Download presentation
Presentation is loading. Please wait.

1
Update on Pulmonary Hypertension and Implications for Solid Organ Transplantation
Ivan M. Robbins, M.D. Adult Pulmonary Hypertension Center Vanderbilt University

2
Pulmonary circulation
Low resistance, high compliance vascular bed Only organ to receive entire cardiac output (CO) Changes in CO as well as pleural/alveolar pressure affect pulmonary blood flow Different reactions compared to the systemic circulation Normally in a state of mild vasodilation
 Changes in CO as well as pleural/alveolar pressure affect pulmonary blood flow. Different reactions compared to the systemic circulation. Normally in a state of mild vasodilation.")
3
Vascular Pressure in Systemic and Pulmonary Circulations (mm Hg)
120/80, mean 93 25/8, mean 14 Systemic Circulation Pulmonary Circulation Arteries Arteries Right Atrium Mean >6 Left Atrium Mean 5 Body Lung SVR= PVR= 1.8 Right Ventricle 25/2-5 Left Ventricle 120/5-10 Veins Veins

4
Outline Review classification of pulmonary hypertension (PH)
Pulmonary arterial hypertension (PAH) Evaluation of PH and how to differentiate PAH from other forms of PH PH and cardiac, renal and hepatic transplantation Review PAH-approved therapy and treatment of non-Group 1 PH
 Evaluation of PH and how to differentiate PAH from other forms of PH. PH and cardiac, renal and hepatic transplantation. Review PAH-approved therapy and treatment of non-Group 1 PH.")
5
Dana Point Classification of Pulmonary Hypertension (PH)
1) Pulmonary arterial hypertension 2) Pulmonary hypertension due to left heart disease 3) Pulmonary hypertension due to lung diseases and/or hypoxia 4) Chronic Thromboembolic pulmonary hypertension (CTEPH) 5) Pulmonary Hypertension with unclear and/or multifactorial mechanism
 Pulmonary arterial hypertension. 2) Pulmonary hypertension due to left heart disease. 3) Pulmonary hypertension due to lung diseases and/or hypoxia. 4) Chronic Thromboembolic pulmonary hypertension (CTEPH) 5) Pulmonary Hypertension with unclear and/or multifactorial mechanism.")
6
Dana Point Classification of PAH, Group 1
Idiopathic PAH (formerly primary pulmonary hypertension, PPH) Heritable Drug/toxin induced Associated with: Connective tissue diseases HIV infection Portal hypertension Systemic to pulmonary shunts Schistosomiasis Chronic hemolytic anemia
 Heritable. Drug/toxin induced. Associated with: Connective tissue diseases. HIV infection. Portal hypertension. Systemic to pulmonary shunts. Schistosomiasis. Chronic hemolytic anemia.")
7
WHO Group 2 PH Pulmonary hypertension owing to left heart disease
Systolic dysfunction Diastolic dysfunction Valvular disease Pulmonary venous obstruction

8
PH with unclear or multifactorial mechanisms: Group 5
1.Hematologic disorders 2.Systemic disorders: vasculitis 3.Metabolic disorders 4.Others: chronic renal failure on dialysis

9
Definitions Definition of PH: Definition of PAH:
mPAP > 25 mm Hg at rest Definition of PAH: PWP < 15 Normal LVEF No left-sided valvular disease

10
PAH: A Disease of Decline & Deterioration
20 40 60 80 100 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 Years of Follow-up Percentage Surviving IPAH NIH Registry Adapted from: D’Alonzo GE, Ann Int Med, 1991

11
Years From Diagnosis of PHT
Outcome of Scleroderma Patients with Pulmonary Hypertension is worse than IPAH 10 20 30 40 50 60 70 80 90 100 1 2 3 4 5 6 7 8 9 11 12 13 Years From Diagnosis of PHT PHT Lung Involvement (without PHT) None Survival, % Koh et al, Br J Rheumatol, 1996
 None. Survival, % Koh et al, Br J Rheumatol,")
12
IPAH NIH Registry 187 patients followed over 7 years
Extensive evaluation to R/O secondary causes mPAP-60mmHg, CI-2.3 l/min, PVRI-26 U Mean age at Dx: 36, almost 2:1 female:male Mean duration of symptoms before Dx: 2 years Rich, Ann Intern Med, 1987 ~Two cases per 1,000,000

