Download presentation
Presentation is loading. Please wait.

1
Sebastiano Mercadante, MD
Professor of Palliative Medicine, University of Palermo Director Anesthesia & ICU - Pain Relief & Palliative Care Unit La Maddalena Cancer Center, Palermo – Italy 1

3
LE COMPONENTI DEL DOLORE ONCOLOGICO
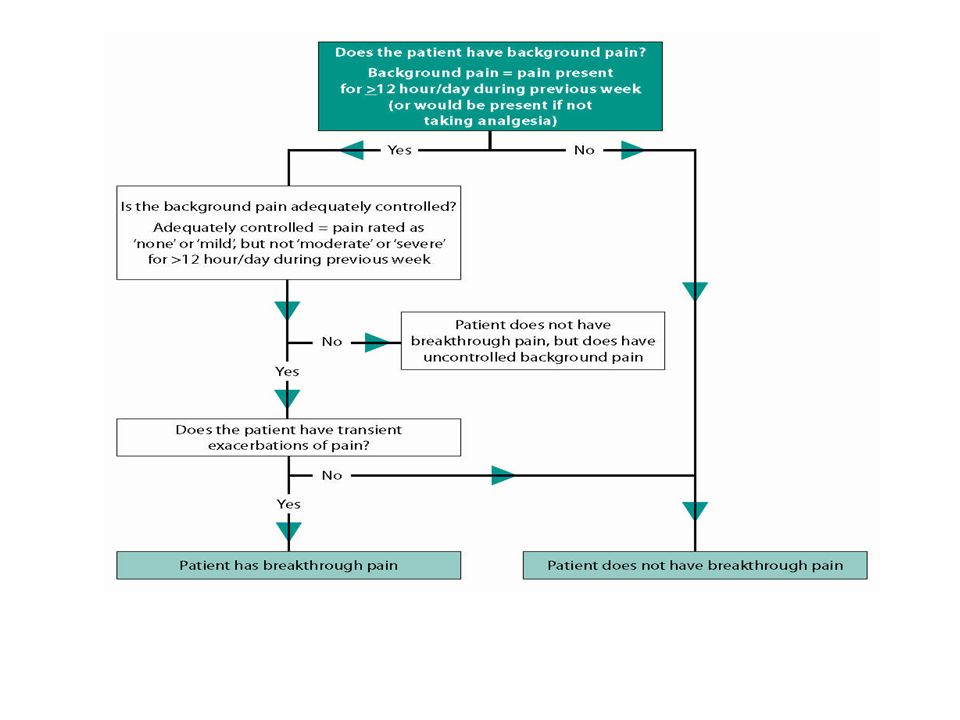
Dolore di base o persistente BreakThrough cancer Pain (BTcP) What is BTcP? It occurs in patients with cancer who have persistent pain. i.e. pain that is experienced for at least 12 hours per day and is managed with ATC medication. BTcP is a transitory exacerbation of pain experienced by the patient who has relatively stable and adequately controlled baseline pain. BTcP requires independent assessment and targeted treatment. The graphic illustrates how BTcP “breaks through” the level of analgesia provided by around-the-clock (ATC) medication used to control a patient’s persistent pain. References Portenoy et al. Oxford Textbook of Palliative Medicine (3rd ed) Oxford University Press, Oxford, 438–458. Bennett D, Burton AW, Fishman S, et al. Consensus panel recommendations for the assessment and management of breakthrough pain. Part II—management. Pharm Ther 2005;30:354–361. O 1-Portenoy RK, et al. Oxford Textbook of Palliative Medicine (3rd ed). Oxford: Oxford University Press; 2004:438-58 2-Bennett D, et al. Pharmacy & Therapeutics. 2005;30: 3-Zeppetella G. et al. Curr Op Supp Pall Care Realizzato con il contributo non condizionato di Cephalon
 What is BTcP It occurs in patients with cancer who have persistent pain. i.e. pain that is experienced for at least 12 hours per day and is managed with ATC medication. BTcP is a transitory exacerbation of pain experienced by the patient who has relatively stable and adequately controlled baseline pain. BTcP requires independent assessment and targeted treatment. The graphic illustrates how BTcP breaks through the level of analgesia provided by around-the-clock (ATC) medication used to control a patient’s persistent pain. References. Portenoy et al. Oxford Textbook of Palliative Medicine (3rd ed) Oxford University Press, Oxford, 438–458. Bennett D, Burton AW, Fishman S, et al. Consensus panel recommendations for the assessment and management of breakthrough pain. Part II—management. Pharm Ther 2005;30:354–361. O. 1-Portenoy RK, et al. Oxford Textbook of Palliative Medicine (3rd ed). Oxford: Oxford University Press; 2004: Bennett D, et al. Pharmacy & Therapeutics. 2005;30: Zeppetella G. et al. Curr Op Supp Pall Care. Realizzato con il contributo non condizionato di Cephalon.")
4
Characteristics of BP Frequency 30-90% Moderate to severe intensity
Rapid onset (<3 minutes in 43% of patients) Often unpredictable Relatively short duration (30-60’) Frequency: 1-4 episodes per day Features: Physical consequences Psychological consequences Social consequences Resource consequences
 Often unpredictable. Relatively short duration (30-60’) Frequency: 1-4 episodes per day. Features: Physical consequences. Psychological consequences. Social consequences. Resource consequences.")
6
