Download presentation
Presentation is loading. Please wait.

1
Congenital heart disease in adults Heart Disease Braunwald CV R4 李威廷醫師 Supervisor: 詹世鴻醫師

2
Pregnancy Maternal risk: Pulmonary hypertension Obstructive lesions (LVOTO, RVOTO) Ventricular dysfunction Heart failure Ascending aortic aneurysm (Marfan syndrome)
 Ventricular dysfunction Heart failure Ascending aortic aneurysm (Marfan syndrome)")
3
ASD (atrial septal defect) Ostium primum Ostium secundum Sinus venousus: SVC / IVC LA and RA, abnormal pulmonary venous drainage (usually right lung) Coronary sinus
 Ostium primum Ostium secundum Sinus venousus: SVC / IVC LA and RA, abnormal pulmonary venous drainage (usually right lung) Coronary sinus")
4
ASD (atrial septal defect) Qp/Qs > 1.5: symptoms (+) Effort dyspnea (exercise intolerance) Palpitation (Af/AF) Paradoxical embolism Pulmonary hypertension Eisenmenger syndrome Systolic murmur at left 2 nd insterconstal space mid-diastole rumble at LLSB (tricuspid flow)
 Qp/Qs > 1.5: symptoms (+) Effort dyspnea (exercise intolerance) Palpitation (Af/AF) Paradoxical embolism Pulmonary hypertension Eisenmenger syndrome Systolic murmur at left 2 nd insterconstal space mid-diastole rumble at LLSB (tricuspid flow)")
5
ASD (atrial septal defect) EKG: SR / Af / AF; RBBB CXR: cardiomegaly, dilated PA Echo: TTE, TEE Cath: Qp / Qs, PA pressure
 EKG: SR / Af / AF; RBBB CXR: cardiomegaly, dilated PA Echo: TTE, TEE Cath: Qp / Qs, PA pressure")
6
ASD (atrial septal defect) Nonsignificant (Qp / Qs <1.5): not require closure Significant ASD (Qp / Qs> 1.5 or RV volume overload): surgical intervention Device closure: Surgery: Reduce CHF, improve exercise status, not prevent Af
 Nonsignificant (Qp / Qs <1.5): not require closure Significant ASD (Qp / Qs> 1.5 or RV volume overload): surgical intervention Device closure: Surgery: Reduce CHF, improve exercise status, not prevent Af")
7
Isolated ventricular septal defect Muscular VSD Membranous VSD Doubly committed subarterial or outlet VSD

8
Isolated ventricular septal defect Restrictive VSD: Qp/Qs <1.5, no s/s Moderately restrictive VSD: Qp/Qs =1.5-2.5, with s/s (LA and LV dilate, elevated PA, dyspnea, S3, holosystolic murmur) Nonrestrictive VSD: Eisenmenger syndrome Apical diastolic rumble and S3
 Nonrestrictive VSD: Eisenmenger syndrome Apical diastolic rumble and S3")
9
Isolated ventricular septal defect EKG: Af, deep Q+ tall R + tall T in V5, V6 (LV overload) CXR: dilated PA Echo: TTE Cath: Qp / Qs, PA pressure
 CXR: dilated PA Echo: TTE Cath: Qp / Qs, PA pressure")
10
Isolated ventricular septal defect Interventional indication: Significant VSD (Qp/Qs >1.5, PA> 50mmHg, LA, LV dilate, LV function deterioration) Absence of irreversible pulmonary HTN Reduce AR, IE, slightly increase intraventricular conduction delay
 Absence of irreversible pulmonary HTN Reduce AR, IE, slightly increase intraventricular conduction delay")
11
Atrioventricular septal defect (AVSD)
")
12
EKG: 1 st degree AVB / LAFB / CAVB, Af /AF CXR: cardiomegaly, enlarged LA Echo: AR, subaortic stenosis, Cath: PA pressure, intracardiac shunt, aubaortic stenosis severity Intervention indication: hemodynamic defects, atrial arrhythmia, LV or RV dysfunction, reversible pulmonaru hypertension, trans-AV PG> 50mmHg

