Download presentation
Presentation is loading. Please wait.

2
Acute Poststreptococcal glomerulonephritis
A.R.Merrikhi.MD. PediatricNephrologist

3
INTRODUCTION Poststreptococcal glomerulonephritis (PSGN) is caused by prior infection with specific nephritogenic strains of group A beta-hemolytic streptococcus. The clinical presentation of PSGN varies from asymptomatic, microscopic hematuria to the full-blown acute nephritic syndrome, characterized by red to brown urine, proteinuria (which can reach the nephrotic range), edema, hypertension, and acute kidney injury. The prognosis is generally favorable, especially in children, but in some cases, the long-term prognosis is not benign.
 is caused by prior infection with specific nephritogenic strains of group A beta-hemolytic streptococcus. The clinical presentation of PSGN varies from asymptomatic, microscopic hematuria to the full-blown acute nephritic syndrome, characterized by red to brown urine, proteinuria (which can reach the nephrotic range), edema, hypertension, and acute kidney injury. The prognosis is generally favorable, especially in children, but in some cases, the long-term prognosis is not benign.")
4
Diffuse Intracapillary GN. Diffuse Endocapillary GN
*Diffuse Intracapillary GN *Diffuse Endocapillary GN *Acute Postinfection GN

5
EPIDEMIOLOGY Although PSGN continues to be the most common cause of acute nephritis globally, it primarily occurs in developing countries. Of the estimated 470,000 new annual cases of PSGN worldwide, 97 percent occur in developing countries, with an annual incidence that ranges from 9.5 to 28.5 per 100,000 individuals. In more developed and industrialized countries, the incidence has decreased over the past three decades.

6
EPIDEMIOLOGY Based upon data from the Italian Biopsy registry, the estimated annual incidence was 0.3 per 100,000 individuals between 1992 and 1994. The risk of PSGN is increased in older patients (greater than 60 years of age) and in children between 5 and 12 years of age. PSGN is uncommon in children less than three years of age. The incidence of clinically detectable PSGN in children infected during a GAS epidemic is about 5 to 10 percent with pharyngitis and 25 percent with skin infections.
 and in children between 5 and 12 years of age. PSGN is uncommon in children less than three years of age. The incidence of clinically detectable PSGN in children infected during a GAS epidemic is about 5 to 10 percent with pharyngitis and 25 percent with skin infections.")
7
Host factors Age: (2-12 years , 5%< 2 yrs) Sex: (M:F→2:1)
Socioeconomic background Genetic predisposition (HLA-DR1 & DRW4) (HLA –DRW48 & DRW8 less susceptible)
 (HLA –DRW48 & DRW8 less susceptible)")
8
PATHOGENESIS PSGN appears to be caused by glomerular immune complex disease induced by specific nephritogenic strains of group A beta-hemolytic streptococcus (GAS). The resulting glomerular immune complex disease triggers complement activation and inflammation.
. The resulting glomerular immune complex disease triggers complement activation and inflammation.")
9
Pathogenesis of APSGN Trapping of circulating immune Complexes in the glomeruli Molecular mimicry between streptococcal & renal antigen Insitu immune complex formation between antistreptococcal antibodies & glomerular planted Ags Direct complement activation by streptococcal Ags deposited in the glomeruli

