Download presentation
Presentation is loading. Please wait.

1
Preventing Operating Room Disasters Before They Happen Rafael Ortega, MD Associate Professor of Anesthesiology Rafael Ortega, MD Associate Professor of Anesthesiology Joint Anesthesia / Nursing Lecture Risk Management Activity Joint Anesthesia / Nursing Lecture Risk Management Activity Boston University School of Medicine February 26, 2007 Boston University School of Medicine February 26, 2007 7:00-8:00am

2
Objectives To review conditions O.R. disasters have in common To recommend strategies to minimize O.R. mishaps To present examples of O.R. disasters (or near disasters) To review conditions O.R. disasters have in common To recommend strategies to minimize O.R. mishaps To present examples of O.R. disasters (or near disasters)
 To review conditions O.R. disasters have in common To recommend strategies to minimize O.R. mishaps To present examples of O.R. disasters (or near disasters).")
3
Anesthesia Risk The rates of morbidity and mortality depend on the definitions. Data demonstrates that risk directly attributable to anesthesia has declined over time. The rates of morbidity and mortality depend on the definitions. Data demonstrates that risk directly attributable to anesthesia has declined over time.

4
Liquid Oxygen Leak Birmingham, Alabama VA Hospital Schumacher SD et al. Bulk Liquid Oxygen Supply Failure. Anesthesiology. 2004;100:186-189. Birmingham, Alabama VA Hospital Schumacher SD et al. Bulk Liquid Oxygen Supply Failure. Anesthesiology. 2004;100:186-189.

5
Recognition, management, and prevention of specific operating room catastrophes Presented at the American College of Surgeons 89th Annual Clinical Congress, Chicago, IL, October 2003. Christopher R. McHenry MD, Ramon Berguer MD, FACS, Rafael A. Ortega MD Journal of the American College of Surgeons Volume 198, Issue 5, May 2004, Pages 810-821 Recognition, management, and prevention of specific operating room catastrophes Presented at the American College of Surgeons 89th Annual Clinical Congress, Chicago, IL, October 2003. Christopher R. McHenry MD, Ramon Berguer MD, FACS, Rafael A. Ortega MD Journal of the American College of Surgeons Volume 198, Issue 5, May 2004, Pages 810-821 It’s Everyone’s Business!

6
Potential Crises Anaphylaxis Transfusion Reactions Malignant Hyperthermia Difficult Airway Fires Electrical Safety Cardiac Arrest Etc. Anaphylaxis Transfusion Reactions Malignant Hyperthermia Difficult Airway Fires Electrical Safety Cardiac Arrest Etc. But what do they have in common?

7
Features in Common Critical incidents Reason’s Swiss Cheese Relatively Rare Training (and re-training) Required Fixation Errors Reportable Litigation Prone More….. Critical incidents Reason’s Swiss Cheese Relatively Rare Training (and re-training) Required Fixation Errors Reportable Litigation Prone More…..
 Required Fixation Errors Reportable Litigation Prone More…...")
8
Normal MP l Small jaw MP ll Small jaw Short neck MP lll Small jaw Short neck Obese Goiter MP lV …more preparation needed… history / physical exam / medical record / anesthesia record / lab work / consults / etc.