13
Patent ductus arteriosus 1: 2000—1:5000 6th primitive aortic arch Proximal PA descending AO Increase IE (murmur) LA and LV volume overload Continuous “machinery” murmur
 LA and LV volume overload Continuous machinery murmur")
14
Patent ductus arteriosus EKG: deep Q+ tall R + tall T in V5, V6 (LV volume overload) CXR: cardiomegaly, LA, LV dilate Echo: TTE (suprasternal or parasternal short axis), systolic and diastolic flow toward the pulmonary valve in the main pulmonary artery
 CXR: cardiomegaly, LA, LV dilate Echo: TTE (suprasternal or parasternal short axis), systolic and diastolic flow toward the pulmonary valve in the main pulmonary artery")
15
Patent ductus arteriosus Intervention: PAP > 2/3 SAP, PAR > 2/3 SAR, Qp/Qs >1.5, evidence of PA reactivity with challenged to vasodilator (O2, NO) Irreversible pulmonary HTN (x) Active endarteritis (x) Transcatheter: Surgery:
 Irreversible pulmonary HTN (x) Active endarteritis (x) Transcatheter: Surgery:")
16
Bicuspid aortic valve 1-2% of population Male: female= 4:1 20% with coarctation of AO and PDA Late aortic stenosis at 60+ y/o Increase IE

17
Bicuspid aortic valve EKG: from normal to LVH CXR: ascending aorta dilatation, valvular calcification Echo: concomitant defects such as coarctation or dissection of aorta

18
Bicuspid aortic valve Interventional indication: AS: dyspnea, angina, syncope, <0.6cm 2, AR: AO root >55mm: prophylactic surgery Balloon valvuloplasty surgery

19
Subaortic stenosis AS, LVH, mild-moderate AR IE Systolic murmur at mid-left sternal edge Indication for intervention: pressure gradient >50mmHg, progressive or moderate to severe AR

20
Coarctation of the aorta Simple coarctation: Complex coarctation: combine other lesions (bicuspid aortic valve, intracranial aneurysm, and acquired intercostal artery aneurysm) Significant coarctation: trans-lesion pressure gradient >20mmHg or proximal hypertension
 Significant coarctation: trans-lesion pressure gradient >20mmHg or proximal hypertension")
21
Coarctation of the aorta Epistaxis, headache, leg weakness on exertion Leg claudication is rare (in abdominal coarctation) Brachial pressure> popliteal pressure 10mmHg Widespread cresendo-decresendo systolic murmur at chest wall “Corkscrew” torturosity of retinal artery
 Brachial pressure> popliteal pressure 10mmHg Widespread cresendo-decresendo systolic murmur at chest wall Corkscrew torturosity of retinal artery")
23
Coarctation of the aorta Interventional indication: Arm > leg systolic BP 10mmHg Radial-femoral pulse delay Peak trans-coarctation pressure gradient >20mmHg Surgery Transcatheter