10
PATHOGENESIS The mechanisms for the immunologic glomerular injury induced by GAS infection: Deposition of circulating immune complexes with streptococcal antigenic components In situ immune complex formation resulting from deposition of streptococcal antigens within the glomerular basement membrane (GBM) and subsequent antibody binding In situ glomerular immune complex formation promoted by antibodies to streptococcal antigens that cross-react with glomerular components (molecular mimicry) Alteration of a normal renal antigen that elicits autoimmune reactivity
 and subsequent antibody binding. In situ glomerular immune complex formation promoted by antibodies to streptococcal antigens that cross-react with glomerular components (molecular mimicry) Alteration of a normal renal antigen that elicits autoimmune reactivity.")
11
Nephritogenic Antigens
Endostreptosin → Early phase of APSGN Cationic Antigens → Later phase of the disease Streptococcal pyrogenic Exotoxin B (SpeB) Ab titers to SpeB are markedly elevated in APSGN (Acute rheumatic fever, scarlet fever or healthy subjects) SpeB→ 67% APSGN biopsy specimens Streptokinase Neuraminidase Nephritis – Associated plasmin Receptor (NAPlr)→ Early stage
 Ab titers to SpeB are markedly elevated in APSGN. (Acute rheumatic fever, scarlet fever or healthy subjects) SpeB→ 67% APSGN biopsy specimens. Streptokinase. Neuraminidase. Nephritis – Associated plasmin Receptor (NAPlr)→ Early stage.")
12
Nephritogenic Antigens
There are two leading candidates for the putative streptococcal antigen(s) responsible for PSGN: Nephritis-associated plasmin receptor (NAPlr), a glycolytic enzyme, which has glyceraldehyde-3- phosphate dehydrogenase (GAPDH) activity Streptococcal pyrogenic exotoxin B (SPE B), a cationic cysteine proteinase
