Download presentation
Presentation is loading. Please wait.

1
Patient Safety Culture
Andrea McGuinness Since the publication of An Organisation with a Memory [10] there has been a growing interest in the topic of safety culture within the NHS. Research has shown that factors such as an emphasis on production, efficiency and cost, or professional norms for perfectionism among healthcare providers may combine to create a culture contradictory to the requirements of patient safety [30]. The establishment of a “no-blame” culture within the NHS that facilitates the reporting of and the learning from incidents has become one of the cornerstones of patient safety improvements. There is now awareness that major cultural transformations must accompany structural and procedural changes in order to achieve and sustain desired improvements in quality and safety of care [31]. Healthcare organisations need to learn about organisational deficiencies that may cause latent failure conditions in the work environment © 2014 AQuA

2
‘A safety culture is where staff within an organisation have a constant and active awareness of the potential for things to go wrong. Both the staff and the organisation are able to acknowledge mistakes, learn from them, and take action to put things right.’ The notion of safety culture was first explored in safety-critical industries following major disasters, most notably the Chernobyl nuclear accident in 1986 [32]. A common definition of safety culture in the nuclear industry that is now widely adopted across industries suggests that: “The safety culture of an organisation is the product of individual and group values, attitudes, perceptions, competencies and patterns of behaviour that determine the commitment to, and the style and proficiency of, an organisation’s health and safety management. Organisations with a positive safety culture are characterised by communications founded on mutual trust, by shared perceptions of the importance of safety and by confidence in the efficacy of preventive measures.” [33] Safety culture can be described as “the way safety is done around here”, emphasising the importance of understanding what people actually believe and do [34]. What people believe about safety and the importance given to safety within an organisation will strongly influence their decisions, and these beliefs and attitudes are shaped by individual experience and by interacting with and observing peers [32]. In the literature there is a distinction between safety culture and safety climate. Safety climate commonly refers to more readily measurable aspects of safety culture [35] and can be regarded as the surface features of the underlying safety culture [36]. Assessment of safety climate is becoming increasingly popular and is conducted using quantitative safety climate questionnaires. A deeper understanding of safety culture requires qualitative methods as it is concerned with the more enduring underlying culture [32]. In healthcare, the quantitative assessment of safety climate using questionnaires is an established approach and recommended by bodies such as the Joint Commission [34]. Such assessments can be used to [30]: • Identify areas for improvement and raise awareness about patient safety • Evaluate patient safety interventions and track changes over time • Conduct internal and external benchmarking • Fulfil directives and regulatory requirements