Episodic (Breakthrough) Pain Consensus Conference of an Expert Working Group of the EAPC, Cancer 2002 Sebastiano Mercadante, M.D.1 Lukas Radbruch, M.D.2 Augusto Caraceni, M.D.3 Nathan Cherny, M.D.4 Stein Kaasa, M.D., Ph.D.5 Friedemann Nauck, M.D.6 Carla Ripamonti, M.D.3 Franco De Conno, M.D.3 the Steering Committee of the European Association for Palliative Care (EAPC) Research Network BACKGROUND: Breakthrough pain is transitory exacerbation of pain that occurs in addition to otherwise stable persistent pain. The wide differences in estimation of incidence reported in literature are probably because of different settings and meanings attributed to the definition to breakthrough pain. METHODS: A panel of experts met to establish the actual knowledge on breakthrough pain, according to the evidence in literature and experience. They agreed that episodic or transient pain could be a more simple and adequate term in most languages, including English, France, Italian, and Spanish. RESULTS: A specific assessment and precise pain characterization are essential to plan the most appropriate treatments. Despite the relevance of this temporal pain pattern for the influence on the outcome and quality of life, few controlled studies have been performed to give evidence of a specific approach. Several experiences have reported the possible efficacy of different drugs, route of administration, and modalities of administration in different circumstances. CONCLUSIONS: Prospective studies with previous treatments using similar terminologies are necessary to find the most convenient therapeutic intervention, according to the temporal pattern characteristics and the pain mechanism involved. Cancer 2002;94: © 2002 American Cancer Society. DOI /cncr.10249 KEYWORDS: cancer pain, breakthough pain, incident pain, transient pain, opioids, nonsteroidal antiinflammatory drugs (NSAIDs), pamidronate, transmucosal fentanyl, radiotherapy, spinal opioids.
 Research Network. BACKGROUND: Breakthrough pain is transitory exacerbation of pain that occurs in addition to otherwise stable persistent pain. The wide differences in estimation of incidence reported in literature are probably because of different settings and meanings attributed to the definition to breakthrough pain. METHODS: A panel of experts met to establish the actual knowledge on breakthrough pain, according to the evidence in literature and experience. They agreed that episodic or transient pain could be a more simple and adequate term in most languages, including English, France, Italian, and Spanish. RESULTS: A specific assessment and precise pain characterization are essential to plan the most appropriate treatments. Despite the relevance of this temporal pain pattern for the influence on the outcome and quality of life, few controlled studies have been performed to give evidence of a specific approach. Several experiences have reported the possible efficacy of different drugs, route of administration, and modalities of administration in different circumstances. CONCLUSIONS: Prospective studies with previous treatments using similar terminologies are necessary to find the most convenient therapeutic intervention, according to the temporal pattern characteristics and the pain mechanism involved. Cancer 2002;94: © 2002 American Cancer Society. DOI /cncr KEYWORDS: cancer pain, breakthough pain, incident pain, transient pain, opioids, nonsteroidal antiinflammatory drugs (NSAIDs), pamidronate, transmucosal fentanyl, radiotherapy, spinal opioids.")
7
Breakthrough pain… stories