 responsible for PSGN: Nephritis-associated plasmin receptor (NAPlr), a glycolytic enzyme, which has glyceraldehyde-3- phosphate dehydrogenase (GAPDH) activity. Streptococcal pyrogenic exotoxin B (SPE B), a cationic cysteine proteinase.")
13
Nephritogenic antigens
In a study of Japanese patients with PSGN, NAPlr was present in renal biopsy samples obtained within the first 14 days of their disease. Antibodies to NAPlr were present in the sera of 92 percent of patients with PSGN, and 60 percent of patients with uncomplicated group A streptococcal infections. In another report that included patients from Latin America and Switzerland, SPE B was found in 12 of 17 biopsies. SPE B deposition colocalized with complement deposition and within the subepithelial electron dense deposits (humps) that are characteristic of PSGN. Antibodies to SPE B were detected in the convalescent sera in all 53 patients who were tested. In contrast, circulating antibodies to NAPlr were found in only 5 of 47 tested sera, and in only one biopsy sample.
 that are characteristic of PSGN. Antibodies to SPE B were detected in the convalescent sera in all 53 patients who were tested. In contrast, circulating antibodies to NAPlr were found in only 5 of 47 tested sera, and in only one biopsy sample.")
14
PATHOLOGY Light microscopy
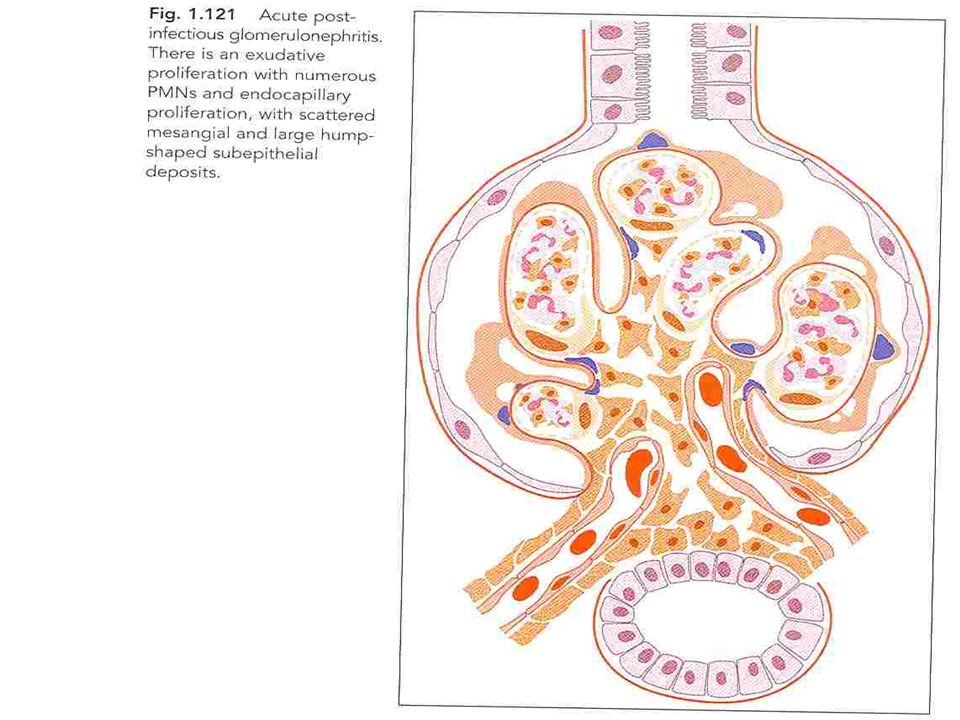
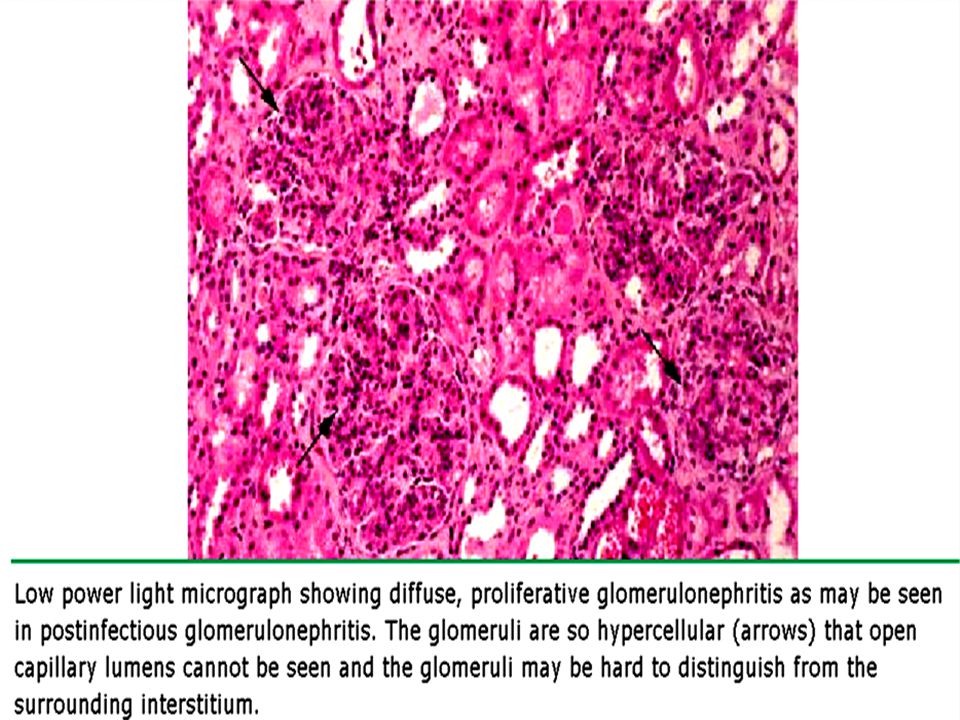
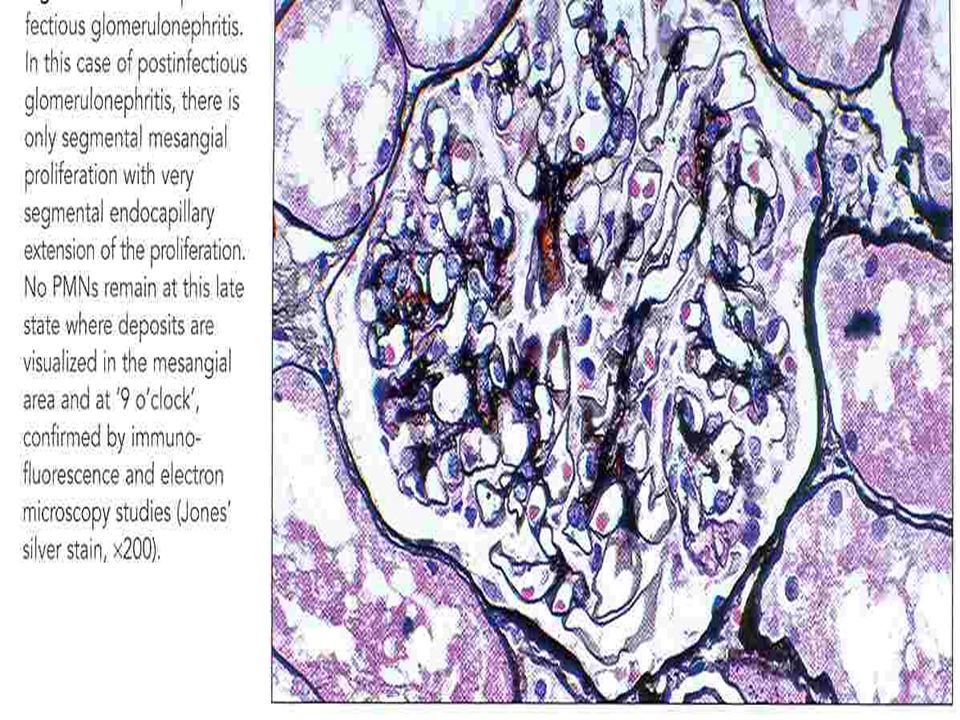
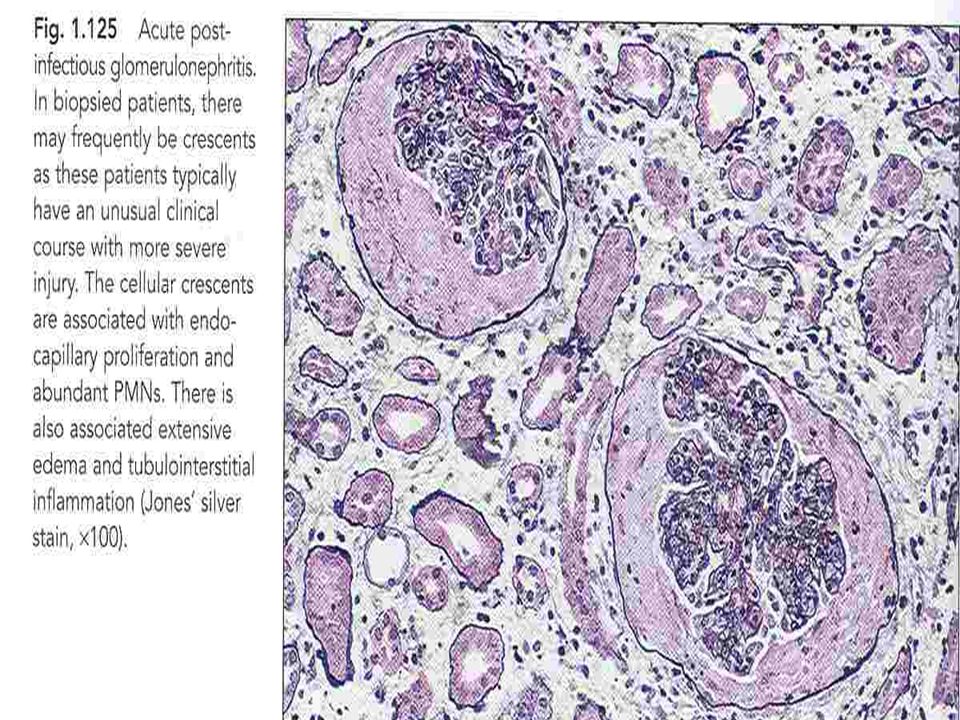
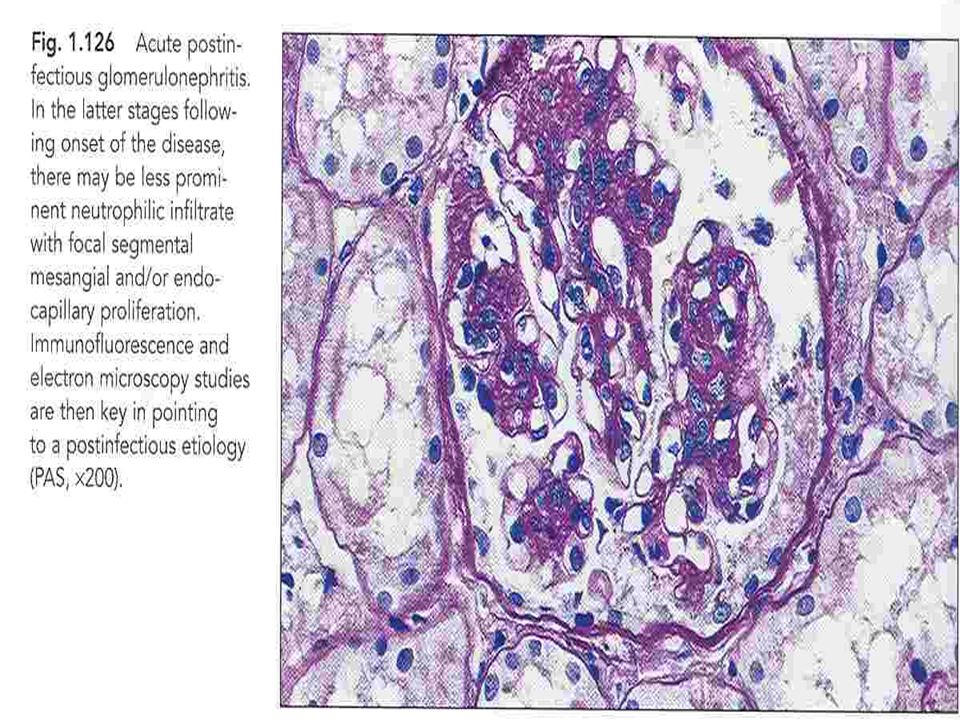
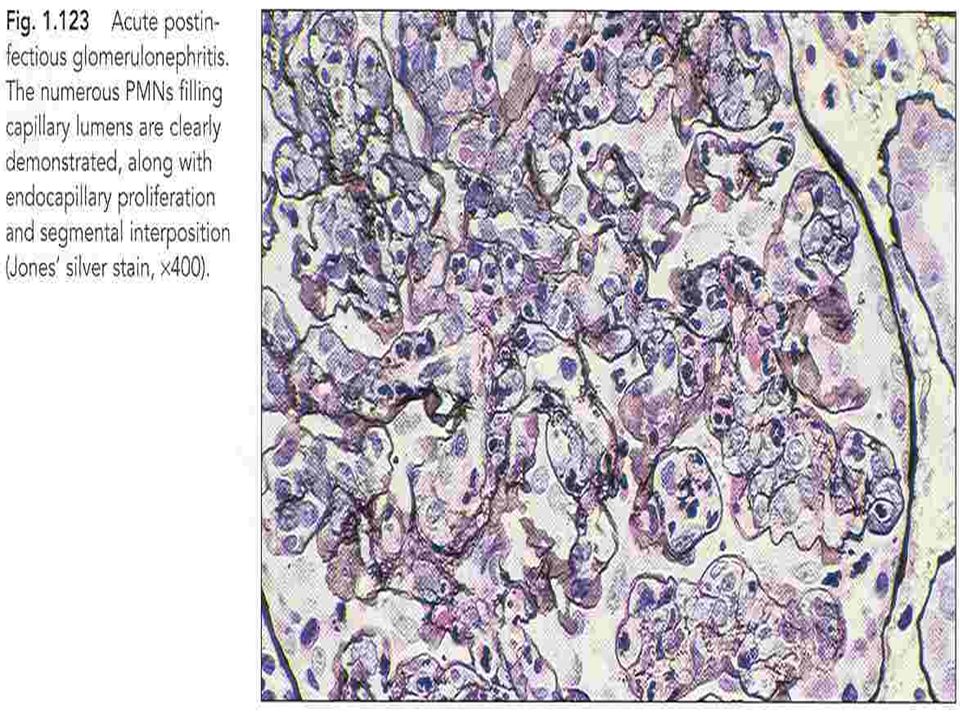
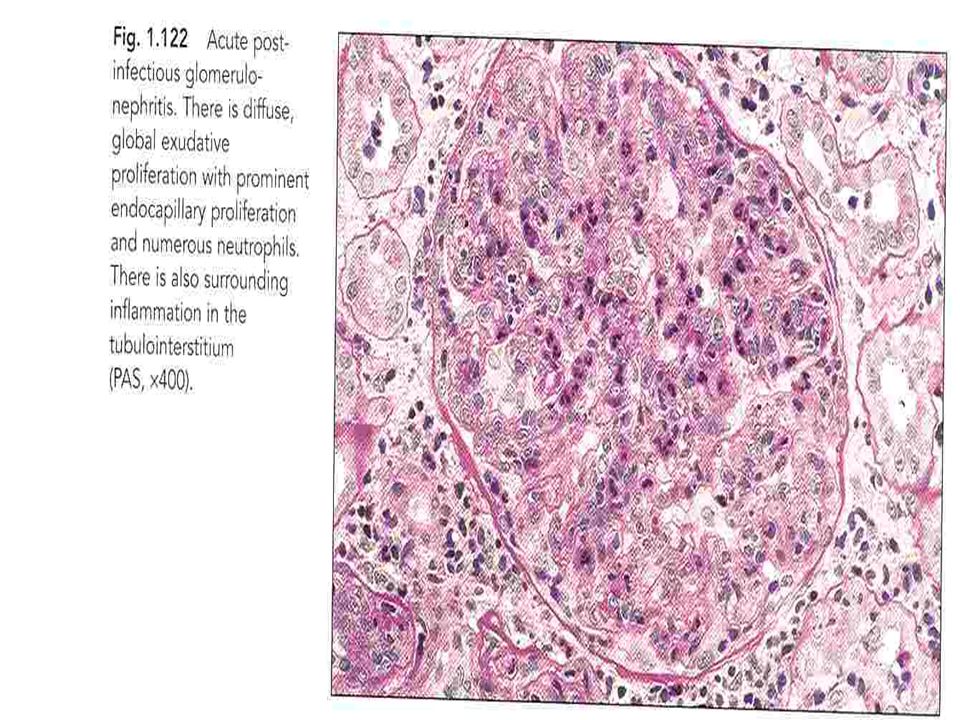
Light microscopy shows a diffuse proliferative glomerulonephritis with prominent endocapillary proliferation and numerous neutrophils. Trichrome stain may show small subepithelial hump- shaped deposits. The severity of involvement varies and usually correlates with the clinical findings. Crescent formation is uncommon and is associated with a poor prognosis.