24
Right ventricular outflow tract obstruction (RVOTO) Isolated or combining other syndrome Valvar RVOTO (pulmonary stenosis): most common Subvalvar RVOTO Supravalvar RVOTO Exertional fatigue, dyspnea, lightheadedness, chest discomfort (RV angina) Normal S1, splitting S2 with diminished P2 Systolic murmur at left 2 nd insterconstal space
 Isolated or combining other syndrome Valvar RVOTO (pulmonary stenosis): most common Subvalvar RVOTO Supravalvar RVOTO Exertional fatigue, dyspnea, lightheadedness, chest discomfort (RV angina) Normal S1, splitting S2 with diminished P2 Systolic murmur at left 2 nd insterconstal space")
26
Right ventricular outflow tract obstruction (RVOTO) EKG: RAE, RVH CXR: dilated common and left pulmonary artery Echo: Cath: Intervention indication: peak RVOT pressure gradient >50mmHg or symptomatic RVOTO Ballooin valvuloplasty or surgical valvotomy
 EKG: RAE, RVH CXR: dilated common and left pulmonary artery Echo: Cath: Intervention indication: peak RVOT pressure gradient >50mmHg or symptomatic RVOTO Ballooin valvuloplasty or surgical valvotomy")
27
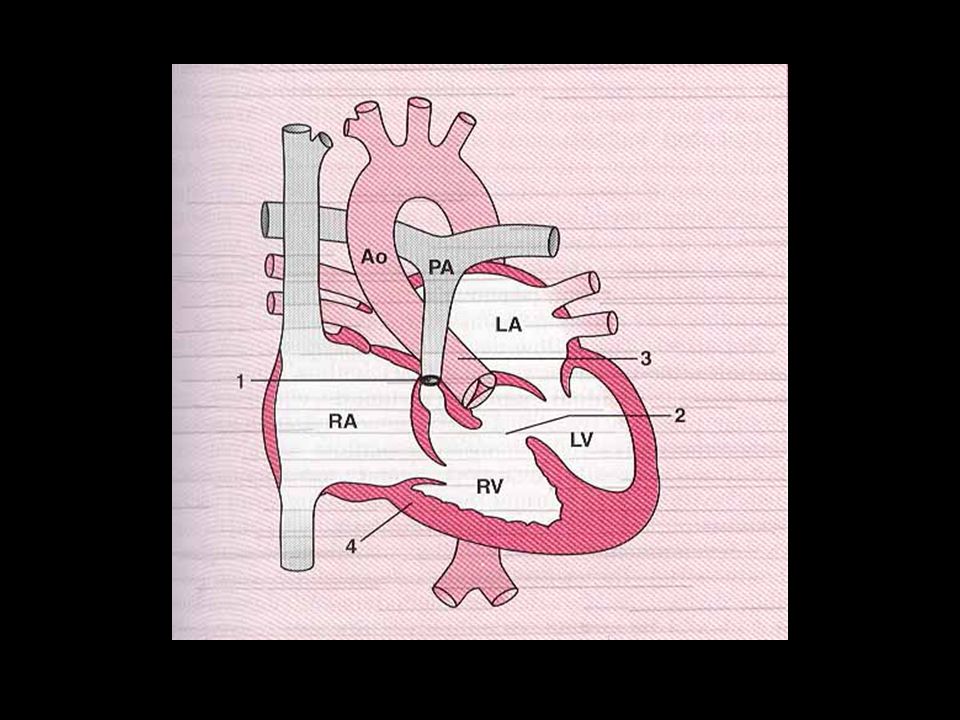
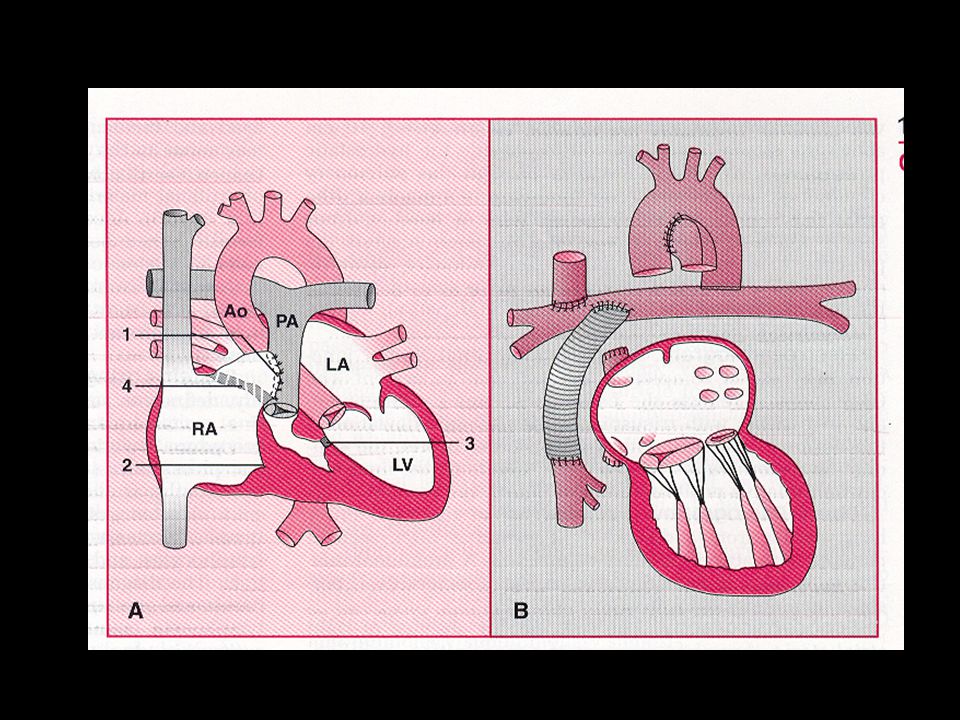
Ebstein anomaly