8
Prima definizione: “BTcP is a transitory increase in pain to greater than moderate intensity which occurs on a baseline pain of moderate intensity or less (Portenoy and Hagen, 1990). ? Pain intensity should be severe (on a numerical scale 7/10), but the baseline pain could be moderate (on a numerical scale 4-6/10) (Serlin et al., 1995). Thus, the differences between the intensity of BTcP could be minimal (1-2 points on a numerical scale).
 Pain intensity should be severe (on a numerical scale 7/10), but the baseline pain could be moderate (on a numerical scale 4-6/10) (Serlin et al., 1995). Thus, the differences between the intensity of BTcP could be minimal (1-2 points on a numerical scale).")
9
Supportive Care Cancer 2010
Breakthrough pain in oncology: a longitudinal study Sebastiano Mercadante MD *°, Enrico Breda, MD +, Carlo Arcara, MD #, Vittorio Gebbia, MD #, Giampiero Porzio, MD #, Federica Aielli, MD #, Fabrizio David, MD*, Teresa Gammucci, MD^, Filomena Narducci, MD^ , Gaetano Lanzetta, Rossella Restuccia, Alessandro Lembo, MD ¶, Virginia Passeri, MD ¶, Vladimir Virzì, MD » Alessandra Casuccio BS $, ♦ Mercadante S et al. Breakthrough pain in oncology: a longitudinal study. J Pain Symptom Manage 2010. ♦ Mercadante S. et al. Breakthrough pain in advanced cancer patients followed at home: a longitudinal study. J Pain Symptom Manage 2009 ♦ Mercadante S. et al. Attitudes on breakthrough pain in hospice. An Italian survey. Supportive Care Cancer 2010

11
Pts admitted in APRPC were divided in the following classes, according to the level of background pain intensity and analgesic drugs used at admission (T0): Patients with no pain-mild pain NO opioids Patients with mild pain receiving weak opioids Patients with moderate pain receiving weak opioids Patients with severe pain receiving weak opioids Patients with mild pain receiving strong opioids Patients with moderate pain receiving strong opioids Patients with severe pain receiving strong opioids Patients with severe pain, receiving NO opioids Patients with moderate pain, receiving NO opioids.

12
MEANINGFUL CUT-OFF PAIN INTENSITY FOR BTcP CHANGES IN ADVANCED CANCER PATIENTS. Submitted
The meaningful pain intensity for asking for a BTcP medication was 7.1/10. 77% of patients had a pain intensity of 7-8 on a numerical scale 0-10. The meaningful pain intensity for adequate analgesia after a BTcP medication was 3.5/10. Similarly, 77% of patients had a pain intensity of 3-4. There was no relationship with the variables examined for coping. Concerns about the use of BTcP medications were minimal.