15
Pathologic changes Light microscopic findings
Early stage → glomerular hypercellularity Later stage → Proliferation of intrinsic endothelial & mesangial cells

24
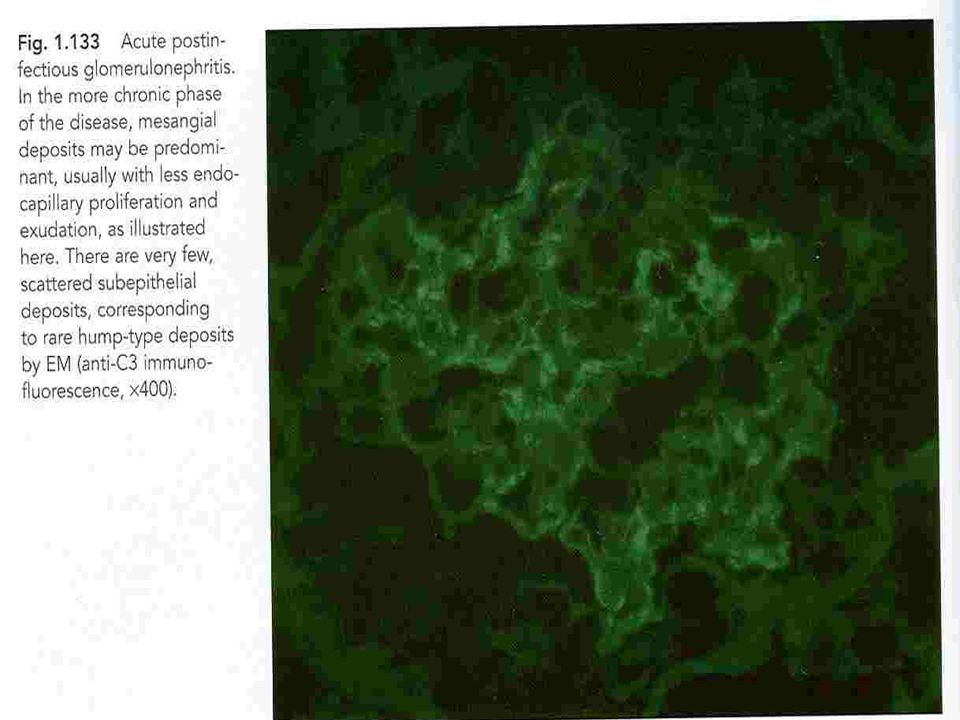
PATHOLOGY Immunofluorescence microscopy
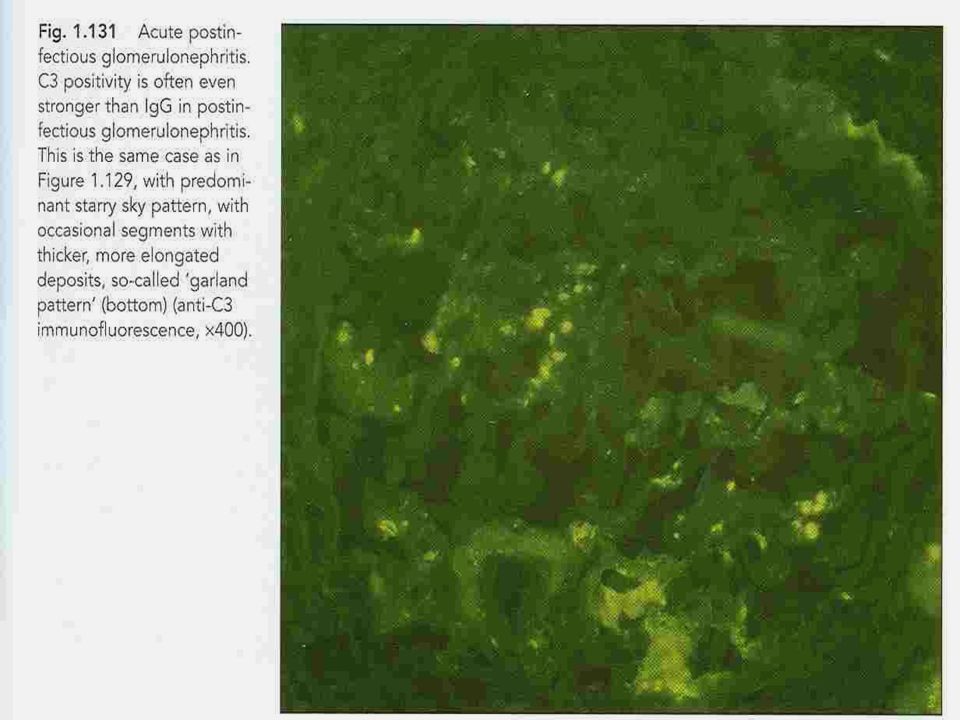
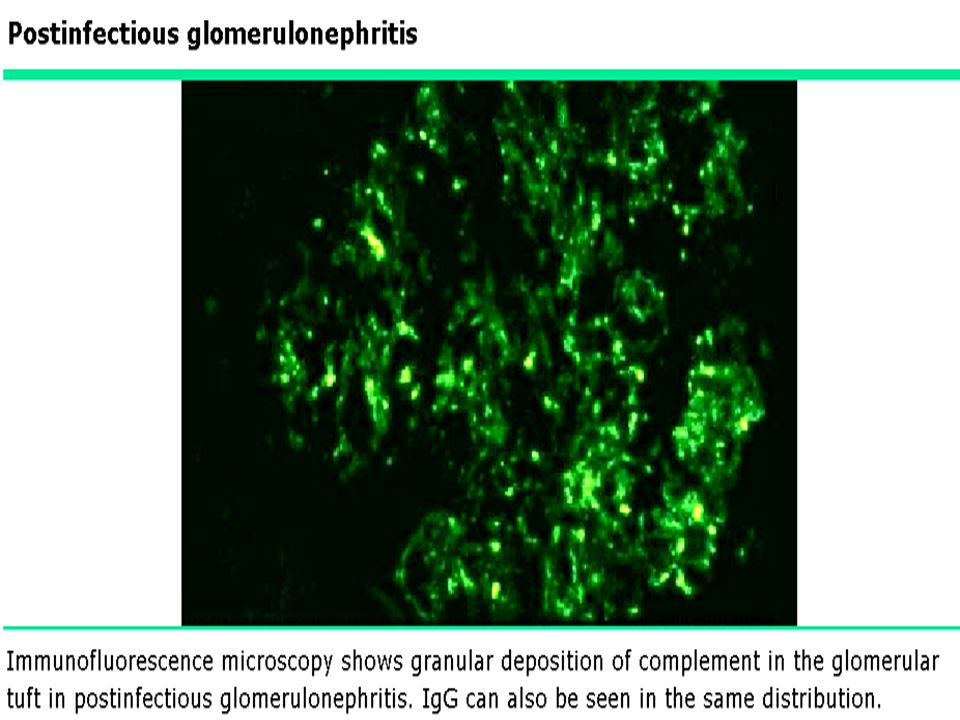
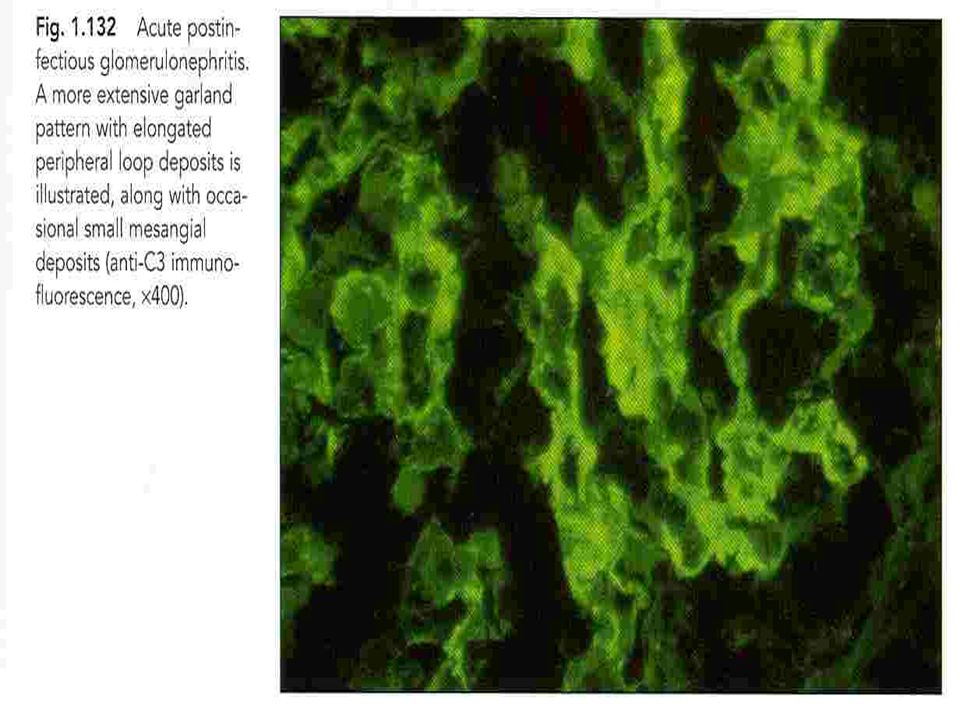
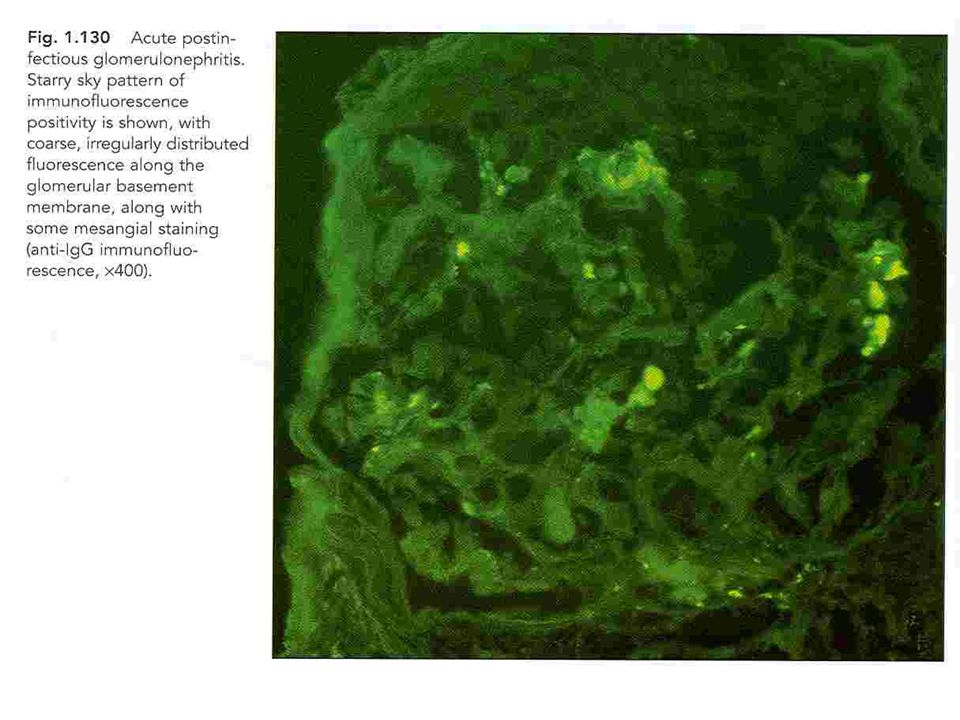
Immunofluorescence (IF) microscopy reveals a characteristic pattern of deposits of immunoglobulin (IgG) and C3 distributed in a diffuse granular pattern within the mesangium, and glomerular capillary walls. Other immune reactants (eg, IgM, IgA, fibrin, and other complement components) may also be detected.
 microscopy reveals a characteristic pattern of deposits of immunoglobulin (IgG) and C3 distributed in a diffuse granular pattern within the mesangium, and glomerular capillary walls. Other immune reactants (eg, IgM, IgA, fibrin, and other complement components) may also be detected.")
25
IF microscopy Coarse granular staining for IgG & C3 can be detected in GCW IgM→ less frequently IgA & C1 & C4 → absent Garland , starry sky & mesangial patterns