13
PAH is a rare disease Incidence of IPAH: ~1-2 cases/million per year
Prevalence: 5,000 patients? Prevalence of PAH: 30,000 patients? ~50 million Americans have systemic hypertension 61% of American adults are overweight 27% are obese (BMI>30) 16% of Americans have diabetes 22% have hyperlipidemia
 16% of Americans have diabetes. 22% have hyperlipidemia.")
14
PAH is rare in patients >65 yo referred to our PH center
Diagnosis Number (%) (n = 248) Pulmonary Arterial Hypertension (PAH) 37 (15%) Idiopathic PAH 5 CTD-associated PAH 28 CHD-associated PAH 1 Portopulmonary HTN 3 PH owing to left heart disease 70 (28%) PH owing to lung disease and/or hypoxia 35 (14%) Chronic thromboembolic PH 19 (8%) Other or mixed causes of PH 42 (17%) Unknown 24 (10%) No PH 21 (8%) Patients aged 65 years or older referred to VUMC Pulmonary Vascular Disease Center for known or suspected PH between XXX (time that PH panel was made) and 9/2011. Patients with previously established PAH who presented for transfer of care were excluded. Patients were classified by pulmonary vascular disease specialist according to standard guidelines. Pugh et al, submitted, 2012
 (n = 248) Pulmonary Arterial Hypertension (PAH) 37 (15%) Idiopathic PAH. 5. CTD-associated PAH. 28. CHD-associated PAH. 1. Portopulmonary HTN. 3. PH owing to left heart disease. 70 (28%) PH owing to lung disease and/or hypoxia. 35 (14%) Chronic thromboembolic PH. 19 (8%) Other or mixed causes of PH. 42 (17%) Unknown. 24 (10%) No PH. 21 (8%) Patients aged 65 years or older referred to VUMC Pulmonary Vascular Disease Center for known or suspected PH between XXX (time that PH panel was made) and 9/2011. Patients with previously established PAH who presented for transfer of care were excluded. Patients were classified by pulmonary vascular disease specialist according to standard guidelines. Pugh et al, submitted,")
15
Pathogenesis of PAH 2012: An Integrated View
Other Risk Factors Altered Pathways and Mediators Genetic Predisposition Proliferation Vasoconstriction Thrombosis Vascular Remodeling Inflammation

16
PH - History History of smoking ETOH/recreational drug use
Systemic hypertension Cyanosis/murmur as a child Joint/musculoskeletal pain Raynaud’s Syndrome FH of unexplained early cardiopulmonary disease Previous DVT, PE or family hx of thromboembolic dz Use of appetite suppressant drugs