3
‘The safety culture of an organisation is the product of individual and group values, attitudes, perceptions, competencies, and patterns of behaviour that determine the commitment to, and the style and proficiency of, an organisation’s health and safety management. Organisations with a positive safety culture are characterised by communications founded on mutual trust, by shared perceptions of the importance of safety, and by confidence in the efficacy of preventive measures.’ Organising for Safety: Third Report of the ACSNI (Advisory Committee on the Safety of Nuclear Installations) Study Group on Human Factors. Health and Safety Commission (of Great Britain). Sudbury, England: HSE Books, 1993. © 2014 AQuA
 Study Group on Human Factors. Health and Safety Commission. (of Great Britain). Sudbury, England: HSE Books, © 2014 AQuA.")
4
A framework for the measurement and monitoring of safety
Has patient care been safe in the past? Ways to monitor harm include: mortality statistics (including HSMR and SHMI) record review (including case note review and the Global Trigger Tool) staff reporting (including incident report and ‘never events’) routine databases. Are our clinical systems and processes reliable? Ways to monitor reliability include: percentage of all inpatient admissions screened for MRSA percentage compliance with all elements of the pressure ulcer care bundle. Is care safe today? Ways to monitor sensitivity to operations include: safety walk-rounds using designated patient safety officers meetings, handovers and ward rounds day-to-day conversations staffing levels patient interviews to identify threats to safety. Will care be safe in the future? Possible approaches for achieving anticipation and preparedness include: risk registers safety culture analysis and safety climate analysis safety training rates sickness absence rates frequency of sharps injuries per month human reliability analysis (e.g. FMEA) safety cases. Are we responding and improving? Sources of information to learn from include: automated information management systems highlighting key data at a clinical unit level (e.g. medication errors and hand hygiene compliance rates) at a board level, using dashboards and reports with indicators, set alongside financial and access targets. A framework for the measurement and monitoring of safety Source: Vincent C, Burnett S, Carthey J. The measurement and monitoring of safety. The Health Foundation, 2013
 record review (including case note review and the Global Trigger Tool) staff reporting (including incident report and ‘never events’) routine databases. Are our clinical systems and processes reliable Ways to monitor reliability include: percentage of all inpatient admissions screened for MRSA. percentage compliance with all elements of the pressure ulcer care bundle. Is care safe today Ways to monitor sensitivity to operations include: safety walk-rounds. using designated patient safety officers. meetings, handovers and ward rounds. day-to-day conversations. staffing levels. patient interviews to identify threats to safety. Will care be safe in the future Possible approaches for achieving anticipation and preparedness include: risk registers. safety culture analysis and safety climate analysis. safety training rates. sickness absence rates. frequency of sharps injuries per month. human reliability analysis (e.g. FMEA) safety cases. Are we responding and improving Sources of information to learn from include: automated information management systems highlighting key data at a clinical unit level (e.g. medication errors and hand hygiene compliance rates) at a board level, using dashboards and reports with indicators, set alongside financial and access targets. A framework for the measurement and monitoring of safety. Source: Vincent C, Burnett S, Carthey J. The measurement and monitoring of safety. The Health Foundation,")
5
Attributes of high reliability organisations
Continuous attitude to improvement Learning culture Highly trained Rewarded staff Flexibility to deal with change ‘Collective mindfulness’ about safety issues Leadership and frontline staff take a shared responsibility for ensuring care is delivered safely In order to try and answer this question the Health Foundation commissioned an evidence scan into the characteristics of ‘high reliability organisations’. These organisations work in hazardous environments like healthcare or aviation, but successfully find ways to minimise risk.

6
How do we build a safety culture?
Sir Stephen Moss (Day 3) ‘developing a safety culture doesn’t happen overnight’. Martin Bromley ‘culture change isn’t about doing one thing – it’s about doing lots of little things consistently and with purpose (whilst maintaining coordination).’ SRFT consistent leadership, building a sense of individual responsibility at every level. Most experience shows that there is no quick fix. In Sir Stephen Moss’ words, ‘developing a safety culture doesn’t happen overnight’. Organisations need to be in it for the long haul. Perhaps one of the reasons that Salford Royal is succeeding is that there’s been a consistent focus from a stable senior leadership team over the last decade. Working to build a sense of individual responsibility for safety issues in staff at every level has also been key. As Martin Bromley points out in a recent Health Foundation blog, ‘culture change isn’t about doing one thing – it’s about doing lots of little things consistently and with purpose (whilst maintaining coordination).’ Measuring how good the safety culture is within an organisation helps to provide a starting point for change. Increasingly NHS organisations concerned with improving safety are using tools such as climate surveys to monitor the attitudes of staff to safety issues and identify areas for development. Patient complaints and feedback are also being looked at more carefully, and patients and families are being more formally involved in improvement work.
 ‘developing a safety culture doesn’t happen overnight’. Martin Bromley. ‘culture change isn’t about doing one thing – it’s about doing lots of little things consistently and with purpose (whilst maintaining coordination).’ SRFT. consistent leadership, building a sense of individual responsibility at every level. Most experience shows that there is no quick fix. In Sir Stephen Moss’ words, ‘developing a safety culture doesn’t happen overnight’. Organisations need to be in it for the long haul. Perhaps one of the reasons that Salford Royal is succeeding is that there’s been a consistent focus from a stable senior leadership team over the last decade. Working to build a sense of individual responsibility for safety issues in staff at every level has also been key. As Martin Bromley points out in a recent Health Foundation blog, ‘culture change isn’t about doing one thing – it’s about doing lots of little things consistently and with purpose (whilst maintaining coordination).’ Measuring how good the safety culture is within an organisation helps to provide a starting point for change. Increasingly NHS organisations concerned with improving safety are using tools such as climate surveys to monitor the attitudes of staff to safety issues and identify areas for development. Patient complaints and feedback are also being looked at more carefully, and patients and families are being more formally involved in improvement work.")
7
Measuring & Understanding Culture is a good start!
Culture Assessment Tools Staff Surveys Patient and Carer Surveys Complaints / Compliments Incidents Successes!!!!

