymphocytes not recognized as foreign if HLA similar More common with related donors Especially if donors homozygous for shared HLA haplotype with recipient

36
Transfusion-associated graft-vs-host disease
Caused by persistent chimerism after blood transfusion Transfused lymphocytes avoid destruction by host immune system, proliferate, and attack host organs Causes skin rash (histo “satellite dyskeratosis”), fever, liver dysfunction, diarrhea, bone marrow dysplasia Occurs 4-30 days post-transfusion, >90% fatal In 1980, incidence in patients with hematologic cancers or lymphoproliferative disorders 0.1-1%, now lower due to leukoreduction and irradiation; more rare if not immunocompromised
, fever, liver dysfunction, diarrhea, bone marrow dysplasia. Occurs 4-30 days post-transfusion, >90% fatal. In 1980, incidence in patients with hematologic cancers or lymphoproliferative disorders 0.1-1%, now lower due to leukoreduction and irradiation; more rare if not immunocompromised.")
37
TA-GVHD more common in immunocompromised patients receiving directed donor HLA-matched products, but can occur in immunocompetent individuals and can be random donor with high HLA similiarity For example……

38
Common “ancestral” haplotype
DR3, B8, A1 haplotype In 9% of chromosomes in the Caucasian population, and 18% of chromosomes in Caucasians with diabetes (Alper 2006) Diabetic population at risk for kidney transplantation
 Diabetic population at risk for kidney transplantation.")
39
24 DR3B8A1 (8.1) Homozygous Individuals
Illumina 2: 24 DR3B8A1 (8.1) Homozygous Individuals Column=individual; Row=SNP; Yellow=Homozygous region for 8.1 alleles Gray=non-8.1 allele; White=8.1 allele; Dark Gray Bar=1st SNP homozygous for non-8.1 alleles telomere 25.2 Mb 7.6 Mb conserved HLA-F HLA-A DQB1 32.8 Mb My thesis work
 Homozygous Individuals. Column=individual; Row=SNP; Yellow=Homozygous region for 8.1 alleles. Gray=non-8.1 allele; White=8.1 allele; Dark Gray Bar=1st SNP homozygous for non-8.1 alleles. telomere Mb. 7.6 Mb. conserved. HLA-F. HLA-A. DQB Mb. My thesis work.")
40
Case study 31 yo F receives kidney transplant from her father, matched for all but one antigen, DR7 2 wks later, she needs PRBC transfusion Family wants her to receive directed donor transfusion from father Should a directed donor transfusion from her father be permitted? If so, should it be leukoreduced or irradiated? If not, should a random donor blood product be leukoreduced or irradiated? Should the guidelines for kidney transplant patients differ from those of heart, lung or bone marrow transplant patients? What if patient is known to have one HLA antibody formed against transplant?

41
Follow-up Information
Received directed donor routine PRBC given from father (not leukoreduced or irradiated) Humoral transplant rejection diagnosed PRA antibody negative prior to transfusion; DR7 antibody detected post-transfusion
 Humoral transplant rejection diagnosed. PRA antibody negative prior to transfusion; DR7 antibody detected post-transfusion.")
42
HLA and Transplantation Bone marrow
HLA class I and II matching High resolution Aim for at least 9/10 HLA alleles matching

43
HLA and Transplantation Cord Blood
Low resolution HLA class I match; high-resolution class II HLA match Safer than bone marrow transplant because cord blood induces less reaction Aim for at least 4 out of 6 matching for transplantation

44
HLA and Transplantation Solid organ
Lung: Class II HLA match Heart: Class I HLA match on case-by-case basis, no class I Liver: No HLA typing indicated Kidney: Class I and II HLA matching but O.K if only 1 or 2 out of 6 matching HLA alleles because prognosis depends more on timing of transplant; prefer negative cross-matching strategy

Similar presentations

 Anti-A11 and B44.>")






 from one part or individual to another (Merriam-Webster) May take place between different.>")

 Overview Willis H Navarro, MD Medical Director, Transplant Services, NMDP Associate Clinical Professor,>")

 Anindyaningrum Chrisant Rystiasih Nadia Karlina *Protein images comparing the MHC I (1hsa) and MHC II (1dlh) molecules.>")