31
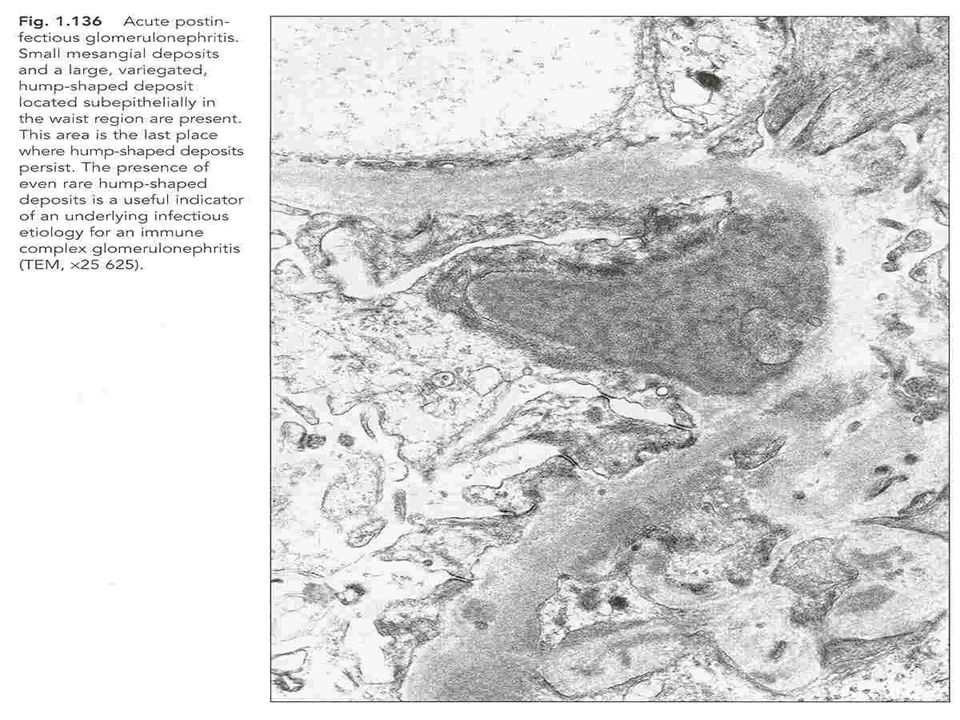
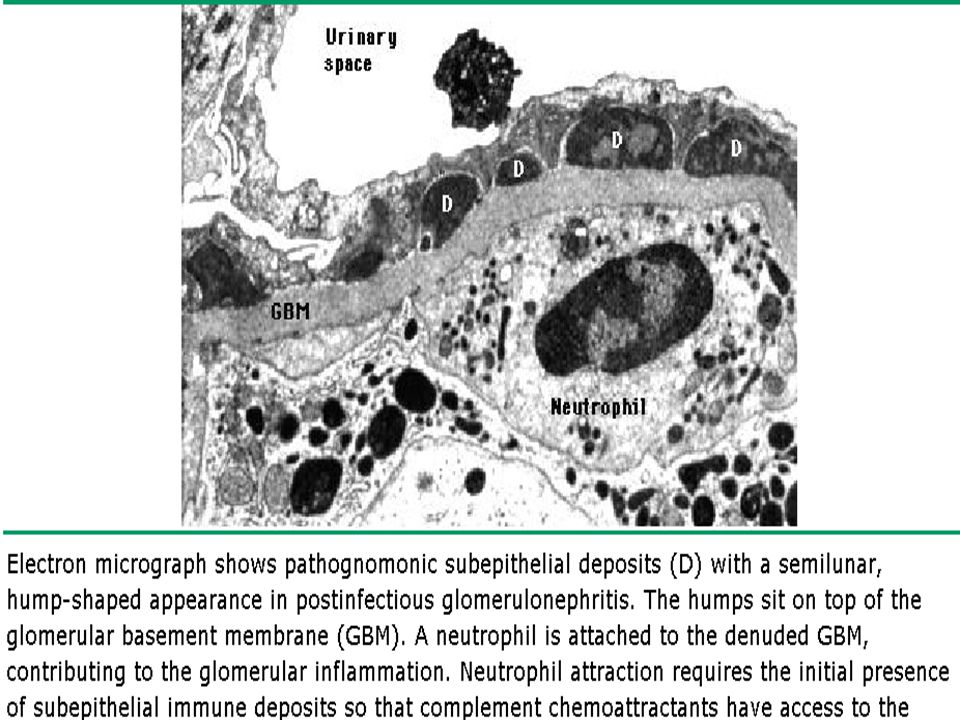
PATHOLOGY Electron microscopy
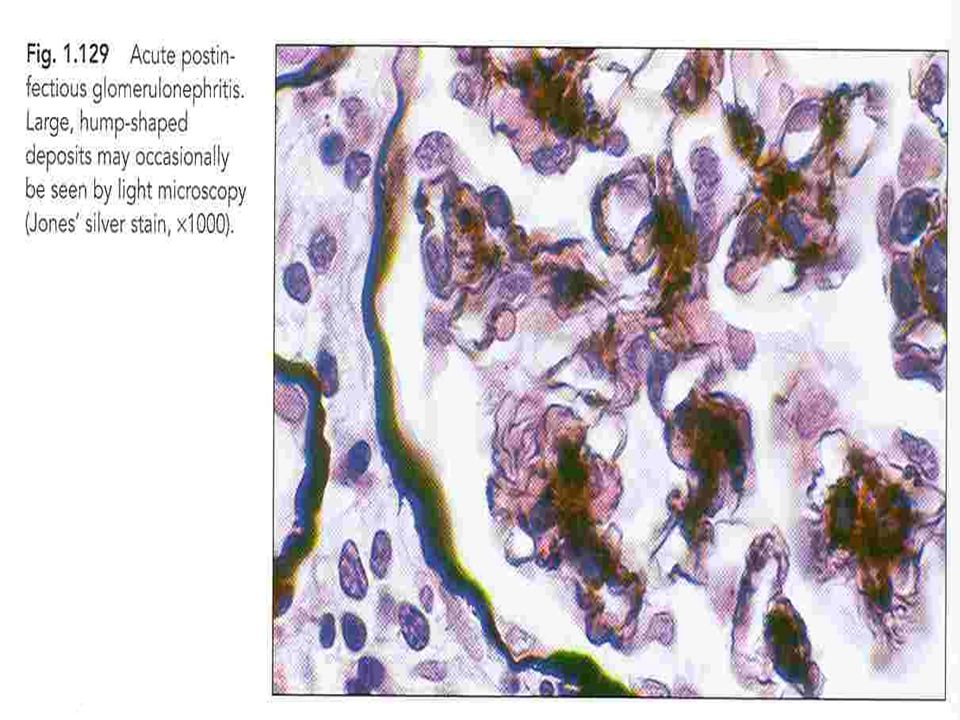
The dome-shaped subepithelial electron-dense deposits that are referred to as humps. Subendothelial immune deposits and subsequent complement activation are responsible for the local influx of inflammatory cells, leading to a proliferative glomerulonephritis, an active urine sediment, and a variable decline in glomerular filtration rate. Subepithelial "humps" are responsible for epithelial cell damage and proteinuria, similar to that seen in membranous nephropathy

