Download presentation
Presentation is loading. Please wait.

1
PRINCIPLES OF DIALYSIS DR SAAD ALSHOHAIB ASSOCIATE PROFESSOR IN MEDICINE AND NEPHROLOGY KAUH

2
Dialysis in Saudi Arabia There are 6700 patients on dialysis in Saudi Arabia There is 130 haemodialysis centres in Saudi Arabia The incidence of hepatitis B is 6.7%and 50% for HCV SCOT data Saudi J kid 2001 12 (3)
")
3
Dialysis in the Kingdom It had been estimated that the number of dialysis patients would exceed 10000 patients in the year 2010 Most centres are saturated and need to expand in order to accept new patients There is a great need for CAPD in Saudi Arabia SCOT data Saudi J kid 2001 12 (3)
")
5
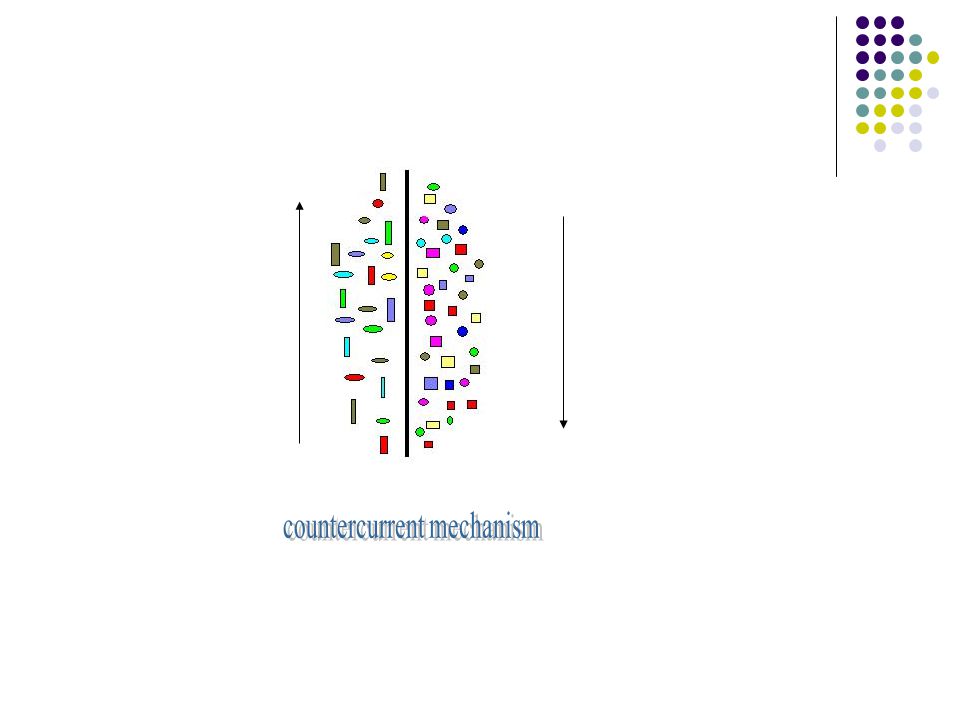
Principles of dialysis The exchange will depend on Concentration Size and binding Speed Membranes pores Time pressure