17
PH- Symptoms DOE Fatigue, weakness Chest pain LE or abdominal swelling
Syncope Not typical of PAH: orthopnea

18
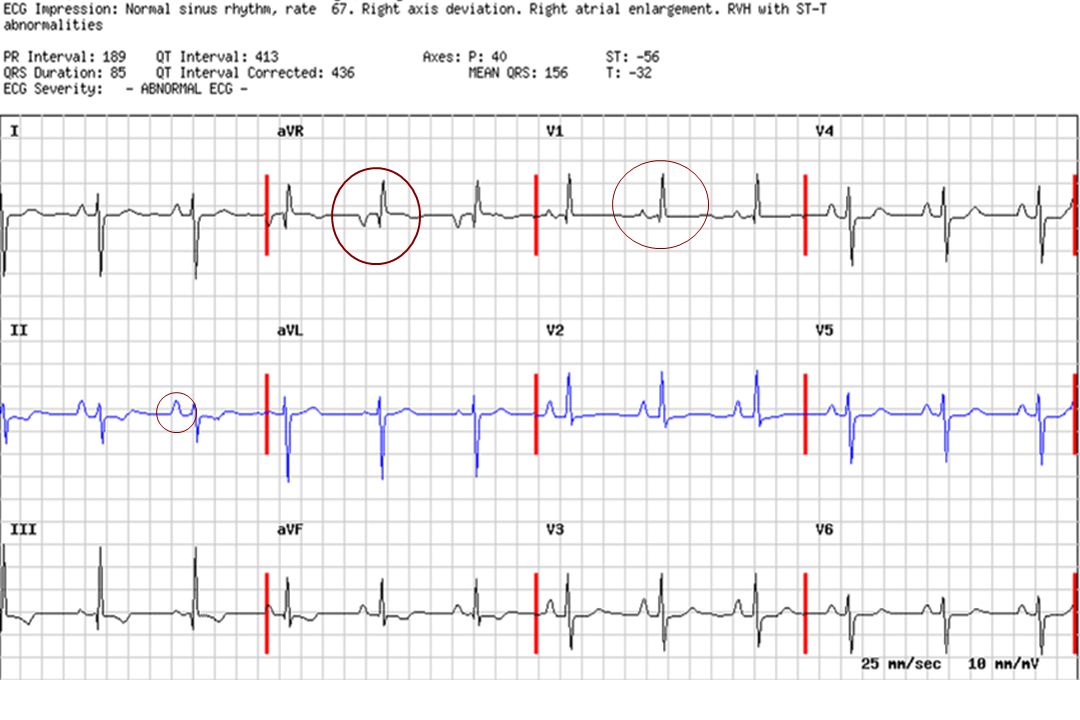
Evaluation for PH ECG Chest x-ray
V/Q scan or contrasted spiral CT (+/- angiogram) PFTs Exercise oximetry Echocardiogram Right heart catheterization w/vasodilator testing Labs: CBC, CMP, INR, ANA, HIV, TFTs
 PFTs. Exercise oximetry. Echocardiogram. Right heart catheterization w/vasodilator testing. Labs: CBC, CMP, INR, ANA, HIV, TFTs.")
19
Clues to causes of PH other than PAH
Dilated LA on echo or on CT angiogram Hx of systemic vascular disease LVH, LAE, no evidence of RVH or RAD on ECG Orthopnea Crackles, clubbing Development of pulmonary edema with pulmonary vasodilators Think of disorders affecting pulmonary veins

21
PH - Radiographic studies
CXR: -large proximal PA with peripheral tapering (pruning) -cardiomegaly due to enlarged RA, RV -pleural effusion is uncommon CT: -PA >aorta -cardiomegaly, enlarged RV -pericardial effusion
 -cardiomegaly due to enlarged RA, RV. -pleural effusion is uncommon. CT: -PA >aorta. -cardiomegaly, enlarged RV. -pericardial effusion.")
22
CXR in PAH

23
CXR in Eisenmenger Syndrome

24
Mitral Stenosis

25
Enlarged main PA on CT Standard view Coronal view

28
Ventilation Perfusion Lung Scan
CTEPH PAH

29
Evaluation for Chronic Thromboembolic PH (CTEPH)
V/Q scan remains the best screening tool CT angiogram is excellent for acute, proximal PE but can miss CTEPH Gold standard for diagnosis is pulmonary angiogram Safe procedure even in patients with marked PH Mortality in 2 large studies: 0/547 and 2/202* PE No PE Tanariu, N. et al, J Nucl Med, 2007 *Hofman LV, et al, AJR, 2004 Pitton MB, et al, AJR, 2007

30
CTEPH: Pulmonary Angiography
Confirms diagnosis of CTEPH in patients with PH Assess thrombus accessibility Distinct angiographic patterns “Web” narrowing Poststenotic dilatation Proximal occlusion “Pouch” defects

31
Organized Clot Removed at Surgery

32
Pulmonary Function tests
No characteristic changes Mandatory to screen for significant restrictive or obstructive lung disease Diffusing capacity often significantly reduced in patients with scleroderma (<50%)
")
33
RV, RA Enlargement on Echocardiogram
LV RA LA Normal PH