9
wasterisk match Complexity Preparedness

10
Complexity

11
Preparedness

12
Organizational Influences Organizational Influences Unsafe Supervision Unsafe Supervision Precondition for Unsafe Acts Precondition for Unsafe Acts Unsafe Acts Unsafe Acts Successive Layers of Defenses Based on: Reason, J. (1990) Human Error. Cambridge: University Press, Cambridge
 Human Error. Cambridge: University Press, Cambridge.")
13
Failed or Absent Defenses Failed or Absent Defenses Aligned Holes Example: wrong site / wrong patient Aligned Holes Example: wrong site / wrong patient Based on: Reason, J. (1990) Human Error. Cambridge: University Press, Cambridge
 Human Error. Cambridge: University Press, Cambridge.")
14
System Failure Based on: Reason, J. (1990) Human Error. Cambridge: University Press, Cambridge
 Human Error. Cambridge: University Press, Cambridge")
15
What is a “Critical Incident”? Term made famous by Cooper. Defined: occurrences that are “significant or pivotal, in causing undesirable consequences. Also defined as: an event that led, or could have led to a problem. Critical Incidents provide opportunity to learn about factors that can be remedied. Term made famous by Cooper. Defined: occurrences that are “significant or pivotal, in causing undesirable consequences. Also defined as: an event that led, or could have led to a problem. Critical Incidents provide opportunity to learn about factors that can be remedied. Preventable anesthesia mishaps: a study of human factors. Anesthesiology. 1978 Dec;49(6):399-406.
:")
16
What is the Role of Simulation? Howard SK, Gaba DM, Fish KJ, Yang G, Sarnquist FH. Anesthesia crisis resource management training: teaching anesthesiologists to handle critical incidents. Aviat Space Environ Med 1992: 63: 763-770 Holzman RS et al:. Anesthesia crisis resource management: real-life simulation training in operating room crises. Journal of Clinical Anesthesia. 7(8):675-87, 1995: >50% felt it should be taken once every 12 months Ziv A et al: Simulation based medical education: an opportunity to learn from errors. Medical Teacher. 27(3):193-9, 2005 May. Berkenstadt H et al: The feasibility of sharing simulation-based evaluation scenarios in anesthesiology. Anesthesia & Analgesia. 101(4):1068-74, 2005 Oct. Ziv A et al: Simulation-Based medical education: an ethical imperative. Academic Medicine. 78(8):783-788, 2003. Howard SK, Gaba DM, Fish KJ, Yang G, Sarnquist FH. Anesthesia crisis resource management training: teaching anesthesiologists to handle critical incidents. Aviat Space Environ Med 1992: 63: 763-770 Holzman RS et al:. Anesthesia crisis resource management: real-life simulation training in operating room crises. Journal of Clinical Anesthesia. 7(8):675-87, 1995: >50% felt it should be taken once every 12 months Ziv A et al: Simulation based medical education: an opportunity to learn from errors. Medical Teacher. 27(3):193-9, 2005 May. Berkenstadt H et al: The feasibility of sharing simulation-based evaluation scenarios in anesthesiology. Anesthesia & Analgesia. 101(4):1068-74, 2005 Oct. Ziv A et al: Simulation-Based medical education: an ethical imperative. Academic Medicine. 78(8):783-788, 2003.
:675-87, 1995: >50% felt it should be taken once every 12 months Ziv A et al: Simulation based medical education: an opportunity to learn from errors. Medical Teacher. 27(3):193-9, 2005 May. Berkenstadt H et al: The feasibility of sharing simulation-based evaluation scenarios in anesthesiology. Anesthesia & Analgesia. 101(4): , 2005 Oct. Ziv A et al: Simulation-Based medical education: an ethical imperative. Academic Medicine. 78(8): , Howard SK, Gaba DM, Fish KJ, Yang G, Sarnquist FH. Anesthesia crisis resource management training: teaching anesthesiologists to handle critical incidents. Aviat Space Environ Med 1992: 63: Holzman RS et al:. Anesthesia crisis resource management: real-life simulation training in operating room crises. Journal of Clinical Anesthesia. 7(8):675-87, 1995: >50% felt it should be taken once every 12 months Ziv A et al: Simulation based medical education: an opportunity to learn from errors. Medical Teacher. 27(3):193-9, 2005 May. Berkenstadt H et al: The feasibility of sharing simulation-based evaluation scenarios in anesthesiology. Anesthesia & Analgesia. 101(4): , 2005 Oct. Ziv A et al: Simulation-Based medical education: an ethical imperative. Academic Medicine. 78(8): ,")
17
21 September 2005. JetBlue Flight 292 What is the Role of Simulation?

18
Simulation at BMC - Anesthesia

19
Illustrative Examples Wrong Dose: Communication Error Airway Management – Fixation Error Wrong Gas Administration Anaphylaxis Malignant Hyperthermia Fires Wrong Dose: Communication Error Airway Management – Fixation Error Wrong Gas Administration Anaphylaxis Malignant Hyperthermia Fires

20
“eight thousand of heparin” vs. “a thousand of heparin” “eight thousand of heparin” vs. “a thousand of heparin” Communication Error

21
Standard practice in the military, esp. in the Navy, is to use “voice procedure” to maximize clarity of spoken communication and reduce misunderstanding. Control Room aboard USS Seawolf submarine. (courtesy of www.navy.mil) Communication Error

22
Why Communication Fails in the Operating Room J Firth-Cozens Qual Saf Health Care 2004;13:327 Team instability - different scrub nurses Team policies about communication - proper introductions Disallowing distractions - noise Redundancy - allows people time to communicate Team meetings outside immediate task - enhancing rapport Sufficient resources - equipment Stress – what stress? Introverts Vs. Extroverts – many examples Groups with traditionally different status – surgeons Professional language - way of maintaining power? Team instability - different scrub nurses Team policies about communication - proper introductions Disallowing distractions - noise Redundancy - allows people time to communicate Team meetings outside immediate task - enhancing rapport Sufficient resources - equipment Stress – what stress? Introverts Vs. Extroverts – many examples Groups with traditionally different status – surgeons Professional language - way of maintaining power?