28
Apical displacement of the septal, posterior, or (rarely) anterior leaflet of the tricuspid valve “Atrialization” of the inflow tract of RV Small functional RV Asymtomatic all the life in some patients Exercise intolerance, supraventricular arrhythmia, cyanosis (R L shunt at atrial level)
 anterior leaflet of the tricuspid valve Atrialization of the inflow tract of RV Small functional RV Asymtomatic all the life in some patients Exercise intolerance, supraventricular arrhythmia, cyanosis (R L shunt at atrial level)")
29
Ebstein anomaly Wide splitting S1 (sail-sound), Wide splitting S2 (RBBB), Right-sided S3 EKG: Af / AF, RAE, RBBB CXR: “water-bottle” appearance Echo: apical displacement of tricuspid valve (8mm/m 2 )
, Wide splitting S2 (RBBB), Right-sided S3 EKG: Af / AF, RAE, RBBB CXR: water-bottle appearance Echo: apical displacement of tricuspid valve (8mm/m 2 )")
30
Ebstein anomaly Interventional indication: NYHA class III or IV Progressive cyanosis Right heart failure Paradoxical embolite Recurrent SVT or asymptomatic cardiomegaly (C/T ratio >65%) (relative indication)
 (relative indication)")
31
Tetralogy of Fallot Non-restrictive VSD Overriding aorta RVOT obstruction Consequent RVH ASD (pentalogy)
")
33
Tetralogy of Fallot Surgical at childhood Palliation: shunt Blalock-Taussig shunt : subclavian artery PA Wasteon shunt : ascending AO to right PA Potts shunt : descending AO to left PA Central interposition tube graft Repair VSD & relieving RVOT obstruction

34
CVA, endocarditis, supraventricular tachycardia, AR LVH, LV failure Fonton procedure: when biventricular repair is impossible direct atrio-pulmonary connection ideal candidates : pre-op mean PA <= 15mmHg pulmonary resistance <=4 units/m 2 pulmonary artery-aortic diameter ratio >= 0.75 systemic ventricular ejection fraction >= 60% MR <= mild