32
Electron microscopy Swelling of glomerular endothelial & mesangial cells Humps (disappear 6 wks after the clinicalonset of dx)
 .")
35
CLINICAL MANIFESTATIONS
The clinical presentation varies from asymptomatic, microscopic hematuria to the full-blown acute nephritic syndrome, characterized by red to brown urine, proteinuria (which can reach the nephrotic range), edema, hypertension, and an elevation in serum creatinine. There is usually an antecedent history of a group A beta- hemolytic streptococcal (GAS) skin or throat infection. The latent period between GAS infection and PSGN is dependent upon the site of infection: between one and three weeks following GAS pharyngitis and between three and six weeks following GAS skin infection.
, edema, hypertension, and an elevation in serum creatinine. There is usually an antecedent history of a group A beta- hemolytic streptococcal (GAS) skin or throat infection. The latent period between GAS infection and PSGN is dependent upon the site of infection: between one and three weeks following GAS pharyngitis and between three and six weeks following GAS skin infection.")
36
CLINICAL MANIFESTATIONS
The most common presenting signs in children: Edema — Generalized edema is present in about two-thirds of patients due to sodium and water retention. In severe cases, fluid overload leads to respiratory distress due to pulmonary edema. Gross hematuria — Gross hematuria is present in about 30 to 50 percent of patients. The urine looks smoky, and tea or coca cola- colored. Hypertension — Hypertension is present in 50 to 90 percent of patients and varies from mild to severe. It is primarily caused by fluid retention. Hypertensive encephalopathy was an uncommon but serious complication. Subclinical cases of PSGN are primarily characterized by microscopic hematuria .