10
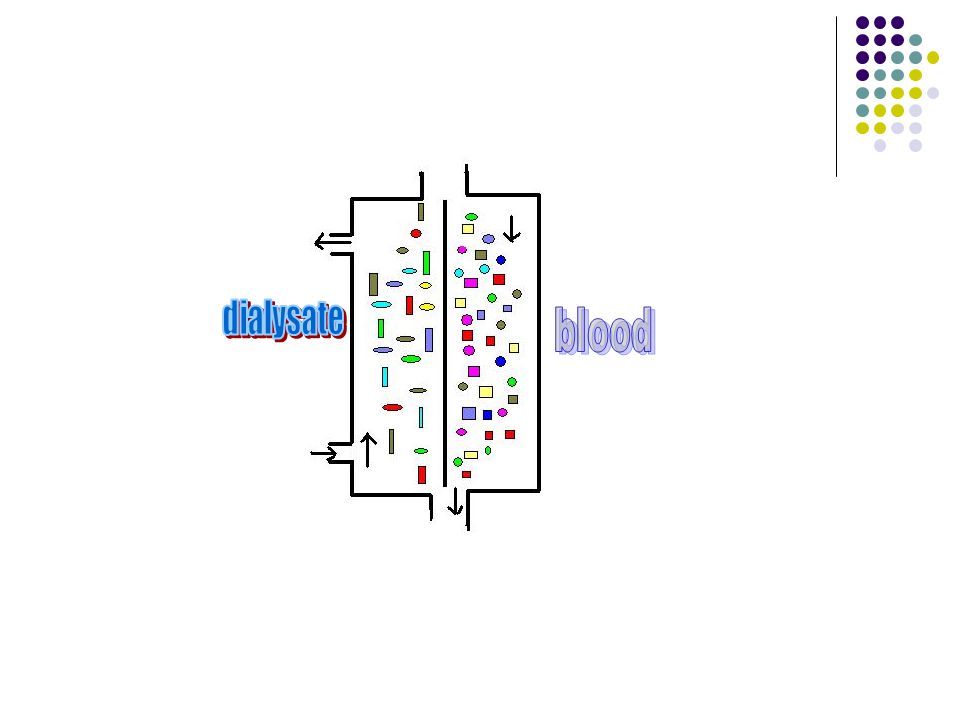
Dialysate Treated water is mixed with an electrolyte solution Na 135---145 K 0 -- 4 Ca variable HCO 3 35 Mg.5-- 1

11
MEMBRANES Cellulose Substituted cellulose ( acetate ) Cellulose synthetic ( amino group added ) Synthetic (PAN polysulfone )
 Cellulose synthetic ( amino group added ) Synthetic (PAN polysulfone )")
12
COMPLEMENT Cellulose membranes activate complement and this reduced by using more compatible membranes

13
prescription Blood flow Time Membrane type Fluid removal Electrolytes

14
DRY WEIGHT WELL KNOWN CONCEPT BUT MANY PITTFALLS WITH PRACTICAL APPLICATION LOW DRY WT LEAD TO FATIGUE WEAKNESS AND LETHARGY HIGH DRY WT LEAD TO HYPERTENSION

15
DRY WEIGHT When patient appetite improve with adequate dialysis their weight improve then tend to be hypotensive Inadequate dialysis lead to decreased appetite and loss of wt these patients present with sever hypertension and possibly pulmonary edema Patient may share in the decision of the dry wt

16
Hypertension and dry wt Hypertension is mostly volume related Hypertension at the beginning of dialysis and improving toward the end is usually volume dependent and respond to fluid removal Hypertension at the end of dialysis may respond to ACE inhibitors

17
Adequacy Kt/v is a good marker but not the only one Monitor the phosphate PTH serum albumin BUN Cr and Hgb The wellbeing of the patient and his general condition and ability to perform activity are important markers of adequate dialysis Good appetite and nutrition are important markers

18
Chronic dialysis prescription Prescription should be individualized according to patient weight sex age and residual renal function Cardiac status is important in determining blood flow Choice of membrane would depend on the facilities expertise and availability of support services

19
Predialysis urea Value higher than expected Increased protein intake G I bleed Decreased residual renal function Decreased dialysis efficiency Value lower than expected Malnutrition Chronic illness Liver disease Wrong sampling

20
Prognosis Good prognosis Cholesterol value 200—250 Being obese Normal albumin Adequate dialysis Bad prognosis Very low urea an Cr Low albumin Low K Low cholesterol High PTH and P Old age DM