34
PH by Echo ≠ PAH Single echo lab / Australian community of 160,000
~10% of patients had est. sPAP>40 mm Hg Only 2.3% with PAH after full evaluation Left heart disease, 78.7% PAH, 2.3% Congenital heart disease, 1.9% Lung disease/ Sleep-related hypoventilation, 9.7% CTEPH, 0.6% Unknown, 6.8% It is important to recognize that while echo is an excellent screening tool when there is suspicion of PH, the echo and cath are complementary, and one cannot substitute for the other. This slide depicts data from a single echo lab on the ultimate diagnosis reached in 483 patients found to have PH on echo. Not unexpectedly, the majority had left heart disease and, importantly, only a small number (2%) had PAH. While these data are subject to referral bias and we cannot be certain of the diagnostic criteria used, the point remains: The echo and cath are each essential. We cannot be certain of PAH on the basis of the echo alone. N=483 of 4579 patients with echo PASP >40 mm Hg. Gabby E. Am J Respir Crit Care Med. 2007;175:A713.
 had PAH. While these data are subject to referral bias and we cannot be certain of the diagnostic criteria used, the point remains: The echo and cath are each essential. We cannot be certain of PAH on the basis of the echo alone. N=483 of 4579 patients with echo PASP >40 mm Hg. Gabby E. Am J Respir Crit Care Med. 2007;175:A713.")
35
Echo estimate of PAP often inaccurate in advanced lung disease
Overestimation Accurate Underestimation Cohort: 374 lung txp pts Echo 24–48 h prior to RHC Prevalence of PH: 25% Echo frequently leads to over-diagnosis of PH in patients with advanced lung disease 20 40 60 % of studies Although the echo is often remarkably accurate in its estimate of pulmonary pressures, in certain situations (as depicted here in patients with advanced lung disease undergoing evaluation for transplant) it can be less reliable. The point is NOT that echo is less valuable. Echo provides important structural, valvular, functional data that are complementary to the cath. Rather, the point is that both tests are essential to be certain of the right diagnosis. PH (-) PH (+) Arcasoy SM et al. Am J Respir Crit Care Med. 2003;167:
 it can be less reliable. The point is NOT that echo is less valuable. Echo provides important structural, valvular, functional data that are complementary to the cath. Rather, the point is that both tests are essential to be certain of the right diagnosis. PH (-) PH (+) Arcasoy SM et al. Am J Respir Crit Care Med. 2003;167:")
36
Right Heart Catheterization
Gold standard for diagnosis of PH Crucial for determining cause of PH, i.e. pre- vs post-capillary process Required prior to initiating therapy for PAH Acute vasodilator testing should be performed at time of RHC in patients with PAH