37
Clinical presentation
Abrupt onset of hemutaria (100%) Proteinuria (80%) Edema (90%) HTN (60-80%) Mild to moderate renal insufficiency (25-40%) Latent period → (1-2 wks, throat infection , 3-6 wks skin infection) Subclinical to clinically overt dx → 4-5:1
 Proteinuria (80%) Edema (90%) HTN (60-80%) Mild to moderate renal insufficiency (25-40%) Latent period → (1-2 wks, throat infection , 3-6 wks skin infection) Subclinical to clinically overt dx → 4-5:1.")
38
Clinical presentation
Gross hematuria (24-40%) (2wks) Urine: smoky or coke – colored Dysuria , frequency & abdominal discomfort Transient oliguria (50%) , anuria (rare) Edema CHF
 (2wks) Urine: smoky or coke – colored. Dysuria , frequency & abdominal discomfort. Transient oliguria (50%) , anuria (rare) Edema. CHF.")
39
Clinical presentation
Hypertension Volume dependent ↑ peripheral vascular resistance Hypertensive emergency Hypertensive urgency Nausea/ vomiting /malaise/ anorexia/ lumbarpain/ weakness

40
Laboratory findings Urinalysis
The urinalysis in patients with PSGN reveal hematuria (some of the red cells are typically dysmorphic) with or without red blood cell casts, varying degrees of proteinuria and often pyuria. Nephrotic range proteinuria is uncommon and occurs in about 5 percent of cases at presentation.
 with or without red blood cell casts, varying degrees of proteinuria and often pyuria. Nephrotic range proteinuria is uncommon and occurs in about 5 percent of cases at presentation.")
41
Laboratory findings Complement
In about 90 percent of patients, C3 and CH50 (total complement activity) are significantly depressed in the first two weeks of the disease course. In comparison, C4 and C2 levels are usually normal or only mildly decreased. The C3 and CH 50 return to normal within four to eight weeks after presentation. The combination of a low C3 level and a normal or only slightly decreased C4 level indicates activation of the alternative pathway of complement.
 are significantly depressed in the first two weeks of the disease course. In comparison, C4 and C2 levels are usually normal or only mildly decreased. The C3 and CH 50 return to normal within four to eight weeks after presentation. The combination of a low C3 level and a normal or only slightly decreased C4 level indicates activation of the alternative pathway of complement.")
42
Laboratory findings Culture
Because PSGN presents weeks after an antecedent GAS infection, only about 25 percent of patients will have either a positive throat or skin culture. In patients with impetigo, there is an increased likelihood of obtaining a positive skin culture.

43
Laboratory findings Serology
The streptozyme test, which measures five different streptococcal antibodies, is positive in more than 95 percent of patients with PSGN due to pharyngitis and about 80 percent of those with skin infections. It includes the following antibodies: Anti-streptolysin (ASO) Anti-hyaluronidase (AHase) Anti-streptokinase (ASKase) Anti-nicotinamide-adenine dinucleotidase (anti-NAD) Anti-DNAse B antibodies
 Anti-hyaluronidase (AHase) Anti-streptokinase (ASKase) Anti-nicotinamide-adenine dinucleotidase (anti-NAD) Anti-DNAse B antibodies.")
44
Serology After a pharyngeal infection, the ASO, anti-DNAse B, anti-NAD, and AHase titers are commonly elevated. In comparison, only the anti-DNAse B and AHase titers are typically increased after a skin infection. If only the ASO titer is used to screen for GAS infection, it may be falsely low or negative in patients with skin infections.

