Download presentation
Presentation is loading. Please wait.

1
Case 1 Two-day-old girl with bilious emesis.

4
There is abnormal position of the duodenum; and there is a corkscrew configuration of contrast as it passes through the proximal small bowel.

5
Malrotation /midgut volvulus Normally, a long, fixed small bowel mesenteric root attachment runs from the duodenojejunal junction in the left upper quadrant to the cecum in the right lower quadrant With malrotation, duodenojejunal and ileocecal junctions are malpositioned, with resulting short small bowel mesentery base prone to volvulus Malrotation also predisposes to duodenal obstruction due to paraduodenal hernias or Ladd bands (peritoneal reflections crossing duodenum and extending to the inferior liver or posterior wall of the abdomen) Compromise of superior mesenteric vessels may occur with volvulus, which can result in small bowel ischemia and necrosis. Midgut volvulus results in death in at least 15% of cases High incidence of morbidity in survivors from short gut syndrome and dependence on TPN leading to cirrhosis May present at any age, but 60% present by one month of age Present with bilious vomiting Diagnose with upper GI: Malrotation: –Abnormally positioned duodenojejunal junction Right of spine Inferior to the duodenal bulb –Jejunum in the right abdomen Midgut Volvulus: –Proximal small bowel obstruction or corkscrew pattern as contrast traverses the proximal jejunum in right or mid upper abdomen Treatment is surgical

6
Case 2 Routine prenatal ultrasound in healthy thirty-year-old.

9
Findings: There is a large occipital encephalocele, containing mixed solid and cystic areas. The calvarial defect is between 1-2 cm, through which brain tissue is seen to herniate Differential Diagnosis: Occipital encephalocele Cystic hygroma Teratoma Branchial cleft cyst Scalp edema Epidermal scalp cyst

10
Occipital encephalocele: An encephalocele results from failure of the surface ectoderm to separate from the neuroectoderm. The final result is a bony defect in the skull table, which allows herniation of the meninges (cranial meningocele) or herniation of brain tissue. Encephaloceles represent 10-15% of all neural tube defects. Of encephaloceles, occipital encephaloceles are most common (75-80%). 90% are midline. The absence of brain tissue within the herniated sac is the single most favorable prognostic feature for survival.
 or herniation of brain tissue. Encephaloceles represent 10-15% of all neural tube defects. Of encephaloceles, occipital encephaloceles are most common (75-80%). 90% are midline. The absence of brain tissue within the herniated sac is the single most favorable prognostic feature for survival..")
11
Case 3 Woman with breast cancer.