21
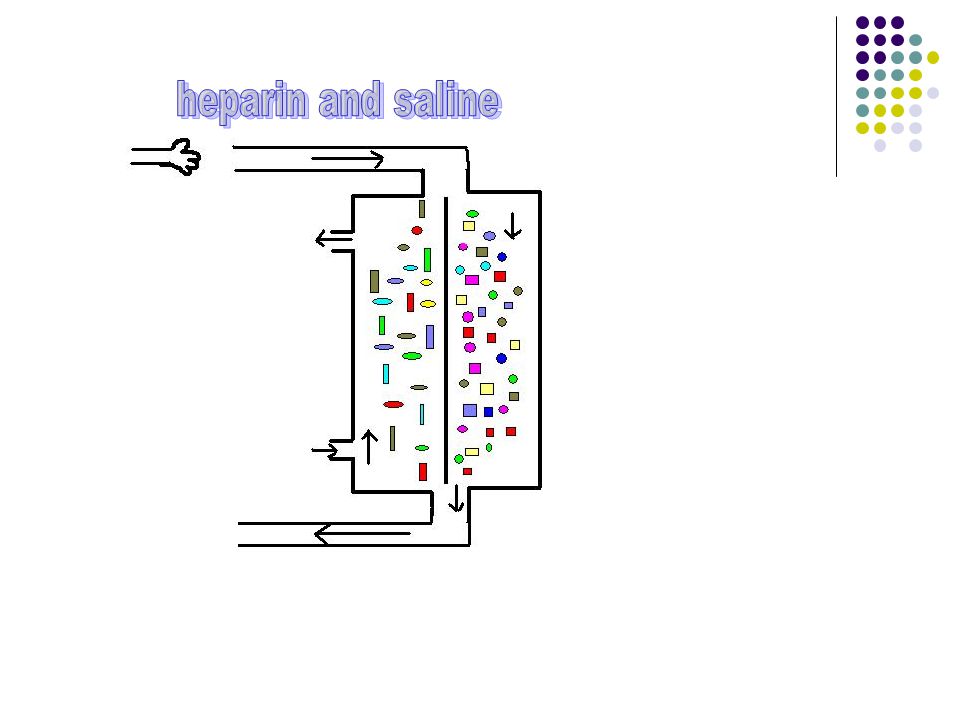
Anticoagulation Heparin is usually used to maintain an ACT of 1.5 -- 1.8 Heparin is usually as a bolus followed by infusion Stop heparin at the last hour of dialysis Contraindications include pericarditis recent surgery active bleeding and thrombocytopenia

22
Hypotension during dialysis High UF rate Fluctuation in UF rate Dry weight set too low Low dialysis Na Warm dialysis solution Food ingestion Diabetic neuropathy Antihypertensive meds Poor cardiac status

23
Hypotension prevention Decrease intradialytic weight gain Adjust dry weight Keep dialysate Na at or above serum value No antihypertensive before dialysis May need to avoid feeding certain patients on dialysis