8
Patient Safety Culture Assessment Tools

9
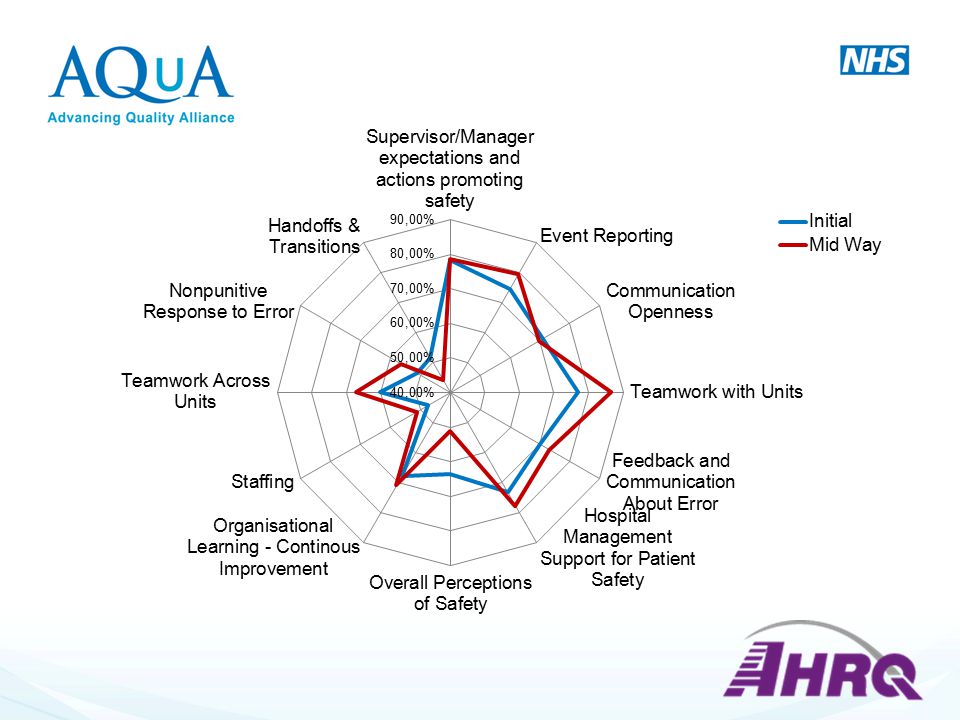
Patient Safety Culture Survey
AHRQ has established comparative databases as central repositories for survey data from organizations that have administered the AHRQ patient safety culture survey instruments. The databases serve as important resources for sites wishing to compare their patient safety culture survey results to those of other sites in support of patient safety culture improvement. The table below indicates the planned data submission time periods for the Surveys on Patient Safety Culture. Planned Surveys on Patient Safety Culture Data Submission Periods are done every 2 years in USA Hospital Survey on Patient Safety Culture & Medical Office Survey on Patient Safety Culture due 2015 Nursing Home Survey & Community Pharmacy Survey on Patient Safety Culture due 2016 As of October 2014, the number of international users that have administered the hospital survey now includes 59 countries, with 27 different translations. The nursing home survey has been administered in eight countries and translated into six languages. The medical office survey has been administered in 14 countries and translated into five languages. Lastly, the community pharmacy survey has been administered in five countries and translated into three languages. AHRQ survey there is increasing evidence available about the Validity and reliability of their dimensions. © 2014 AQuA

10
Background Health care organisations can use these survey assessment tools to: Raise staff awareness about patient safety. Diagnose and assess the current status of patient safety culture. Identify strengths and areas for patient safety culture improvement. Examine trends in patient safety culture change over time. Evaluate the cultural impact of patient safety initiatives and interventions. Conduct internal and external comparisons. © 2014 AQuA