37
PH: The Importance of Hemodynamics
Pulmonary venous hypertension Mixed etiology PCWP >15 mm Hg VC RA RV PA PV LA LV Ao PC Right heart catheterization (RHC) is the diagnostic gold standard for PH. RHC is required to confirm the diagnosis of PH and assess its severity (for prognosis), exclude left heart disease, and perform vasoreactivity testing. This slide represents the cardiovascular connections in series: [VC=vena cava, RA=right atrium, RV=right ventricle, PA=pulmonary artery, PC=pulmonary capillary bed, PV=pulmonary venous bed, LA=left atrium, LV=left ventricle, Ao=aorta]. Patients with PH in WHO group I (PAH), III, or IV have “pre-capillary” PH, where the left-sided filling pressure (PWCP and/or LVEDP) is normal and the pulmonary vascular resistance (PVR) is elevated. In the case of pulmonary venous hypertension (“passive” or “post-capillary” PH), which is related to diseases of the left heart, PA mean pressure and PCWP are elevated, whereas PVR is normal. For some patients the picture is mixed: left-sided filling pressure and PVR are both elevated. Clinically, this situation is seen most commonly with advanced systolic LV failure or restrictive cardiomyopathy (typically associated with “reactive” pulmonary vasoconstriction). Patients with a high CO state (“hyperkinetic” PH) have elevated mean PAP and CO, yet normal LV filling pressure and PVR. PAH PH with respiratory disease CTEPH Other: High CO PCWP ≤15 mm Hg PVR ≤3 Wood units PCWP ≤15 mm Hg PVR >3 Wood units 37
 is the diagnostic gold standard for PH. RHC is required to confirm the diagnosis of PH and assess its severity (for prognosis), exclude left heart disease, and perform vasoreactivity testing. This slide represents the cardiovascular connections in series: [VC=vena cava, RA=right atrium, RV=right ventricle, PA=pulmonary artery, PC=pulmonary capillary bed, PV=pulmonary venous bed, LA=left atrium, LV=left ventricle, Ao=aorta]. Patients with PH in WHO group I (PAH), III, or IV have pre-capillary PH, where the left-sided filling pressure (PWCP and/or LVEDP) is normal and the pulmonary vascular resistance (PVR) is elevated. In the case of pulmonary venous hypertension ( passive or post-capillary PH), which is related to diseases of the left heart, PA mean pressure and PCWP are elevated, whereas PVR is normal. For some patients the picture is mixed: left-sided filling pressure and PVR are both elevated. Clinically, this situation is seen most commonly with advanced systolic LV failure or restrictive cardiomyopathy (typically associated with reactive pulmonary vasoconstriction). Patients with a high CO state ( hyperkinetic PH) have elevated mean PAP and CO, yet normal LV filling pressure and PVR. PAH. PH with respiratory disease. CTEPH. Other: High CO. PCWP ≤15 mm Hg. PVR ≤3 Wood units. PCWP ≤15 mm Hg. PVR >3 Wood units. 37.")
38
Other Helpful Diagnostic Tests (Determined by patient’s history)
High resolution chest CT Cardiopulmonary exercise study Polysomnography Arterial blood Gas Hepatitis serologies Left heart catheterization, evaluation of coronary arteries

39
PH and Cardiac Transplantation
ISHLT guidelines: no absolute cutoffs for PH that prohibits transplant1 Relative contraindication: PVR>5 or PVRI>6 or TPG >16-20 Increased risk of RHF and death if sPAP >60 mm Hg and one of the above If PVR to <2.5 with vasodilator but patient becomes hypotensive, persistent high risk (3.8% vs 27.5% 3 month mortality2 1. Mehra, M. et al, J Heart Lung Transplant, 2006 2. Costard-Jackle, et al, JACC, 1992

40
Causes of RV failure after cardiac transplantation in patients with PH
Smaller mass than LV, less able to adapt to increased afterload Low coronary blood flow/unit mass, less cooling, perhaps less cardioplegia TR results from annular distortion during implantation and from increased afterload

41
PH in ESRD Prevalence up 48% on echo reported in literature1-4
Only 10-14% had est. sPAP>45-50 mm Hg1 Largest study: 500 pts, 68 (13%) on PD Mean sPAP: 47±9 mm Hg, range: mm Hg 5.9% incidence in PD patients Longer duration of dialysis in PH pts, 51 vs 30 months Patients with PH had: Higher CO1-3 Worse survival1,3 1. Yigla et al, Chest, 2003 2. Nakhoul, et al Nehrol Dial Transplant, 2005 3. Issa et al, Transplantation, 2008 4. Bozbas et al, Transplanat Proc, 2009 5. Hemnes et al, Nephrol Seminar, 2010
 on PD. Mean sPAP: 47±9 mm Hg, range: mm Hg. 5.9% incidence in PD patients. Longer duration of dialysis in PH pts, 51 vs 30 months. Patients with PH had: Higher CO1-3. Worse survival1,3. 1. Yigla et al, Chest, Nakhoul, et al Nehrol Dial Transplant, Issa et al, Transplantation, Bozbas et al, Transplanat Proc, Hemnes et al, Nephrol Seminar,")
42
PH is a risk factor for decreased survival in hemodialysis patients
Yigla, et al Kidney International, 2009

43
Problems with studies of PH in ESRD
No direct hemodynamic measurements All studies are estimated pressure by echo PH generally defined as est. sPAP>35 mm Hg Volume status of patients not reported RV function is reported in only one study No measurement of PWP or PVR Many studies involve small numbers of patients No prospective studies