24
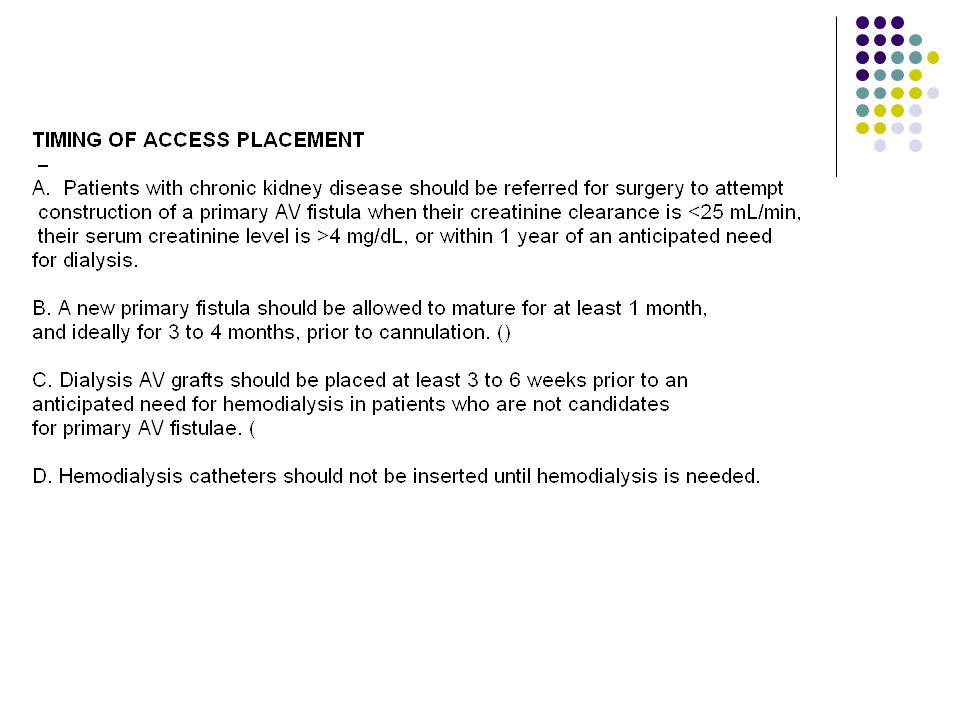
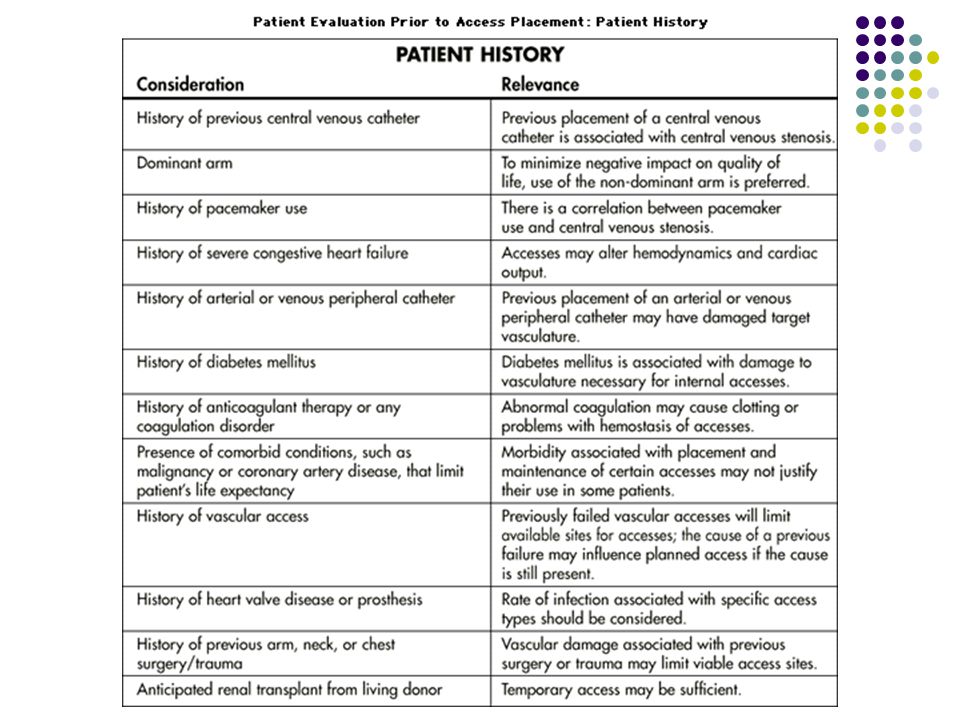
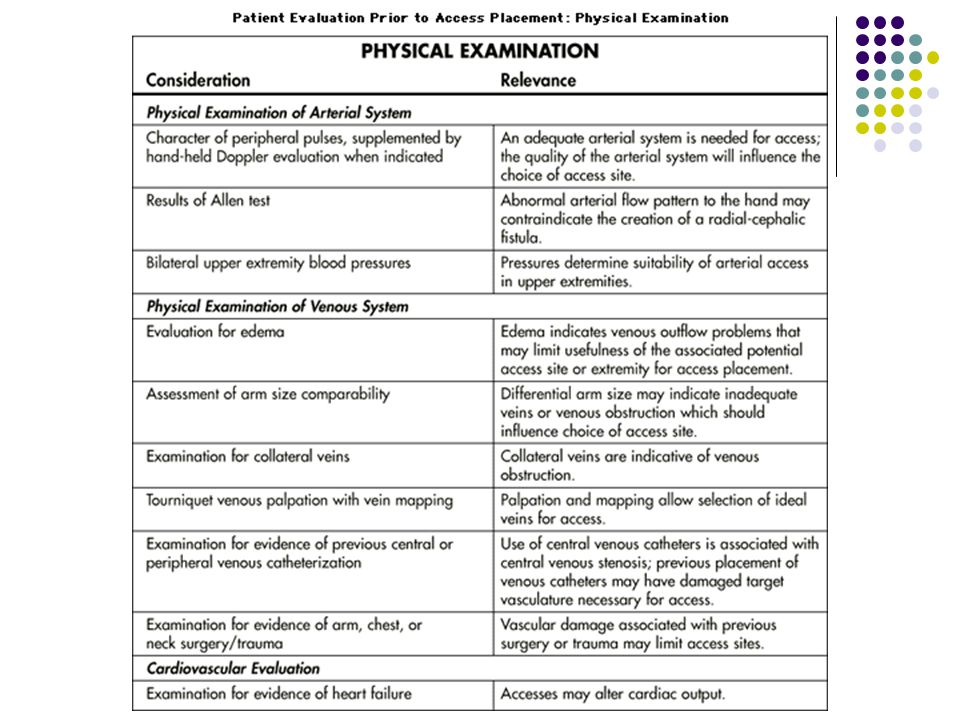
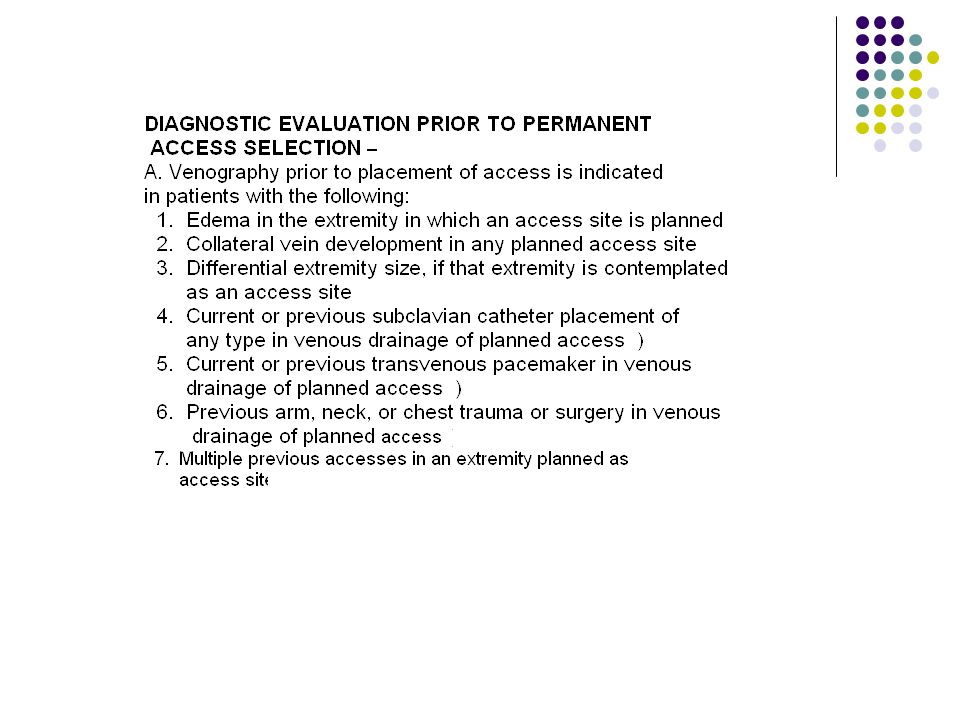
CRF There are three types of access for dialysis AV fistula Graft Central line

34
Improving patient lifetime on therapy AccessAdequacy Nutrition Compliance QoL Infection control

35
Complications of Renal Failure Hypertension Sodium Retention/Fluid Accumulation Anemia Dyspnoea Electrolyte Imbalance Acidosis Uraemic Syndrome

36
Uraemic Syndrome Loss of Appetite Nausea Change in Taste Fatigue Sleep Disorders Mental Changes Neuropathy Anemia Itching Acidosis Shortness of Breath

37
Withdrawal or No Treatment Some patients may not be able to psychologically accept dialysis. An elderly patient with co-morbid conditions may not be accepted for therapy. Medical conditions may preclude therapy. Medical team, patient and patient family will discuss treatment alternatives.

Similar presentations




activate vitamin D (renal 1-alpha hydroxylase) produces erythropoietin.>")










.>")