11
Why use the tool? To support patient safety and quality improvement they sponsored the development of patient safety culture assessment tools. Bespoke AQuA member access (3 tools): Acute (Hospitals) Community Mental Health
: Acute (Hospitals) Community. Mental Health.")
12
Why use the tool? To support patient safety and quality improvement they sponsored the development of patient safety culture assessment tools. Bespoke AQuA member access (3 tools): Acute (Hospitals) Community Mental Health
: Acute (Hospitals) Community. Mental Health.")
13
© 2014 AQuA

17
Action Planning for Improvement
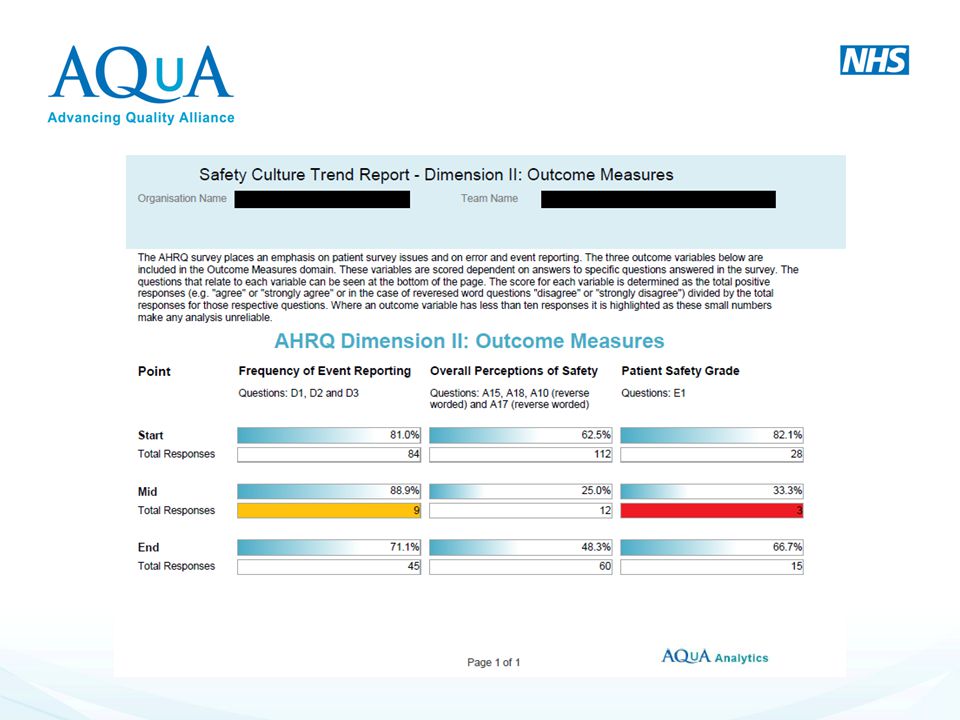
Understand your survey results. Communicate and discuss the survey results. Develop plans focused on actions. Communicate plans and clear deliverables. Implement action plans (remember what Jane Reid said about action plans!) Track progress and evaluate impact. Share what works. The delivery of survey results is not the end point in the survey process; it is just the beginning. Often, the perceived failure of surveys to create lasting change is actually due to faulty or nonexistent action planning or survey follow-up. Seven steps of action planning are provided to give hospitals guidance on next steps to take to turn their survey results into actual patient safety culture improvement:
 Track progress and evaluate impact. Share what works. The delivery of survey results is not the end point in the survey process; it is just the beginning. Often, the perceived failure of surveys to create lasting change is actually due to faulty or nonexistent action planning or survey follow-up. Seven steps of action planning are provided to give hospitals guidance on next steps to take to turn their survey results into actual patient safety culture improvement:")
18
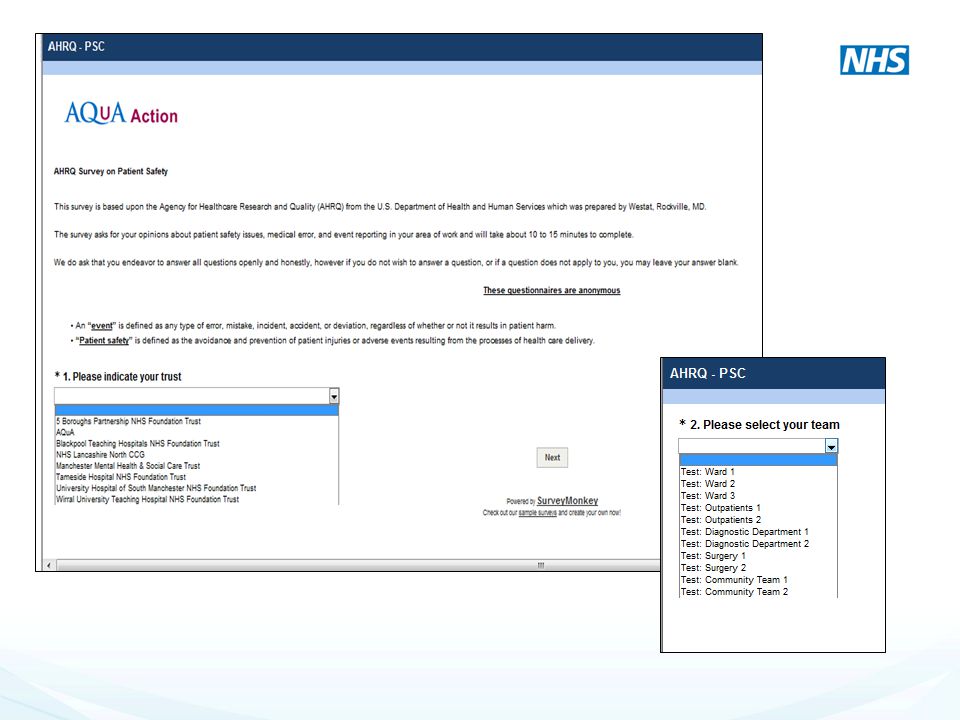
PSC AQuA AHRQ Demo