13
Dolore osseo: prognosi
Per la sua natura intermittente, il dolore è difficile da controllare, e limita il malato ad evitare di muovere con ovvie conseguenze sulla qualità di vita. Il dolore incidente associato a metastasi ossee è considerato un fattore prognostico negativo per il controllo del dolore (Bruera et al,1989, Mercadante et al,1992). La libertà di movimento è particolarmente difficile da raggiungere (Banning et al,1991). 13
. La libertà di movimento è particolarmente difficile da raggiungere (Banning et al,1991). 13.")
14
Construct for opioid titration in incident pain
Analgesic line Toxicity line Dose Dose for pain on movement Dose for pain at rest Incident pain can be an expression of poor basal pain control. It may be possible to prevent or limit the intensity of pain induced by movement by increasing opioid doses to the top of the therapeutic window.1 Recent animal studies of metastatic bone pain suggest that similar pain intensities induced by different stimuli (i.e. cancer cells injected in bone or inflammatory stimulus) may have different sensitivities to opioids.1 Reference: 1. Mercadante S et al. J Pain Symptom Manage 2004; 28: Effects Mercadante S et al. Optimization of opioid therapy……J Pain Symptoms Manage 2004 14
 may have different sensitivities to opioids.1. Reference: 1. Mercadante S et al. J Pain Symptom Manage 2004; 28: Effects. Mercadante S et al. Optimization of opioid therapy……J Pain Symptoms Manage")
15
Balancing Analgesia and Side Effects
The goal of opioid therapy is to achieve maximal analgesia with minimal side effects.This means that side effects should be managed aggressively and that opioids should be dosed in a manner that matches opioid blood levels with the intensity of pain. The goal is to achieve the optimal balance between analgesia and side effects.

16
Ideal Breakthrough Pain Medication
Rapid onset Short duration of effect Minimal side effects Noninvasive, easy-to-use Cost-effective Portenoy RK, Hagen NA. Pain. 1990;41: 16

17
BTP Profile Oral Morphine Profile Overmedication Pain relief gap
Pain Intensity Oral Morphine Profile BTP Profile Overmedication 5 30 60 Time (minutes) 17
 17.")
18
Short-acting opioids are the mainstay of pharmacological treatment1
Due to its nature, breakthrough cancer pain requires a treatment that: Has a fast onset of action2 Is appropriate in its potency3 Is easily administered3 The WHO analgesic ladder recommends background pain is controlled with around-the-clock analgesia4 Issues with opioids:1 Only effective if breakthrough cancer pain is an opioid-responsive pain1 Only effective if onset of action reflects the duration of the episode1 Breakthrough cancer pain is distinct from background pain.1 Patients suffer an average of 2-4 episodes of breakthrough cancer pain per day.2,3 Breakthrough cancer pain is:2 Rapid in onset (<3 minutes in 43% of patients) Transitory (median 30 minutes) Evident in patients with otherwise stable and adequately controlled background pain References: 1. Zeppetella G and Ribeiro MDC. Opioids for the management of breakthrough (episodic) pain in cancer patients. The Cochrane Database of Systematic Reviews 2006. 2. Portenoy RK and Hagen NA. Pain 1990; 41: 3. Hojsted J et al. Acta Anaethesiol Scand 2006; 50: 1. Davies AN. Brit J Hosp Med 2006; 67: Mercadante S et al. J Pain Symptom Manage 2004; 27: Mercadante S et al. Cancer 2002; 94: World Health Organisation. WHO analgesic ladder for cancer. Accessed 09/06/07.
 Transitory (median 30 minutes) Evident in patients with otherwise stable and adequately controlled background pain. References: 1. Zeppetella G and Ribeiro MDC. Opioids for the management of breakthrough (episodic) pain in cancer patients. The Cochrane Database of Systematic Reviews Portenoy RK and Hagen NA. Pain 1990; 41: Hojsted J et al. Acta Anaethesiol Scand 2006; 50: Davies AN. Brit J Hosp Med 2006; 67: Mercadante S et al. J Pain Symptom Manage 2004; 27: Mercadante S et al. Cancer 2002; 94: World Health Organisation. WHO analgesic ladder for cancer. Accessed 09/06/07.")
19
Dolore persistente trattato con terapia oppioide
TRATTAMENTO DEL BTcP Il trattamento ideale dovrebbe coprire tutta la variabilità degli episodi di BTcP 3’ 60’ Durata Durata Durata Durata Intensità A: Inter individual variably is important: A physician or a hospital with a big number of patients who want only to prescribe or to reference one or two BTcP medicines should choose one that covers a maximum of situations. Intra-individual variably is very important. A patient should have a medicine that covers if possible every BTcP. The Ideal treatment should cover all BTcP Episodes. F: What are the advantages of FBT in this case? Dolore persistente trattato con terapia oppioide Tempo 19 19