44
Echocardiographic findings in ESRD patients undergoing transplant
Echocardiographic Data Patients With PHT (n = 85) Patients Without PHT (n = 415) P Value LV, diastole (cm) 4.9 ± 0.5 4.7 ± 2.0 .3 LV, systole (cm) 3.2 ± 0.5 3.1 ± 0.5 .8 Right ventricle (cm) 3.3 ± 0.5 3.2 ± 0.4 Left atrium (cm) 4.0 ± 0.7 3.5 ± 0.6 <.0001 Right atrium (cm) 3.7 ± 0.5 3.3 ± 0.4 Diastolic dysfunction (%) 18.8 21.4 .6 Systolic dysfunction (%) 22.4 13.5 .04 LV ejection fraction (%) 49.7 ± 7.9 52.3 ± 6.9 .002 LV hypertrophy (%) 78.8 59.8 .001 Bozbas et al, Transplantation Proceedings, 2009
 Patients Without PHT. (n = 415) P Value. LV, diastole (cm) 4.9 ± ± LV, systole (cm) 3.2 ± ± Right ventricle (cm) 3.3 ± ± 0.4. Left atrium (cm) 4.0 ± ± 0.6. < Right atrium (cm) 3.7 ± ± 0.4. Diastolic dysfunction (%) Systolic dysfunction (%) LV ejection fraction (%) 49.7 ± ± LV hypertrophy (%) Bozbas et al, Transplantation Proceedings,")
45
PH is a associated with decreased survival after renal transplant
Retrospective analysis of 215/472 renal txp pts who had echo and est. RVSP obtainable1 48% on no HD prior to txp, only 10 on PD Mean RVSP 34±10 mm Hg, range 21-71 RVSP <35 mm Hg in 68%, mm Hg in 22%, >50 mm Hg in 10% (22 pts) Time on HD significantly related to development of PH independent of other risk factors 1.Issa et al, Transplantation, 2008
 Time on HD significantly related to development of PH independent of other risk factors. 1.Issa et al, Transplantation,")
46
Summary Pulmonary hypertension being recognized more frequently in patients with ESRD LV dysfunction and fluid overload are the primary factors contributing to clinically significant PH in patients on HD Although PH is associated with worse outcome, patients are not dying of rh failure PH, as with other disorders, is associated with worse outcome

47
PH in patients with portal hypertension
All patients must be screened for PH Portopulmonary HTN: mPAP> 25 mm Hg PVR> 3 units PWP <15 mm Hg Krowka, MJ Semin Respir Crit Care Med, 2012

48
Portopulmonary hypertension
~5% of pts in a large epidmiological study of PAH Occurs in % of liver transplant candidates Outcome is poor untreated: 14% and 4% in 2 uncontrolled studies Death can occur due to RH failure or liver dz Treated, survival is improved: 40-68% 5 yr survival Can obtain MELD exception if hemodynamic improvement with PAH therapy

49
Implications for liver transplantation
Higher risk with mPAP>35 mm Hg Up to 36% post-tx in-hospital mortality due to: Acute RH failure during reperfusion of liver Frequent need for enormous amount of blood products Mild PH with normal PVR generally resolves after transplant Effect of Tx in pts with mPAP>35 mm Hg with increased PVR is unpredictable

50
Treatment of Pulmonary Hypertension

51
Treatment of non PAH-pulmonary hypertension
Pulmonary Venous Hypertension: Treat heart failure with afterload reduction Systolic or diastolic MV or AV disease Replace the valve Pulmonary vein stenosis Pulmonary vein stenting

52
Treatment of non PAH-pulmonary hypertension
PH associated with disorders of the respiratory system and/or hypoxemia: Rx of hypoxemia is often the main therapy PH due to chronic thromboembolic disease: Thromboendarterectomy for proximal disease Can consider PAH therapy for distal disease

53
Adjunctive treatments of PAH
Anticoagulation Diuretics Digoxin Oxygen Calcium channel blockers Exercise Salt restriction