14
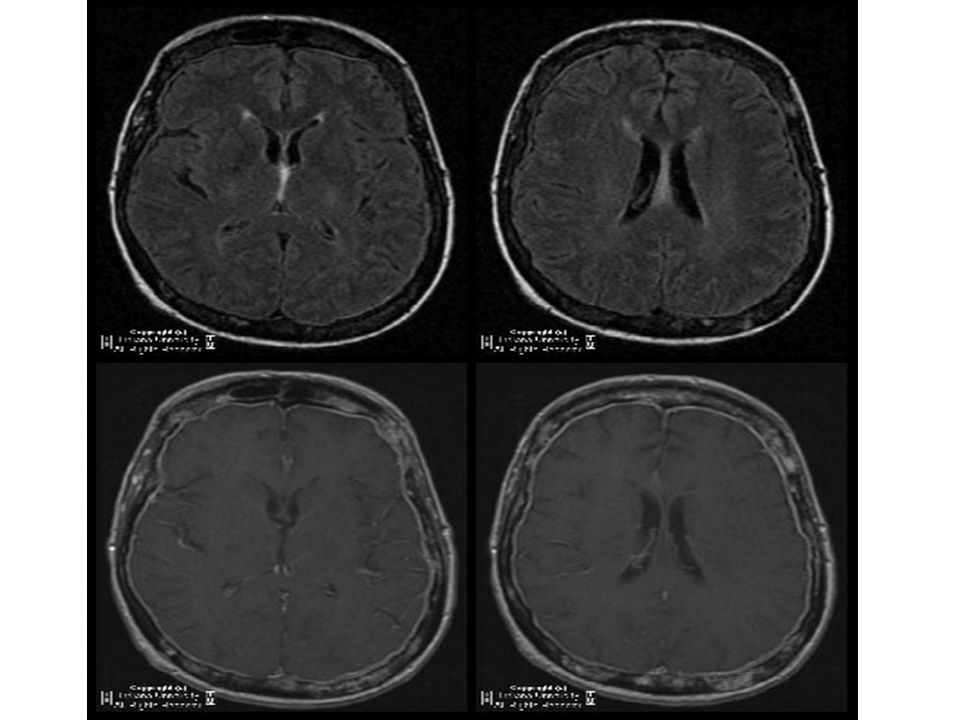
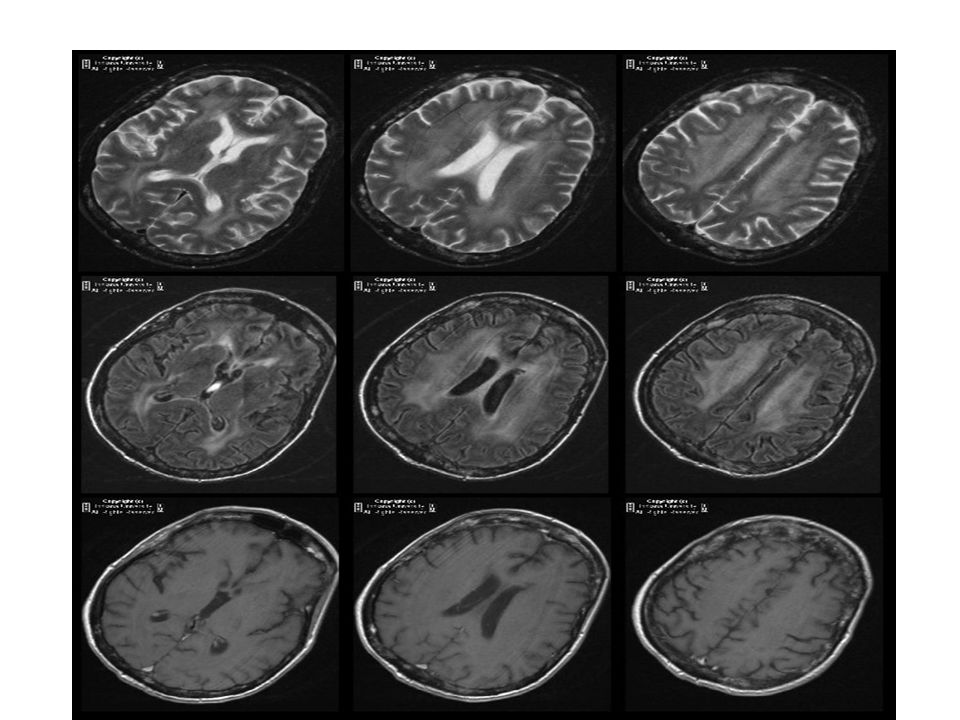
Findings: Initial MRI of the brain shows numerous enhancing lesions scattered throughout the calvarium, consistent with metastatic bony involvement. There is also diffuse enhancement of the pachymeninges. There are no enhancing parenchymal lesions. Newer MRI of the brain shows confluent periventricular deep white matter FLAIR and T2 hyper intensities. There are no abnormal parenchymal lesions or enhancement. There is mild volume loss. There was no restricted diffusion (images not shown) to suggest infarct. Again seen are heterogeneous and enhancing calvarial lesions. Differential Diagnosis: Post radiation white matter disease Microvascular disease Age related white matter changes Tumor edema from metastatic or primary neoplasm Diffuse infectious process Diffuse inflammatory process Diagnosis: Post radiation white matter injury. Metastatic disease to the calvarium.
 to suggest infarct. Again seen are heterogeneous and enhancing calvarial lesions. Differential Diagnosis: Post radiation white matter disease Microvascular disease Age related white matter changes Tumor edema from metastatic or primary neoplasm Diffuse infectious process Diffuse inflammatory process Diagnosis: Post radiation white matter injury. Metastatic disease to the calvarium..")
15
Case 4