20
Flexible use of oral morphine
Anticipated before starting activity (approximately 30’ before) Patients happy with… one shot… Slow onset BP 20
 Patients happy with… one shot… Slow onset BP. 20.")
21
Main data of new formulation - Efficacy in acute administration in comparison with placebo or oral drugs Efficacy in long-term studies - Pain relief within 7-15 min. - Dose-proportionality - Uncertainty on dosing (to titrate..?)
.")
22
BTcP Therapies: Delivery Systems MERCADANTE, DRUGS 2012
1998 2006/2008 2009 2008 2009 2009 Oral trans -mucosal fentanyl citrate OTFC FENTORA®(US)/ EFFENTORA™(EU) ONSOLIS™ (US) FBSF Rapinyl™/ Abstral (EU) SLF Instanyl™ (EU) INFS NasalFent ® (EU) FPNS Several delivery systems are available today and many more are under development They use different route of administration none of them is oral because of the first pass effect and implement They can be grouped into two broad categories based on the route of administration: Buccal/sublingual and nasal Oral Transmucosal Lozenge Effervescent Buccal Tablet Fentanyl Buccal Soluble Film Sublingual Fentanyl Intranasal Fentanyl Sprayy Fentayl Pectin Nasal Spray 22 22 22
/ EFFENTORA™(EU) ONSOLIS™ (US) FBSF. Rapinyl™/ Abstral. (EU) SLF. Instanyl™ (EU) INFS. NasalFent ® (EU) FPNS. Several delivery systems are available today and many more are under development. They use different route of administration none of them is oral because of the first pass effect and implement. They can be grouped into two broad categories based on the route of administration: Buccal/sublingual and nasal. Oral. Transmucosal. Lozenge. Effervescent Buccal. Tablet. Fentanyl Buccal. Soluble Film. Sublingual. Fentanyl. Intranasal. Fentanyl Sprayy. Fentayl Pectin. Nasal Spray")
23
BTcP Therapies: Early Absorption parameters
Actiq Effentora Onsolis Abstral Instanyl Nasalfent Dose (mcg) 400 50-200 Dwell Time (min) 15 15-20 N/A Cmax (ng/mL) 0.6 0.9 0.7 2.5 1.5 Tmax 120 (30–240) 45 (20–240) 60 - (23–240) (6-90) 20 (5-90) 23 23
 Dwell Time. (min) N/A. Cmax. (ng/mL) Tmax (30–240) 45. (20–240) (23–240) (6-90) 20. (5-90)")
24
Pts should be assessed for the presence of BtcP – D
Pts with BtcP should have this pain specifically assessed – D The management of BtcP should be individualized – D Consideration should be given to treatmetn of the underlying cause of pain – D Consideration should be given to avoidance of the precipitating factors – D Consideration shoulc be given to modification of the background analgesia - D Opioids are the rescue medication pf choice – D The dose should be determined by individual titration – B Non pharmacological methods may be useful – D Non-opioid analgesics may be useful – D Interventional techniques may be useful – D Pts should have BtcP re-assessed - D 24 24

26
26 26

27
Respiratory function during parenteral opioid titration
for cancer pain Estfan et al, Palliat Med 2007 Before titration Pain control Pain score Opioid dose