54
Targets for current PAH-specific therapy
Arachidonic Acid Prostacyclin Synthase Vasodilatation and Antiproliferation Prostacyclin cAMP Prostacyclin Derivatives Prostacyclin Pathway Big Endothelin Endothelin- converting Enzyme Endothelin Receptor A Endothelin Receptor B Vasoconstriction and Proliferation Endothelin Receptor Antagonists Endothelin-1 Endothelin Pathway Arginine Nitric Oxide Synthase Vasodilatation and Antiproliferation Nitric Oxide cGMP Exogenous Nitric Oxide Phosphodiesterase Type-5 Phosphodiesterase Type-5 Inhibitors Nitric Oxide Pathway Humbert M et al. N Engl J Med. 2004

55
Specific PAH Treatment
Epoprostenol (generic and Flolan®) Treprostinil (Remodulin®) Iloprost (Ventavis®) Bosentan (Tracleer®) Ambrisentan (Letairis®) Tadalifil (Adcirca®) Sildenafil (Revatio®) Prostaglandins Endothelin receptor antagonists (ERAs) Phosphodiesterase 5 inhibitors (PDE5 inhibitors)
 Treprostinil (Remodulin®) Iloprost (Ventavis®) Bosentan (Tracleer®) Ambrisentan (Letairis®) Tadalifil (Adcirca®) Sildenafil (Revatio®) Prostaglandins. Endothelin receptor. antagonists (ERAs) Phosphodiesterase 5. inhibitors (PDE5 inhibitors)")
56
Comparison of Medical Treatments for PAH
Cost $ (annual) Route Frequency Ease of Use Side effects Long-term Randomized data Epoprostenol ~100,000 IV Continuous + +++ No Treprostinil >175,000 SQ, IV, Inhaled ++ Iloprost ~175,000 Inhaled 6-9x per day Sildenafil ~15,000 Oral TID Tadalafil ~12,000 Daily Bosentan ~75,000 BID ++++ Ambrisentan Once a day
 Route. Frequency. Ease. of Use. Side. effects. Long-term. Randomized data. Epoprostenol. ~100,000. IV. Continuous No. Treprostinil. >175,000. SQ, IV, Inhaled. ++ Iloprost. ~175,000. Inhaled. 6-9x per day. Sildenafil. ~15,000. Oral. TID. Tadalafil. ~12,000. Daily. Bosentan. ~75,000. BID Ambrisentan. Once a day.")
57
PAH Determinants of Risk
Lower Risk Determinants of Risk Higher Risk No Clinical evidence of RV failure Yes Gradual Progression Rapid II, III WHO class IV Longer (>400 m) 6MWD Shorter (<300 m) Minimally elevated BNP Very elevated Minimal RV dysfunction Echocardiographic findings Pericardial effusion, significant RV dysfunction Normal/near normal RAP and CI Hemodynamics High RAP, low CI McLaughlin VV, McGoon MD. Circulation. 2006;114:
 6MWD. Shorter (<300 m) Minimally elevated. BNP. Very elevated. Minimal RV dysfunction. Echocardiographic findings. Pericardial effusion, significant RV dysfunction. Normal/near normal RAP and CI. Hemodynamics. High RAP, low CI. McLaughlin VV, McGoon MD. Circulation. 2006;114:")
58
LUNG TRANSPLANTATION The only cure for PAH
IPAH in UNOS database Survival was calculated using the Kaplan-Meier method, which incorporates information from all transplants for whom any follow-up has been provided. Since many patients are still alive and some patients have been lost to follow-up, the survival rates are estimates rather than exact rates because the time of death is not know for all patients. Survival rates were compared using the log-rank test statistic. P = 0.3

59
Take Home Points PH can not be diagnosed by Echo alone, need a thorough evaluation for all patients Right heart catheterization is necessary in ALL patients to accurately diagnose PH PAH is a progressive disease, even with Rx Make sure the patient has PAH before treating Despite multiple therapies, lung transplantation is the only curative treatment for PAH PH negatively impacts outcome of all solid organ transplants

Similar presentations







 Department of Clinical Pharmacy Salman Bin AbdulAziz University College Of Pharmacy.>")









 CPP = aortic diastolic.>")