45
DIAGNOSIS PSGN is usually diagnosed based upon clinical findings of acute nephritis and demonstration of a recent group A beta- hemolytic streptococcal (GAS) infection. The clinical findings of acute nephritis include hematuria with or without red blood cell casts, variable degrees of proteinuria, edema, and hypertension. Documentation of a recent GAS infection includes either a positive throat or skin culture or serologic tests (eg, ASO or streptozyme test).
 infection. The clinical findings of acute nephritis include hematuria with or without red blood cell casts, variable degrees of proteinuria, edema, and hypertension. Documentation of a recent GAS infection includes either a positive throat or skin culture or serologic tests (eg, ASO or streptozyme test).")
46
DIAGNOSIS Although a low C3 and/or CH 50 (total complement) level are consistent with a diagnosis of PSGN, these complement components may also be decreased in other forms of glomerulonephritis, including membranoproliferative glomerulonephritis. A delay in the diagnosis of PSGN is more common in children who do not have a history of an antecedent GAS infection and have microscopic hematuria. In most of the patients, presenting findings were due to volume overload and included hypertension, edema, and pulmonary edema.
 level are consistent with a diagnosis of PSGN, these complement components may also be decreased in other forms of glomerulonephritis, including membranoproliferative glomerulonephritis. A delay in the diagnosis of PSGN is more common in children who do not have a history of an antecedent GAS infection and have microscopic hematuria. In most of the patients, presenting findings were due to volume overload and included hypertension, edema, and pulmonary edema.")
47
Diagnostic Evaluation
U/A: dysmorphic or crenated RBCs & RBC casts Proteinuria (5-10% nephrotic range) WBC, hyaline & granular casts ↑ BUN , Cr ↑ ASO , Anti- NADase (80% postpharyngitis nephritis) Antihyaluronidase & Anti- DNase B (80-90%) skin infections) ↑ Antibody titers → 1-5 wks after infections C3, C4 , CH50 ↓C3 , CH50(90%) ANCA (9%)
 WBC, hyaline & granular casts. ↑ BUN , Cr. ↑ ASO , Anti- NADase (80% postpharyngitis nephritis) Antihyaluronidase & Anti- DNase B (80-90%) skin infections) ↑ Antibody titers → 1-5 wks after infections. C3, C4 , CH50. ↓C3 , CH50(90%) ANCA (9%)")
48
Renal biopsy A biopsy is usually performed in patients in whom other glomerular disorders are being considered because they deviate from the natural course of the PSGN or they present late without a clear history of prior streptococcal infection. Persistently low C3 levels beyond six weeks are suggestive of a diagnosis of membranoproliferative glomerulonephritis. Recurrent episodes of hematuria are suggestive of IgA nephropathy and are rare in PSGN. A progressive increase in serum creatinine is uncharacteristic of PSGN, but there are occasional patients who do not recover from the acute episode.

49
Indications of kidney Biopsy
Nephrotic – range proteinuria in the acute stage Nl serum complement Progressively increasing serum Cr Prolonged hypocomplementemia for more than 3 mo Ongoing macroscopic hematuria Long standing proteinuria

50
DIFFERENTIAL DIAGNOSIS
Membranoproliferative glomerulonephritis (MPGN) IgA nephropathy Secondary causes of glomerulonephritis — Lupus nephritis and Henoch-Schönlein purpura nephritis share similar features to PSGN. Both hepatitis B and endocarditis-associated glomerulonephritis share common features with PSGN and also will present with reductions in C3 and C4. Postinfectious GN due to other microbial agents
 IgA nephropathy. Secondary causes of glomerulonephritis — Lupus nephritis and Henoch-Schönlein purpura nephritis share similar features to PSGN. Both hepatitis B and endocarditis-associated glomerulonephritis share common features with PSGN and also will present with reductions in C3 and C4. Postinfectious GN due to other microbial agents.")
51
MANAGEMENT The patients with more than 30 percent crescents on renal biopsy are often treated with methylprednisolone pulses. Management is supportive and is focused on treating the clinical manifestations of the disease, particularly complications due to volume overload. These include hypertension and, less commonly, pulmonary edema. General measures include sodium and water restriction and loop diuretics.

52
MANAGEMENT Loop diuretics generally provide a prompt diuresis with reduction of blood pressure and edema. In our practice, intravenous furosemide is given at an initial dose of 1 mg/kg (maximum 40 mg). Patients with PSGN have variable reductions in renal function, and some patients require dialysis during the acute episode. Patients with evidence of persistent group A streptococcal infection should be given a course of antibiotic therapy.
. Patients with PSGN have variable reductions in renal function, and some patients require dialysis during the acute episode. Patients with evidence of persistent group A streptococcal infection should be given a course of antibiotic therapy.")
53
COURSE Resolution of the clinical manifestations of PSGN is generally quite rapid, assuming concurrent resolution of the infection. A diuresis typically begins within one week, and the serum creatinine returns to the previous baseline by three to four weeks. The urinary abnormalities disappear at differing rates. Hematuria usually resolves within three to six months. Proteinuria also falls during recovery, but at a much slower rate. A mild increase in protein excretion is still present in 15 percent at 3 years, and 2 percent at 7 to 10 years. In severe cases with nephrotic range proteinuria, this degree of proteinuria may persist for six months or more, long after the hematuria has disappeared.

54
Recurrence Recurrent episodes of PSGN are rare.
This may be due to the long-term persistence of antibodies to nephritis-associated streptococcal antigen.

55
PROGNOSIS Most patients, particularly children, have an excellent outcome. This is true even in patients who present with acute renal failure and may have crescents on the initial renal biopsy. A review of three case series of 229 children with PSGN found that approximately 20 percent had an abnormal urinalysis (proteinuria and/or hematuria), but almost all (92 to 99 percent) had normal or only modestly reduced renal function 5 to 18 years after presentation. However, the long-term prognosis of PSGN is not always benign.
, but almost all (92 to 99 percent) had normal or only modestly reduced renal function 5 to 18 years after presentation. However, the long-term prognosis of PSGN is not always benign.")
56
PROGNOSIS Some patients, particularly adults, develop hypertension, recurrent proteinuria (with a relatively normal urine sediment), and renal insufficiency as long as 10 to 40 years after the initial illness. These late renal complications are associated with glomerulosclerosis on renal biopsy, which is thought to be hemodynamically-mediated. According to this hypothesis, some glomeruli are irreversibly damaged during the acute episode and compensatory hyperfiltration in the remaining glomeruli maintains a relatively normal glomerular filtration rate.
, and renal insufficiency as long as 10 to 40 years after the initial illness. These late renal complications are associated with glomerulosclerosis on renal biopsy, which is thought to be hemodynamically-mediated. According to this hypothesis, some glomeruli are irreversibly damaged during the acute episode and compensatory hyperfiltration in the remaining glomeruli maintains a relatively normal glomerular filtration rate.")
57
Prognosis & clinical outcome
Early mortality rate:<1% Complete remission Hypertension & gross hematuria → several weeks Proteinuria → several months Microscopic hematuria → persist for years ESRD → % (NAplr protein) ESRD →2% Recurrence APSGN → %(NAplr protein)
 ESRD →2% Recurrence APSGN → %(NAplr protein)")
58
WITH THANKS

Similar presentations











 RENAL DISEASE: OVERVIEW AND ACUTE RENAL FAILURE Pathophysiology of Disease: Chapter 16 (388-394) Jack.>")







 is the sudden onset of: – Haematuria (macroscopic/microscopic)>")
SC>")