20
SECTION A: Your Department/Team

21
SECTION B: Your Supervisor/Manager

22
SECTION C: Communications

23
SECTION D: Frequency of Events Reported

24
SECTION E: Patient Safety Grade

25
SECTION F: Your Organisation

26
SECTION G: Number of Events Reported

27
SECTION H: Background Information

28
Appeared in: Reliability Engineering & System Safety 2012;101:21-34 A Novel Tool for Organisational Learning and its Impact on Safety Culture in a Hospital Dispensary Mark A. Sujan Warwick Medical School, University of Warwick Coventry, CV4 7AL, UK

29
Next Steps Think about your depts./teams to be involved
Agree “names” for the tool for AQuA & identification of each team Survey demonstration and test IT platform to show and allow organisation discussion of the tool Concerns, queries, staff safety and trust issues clarified Reports available (produced by AQuA) Interpretation and evaluation of reports Utilisation of reports
 Interpretation and evaluation of reports. Utilisation of reports.")
30
Top Tips Start small Clarify your purpose Choose carefully
Use holistically Don’t mandate Start small. There is no single ‘organisational culture’. Instead, choose a small team, unit or service to assess the safety culture, preferably testing the survey first to iron out any problems. Clarify your purpose. Do you want to target efforts on areas most in need of improvement, set a baseline for the impact of an intervention, or open up conversations about safety issues? Choose carefully. There any many different tools available, but no single tool is the ‘right one’ – understand their strengths and limitations, and ensure there is a dataset to benchmark yourself against. Use holistically. Used once and in isolation, survey tools are just a snapshot. But as part of a wider suite of tools and targeted measures, and used repeatedly (eg targeting higher risk periods, such as junior doctor rotations), they will be far more illuminating and impactful. Don’t mandate. Culture surveys can facilitate open discussions about risk and safety because staff are engaged in them, not because managers or regulators tell them to do it.
, they will be far more illuminating and impactful. Don’t mandate. Culture surveys can facilitate open discussions about risk and safety because staff are engaged in them, not because managers or regulators tell them to do it.")
31
Evaluation & Next Steps

32
To do list Please watch the DVD’s as these will help you in the further modules DVD’s to be returned on the last day – 22nd May 2015 Please liaise with Rose regarding your site visits (if not already done so) Sign in sheet!
 Sign in sheet!")
33
Any Questions. For more info about the tool: amanda. huddleston@srft
Any Questions? For more info about the tool:

Similar presentations
>")
>")


” for each unit where.>")