28
Significant relationship (p<0.001)
Dose of breakthrough oral opioid versus ATC dose from the four studies of OTFC Significant relationship (p<0.001) High variability 120 100 80 60 40 20 Hagen et al. J Palliat Med 2007 28
 High variability Hagen et al. J Palliat Med")
29
The dose of the oral rescue dose was on average 18% of the ATC dose
Zeppetella J. Opioids for cancer breakthrough pain: a pilot study reporting patient assessment of time to meaningful pain relief. JPSM 2008 50 pts 250 episodes The dose of the oral rescue dose was on average 18% of the ATC dose For OTFC, the rescue dose was approximately 36% of the ATC dose 29 29

30
OTFC versus IV-morphine for breakthrough pain.
Efficacy and safety of IV bolus of morphine for episodic (breakthrough) pain. Mercadante et al, JPSM, 2004 Intravenuos morphine for breakthrough pain in an acute pallliative care unit: a confirmatory study. Mercadante et al JPSM 2008 OTFC versus IV-morphine for breakthrough pain. Mercadante et al, Br J Cancer 2007
 pain. Mercadante et al, JPSM, Intravenuos morphine for breakthrough pain in an acute pallliative care unit: a confirmatory study. Mercadante et al JPSM OTFC versus IV-morphine for breakthrough pain. Mercadante et al, Br J Cancer")
31
293 episodi di BTcP trattati con P e T.
DOSING FENTANYL BUCCAL TABLET FOR BREAKTHROUGH CANCER PAIN: DOSE TITRATION VERSUS PROPORTIONAL DOSES. Mercadante et al, CMRO 2012 126 mg di equivalenti di morfina (range mg) per il dolore di base. 293 episodi di BTcP trattati con P e T. La necessità di ricorrere ad ulteriori dosi è stata maggiore nel gruppo T per il primo episodio (P< ). In pazienti che ricevevano dosi di morfina >120 mg/die, un numero significativo di pazienti ottenne una riduzione del dolore >50% nel gruppo P rispetto al gruppo T (p=0.040). Nessuna differenza di effetti collaterali
 per il dolore di base. 293 episodi di BTcP trattati con P e T. La necessità di ricorrere ad ulteriori dosi è stata maggiore nel gruppo T per il primo episodio (P< ). In pazienti che ricevevano dosi di morfina >120 mg/die, un numero significativo di pazienti ottenne una riduzione del dolore >50% nel gruppo P rispetto al gruppo T (p=0.040). Nessuna differenza di effetti collaterali.")
32
Pain intensity differences between the two groups for episodes of BTcP in patients receiving doses of oral morphine equivalents ≥120 mg/day (60 and 60 episodes in group P and T, respectively)
")
33
No differences in adverse effect intensity
Percentage of pts with adverse effects with an intensity of 1-2 on a 0-3 scale. No patient had intensity of 3

34
Conclusione Il BTcP di tipo incidente al movimento richiede un’ accurata valutazione sulle caratteristiche temporali di latenza e durata e persistenza dello stimolo, che si presentano in maniera molto diversa. Particolare attenzione dovrà essere posta sulle possibilità di trattamento delle metastasi ossee Dovranno essere considerati anche obiettivi realistici rispetto alle capacità di movimento ed alla prognosi. In base a tali caratteristiche si sceglierà il potenziamento dell’ analgesia di base con i mezzi farmacologici disponibili, e il farmaco al bisogno da utilizzare. Considerata l’ eterogeneità del BTcP, si dovrà personalizzare il trattamento 34 34

35
Breakthrough pain in elderly
No studies performed with the primary outcome of comparing adults and old patients. Experience provide infomation that that opioid tolerant patients can be treated with proportional doses safely. Perception of less tendency to call for BTcP events Studies ongoing

36
Sebastiano Mercadante

Similar presentations












 Experience AU EDITED FINAL: 03-18-13.>")
 Arya M Sharma, MD, FRCP(C) Professor of Medicine Research Chair for Obesity Research & Management University.>")





, DNB, FANZCA, MMEd. Director, Regional Anaesthesia Anaesthesia & Pain Medicine Royal Perth Hospital.>")