19
Findings: Salient findings include overgrowth of the soft tissues and bones of the fourth and fifth digits with tuft expansion, periarticular osseous projections and degenerative changes of the interphalangeal joints. Diagnosis: Macrodystrophia lipomatosa

20
Differential diagnosis: –Neurofibromatosis –Klippel – Trenaunay – Weber syndrome –Lymphangiomatosis –Hemangiomatosis – Macrodystrophia lipomatosa –Fibrolipomatous hamartoma of the nerve

21
Case 5

25
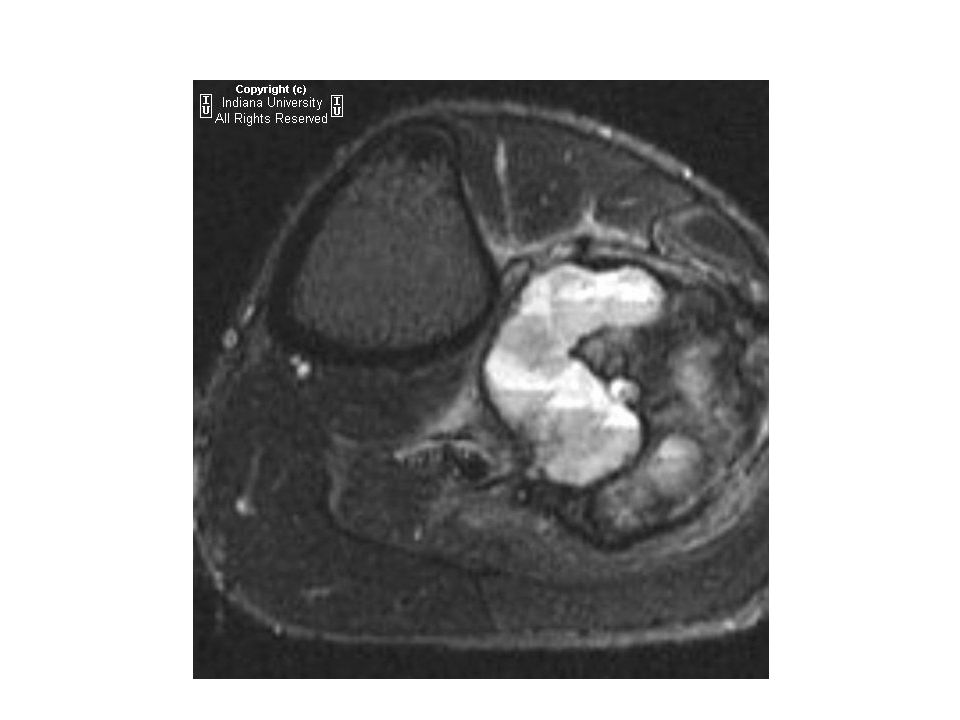
Findings: Plain films show an aggressive appearing permative destructive mass involving the proximal fibula. On the MRI, there is a lobulated, heterogeneous mass that extends superiorly to the growth plate, but not into the growth plate. There is mixed signal throughout the lesion. There is periosteal reaction and abnormal enhancement within bone marrow of the fibula distal to the tumor. Blood-fluid levels are evident, consistent with telangiectatic osteosarcoma. Diagnosis: Telangiectatic osteosarcoma

26
Differential diagnosis: –Sarcomatous tumors: Osteosarcoma Ewings Sarcoma Angiosarcoma Fibrosarcoma Malignant fibrous histiocytoma –Lymphoma –Giant cell tumor (GCT) –Metastasis
 –Metastasis")
27
Case 6

30
Findings: IVP demonstrates a dilated distal left ureter with mild tortuosity and a filling defect in the left bladde

31
Diagnosis: Transitional cell carcinoma of bladder

Similar presentations