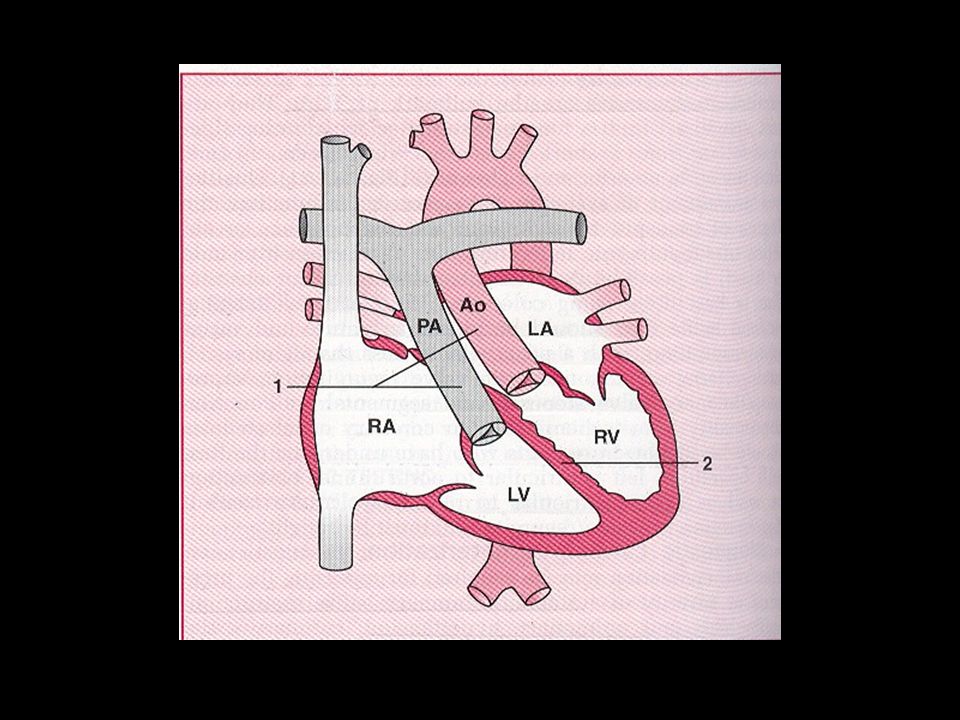
36
Complete transposition of the great arteries Simple transposition Complex transposition: VSD, PS Survival before surgical repair is dependent on mixing of the circulations at one level by natural (ASD, VSD, PDA) or intervention
 or intervention")
38
Complete transposition of the great arteries Atrial switch: change venous return Arterial switch: change artery Two-stage arterial switch Rastelli procedure: LV VSD AO RV tunnel PA Cardiac transplantation

39
Complete transposition of the great arteries EKG: AF, sinus bradycardia or junctional rhythm, RVH, RAD, without RA overload, or normal (post- arterial switch) CXR: “egg on its side” (post-atrial switch) Echo: parallel great vessels (post-atrial switch) tunnel (post-Rastelli operation) Cath
 CXR: egg on its side (post-atrial switch) Echo: parallel great vessels (post-atrial switch) tunnel (post-Rastelli operation) Cath")
40
Congenitally corrected transposition of the great arteries Rare, <1% RA MV LV PA LA TV RV AO VSD (75%), PS (75%), Ebstein-like anomaly (>75%)
, PS (75%), Ebstein-like anomaly (>75%)")
42
Congenitally corrected transposition of the great arteries EKG: CAVB, delta-wave (anomaly of left-sided AV valve) CXR: left-sided ascending aorta rising to the aortic knuckle Echo: bi-leaflet AV valve, Ebstein-like malformation Cath
 CXR: left-sided ascending aorta rising to the aortic knuckle Echo: bi-leaflet AV valve, Ebstein-like malformation Cath")
43
Congenitally corrected transposition of the great arteries Interventional or re-intervention indication: Moderate or severe systemic (tricuspid ) AV valve regurgitation valve replacement Left AV valve replacement under RVEF>45% End-stage symptomatic heat failure heart transplantation VSD (Qp/Qs>1.5) or PS (>50mmHg) correction CAVB permanent pacemaker (epicardial, DDD)
 AV valve regurgitation valve replacement Left AV valve replacement under RVEF>45% End-stage symptomatic heat failure heart transplantation VSD (Qp/Qs>1.5) or PS (>50mmHg) correction CAVB permanent pacemaker (epicardial, DDD)")
44
Eisenmenger syndrome R L shunt or bidirectional shunts “Differnetial cyanosis” Complication: CHF (most often), sudden death, hemoptysis EKG: RAE, RVH, RAD, atrial arrhythmia Restore physiological balance Avoid unnecessary surgery Heart-lung transplantation
, sudden death, hemoptysis EKG: RAE, RVH, RAD, atrial arrhythmia Restore physiological balance Avoid unnecessary surgery Heart-lung transplantation")
45
Eisenmenger syndrome CCB ACEI Prostacyclin Pulmonary artery banding

46
Medical managekent of cyanotic congenital heart disease Hyperviscosity syndrome Iron deficiency Hemostatic abnormalities Cerebrovascular events: infarction or hemorrhage Renal dysfunction

Similar presentations

















 tricuspid valve 2. Hypoplastic right ventricle 3. Ventricular septal defect 4. Atrial.>")