23
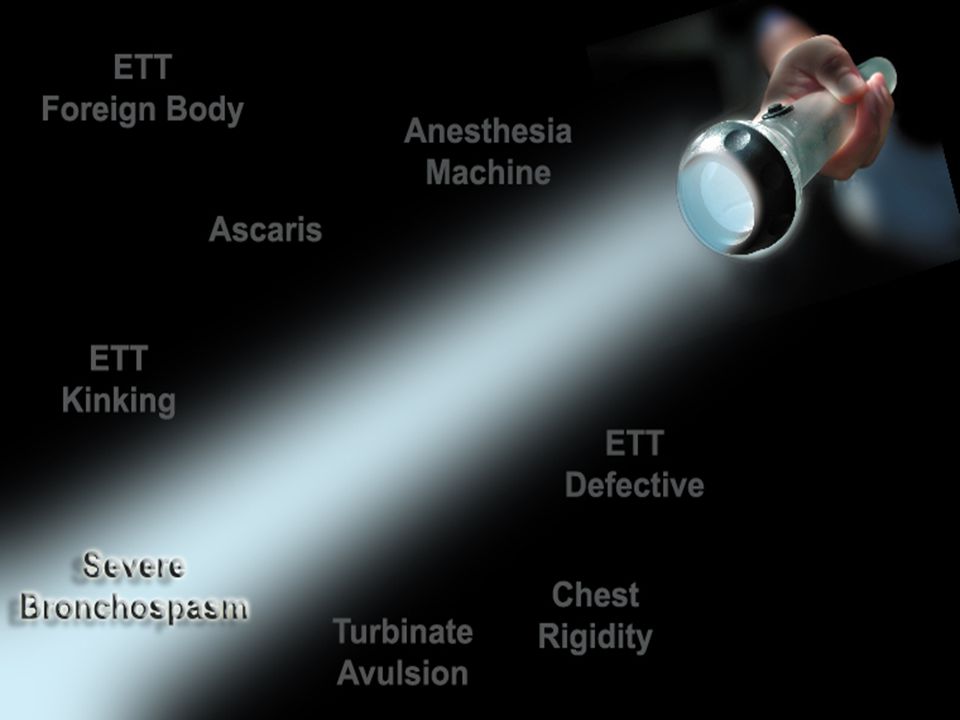
Losing the Airway 27-years-old male patient Fracture jaw Naso-tracheal intubation Class I visualization Difficult ventilation Equivocal capnogram Severe bronchospasm? 27-years-old male patient Fracture jaw Naso-tracheal intubation Class I visualization Difficult ventilation Equivocal capnogram Severe bronchospasm?

26
Fixation Errors Human errors (1/3 of error: FIXATION) Human errors (1/3 of error: FIXATION) DeAnda A, Gaba DM. Unplanned incidents during comprehensive anesthesia simulation. Anesth Analg. 1990 Jul;71(1):77-82. Equipment failures >
: Equipment failures >.")
27
Fixation Errors Types and Countermeasures "This and only this!" Persistent failure to revise a diagnosis Accept possibility that first assumptions may be wrong "Everything but this!" failure to commit to definitive treatment of major problem Rule out worst case scenario "Everything is OK!" Persistent belief that no problem is occurring Artifacts are the last explanation for changes in critical values CountermeasureError TypeDescription (Adapted from Rall M, Gaba DM: Human Performance and Patient Safety, in Miller 6th edition 2005)
")
28
Circular No. 60-22. Federal Aviation Administration Washington, DC

29
ANTI-AUTHORITY "Don't tell me what to do. The policies are for someone else." Follow the rules. They are usually right IMPULSIVITY "Do something quickly-anything!" Not so fast. Think first. INVULNERABILITY "It won't happen to me. It's just a routine case." “It could happen to me. Routine cases develop problems." MACHO "I'll show you I can do it. I intubate anyone’s trachea." Taking chances is foolish. Plan for failure RESIGNATION "What's the use? It's out of my hands." “I'm not helpless. I can make a difference” Hazardous Attitudes and their Antidotes Attitude Example Antidote

30
Wrong Gas: a rare event

31
Compressors Coolers/Dryers

32
Wrong Gas: a rare event Tanks Valves Backup System

33
Incidents with Gases Delivery of an hypoxic gas mixture due to a defective rubber seal of a flowmeter control tube. Eur J Anaesthesiol. 2000 Jul;17(7):456-8. Oxygen contamination of the nitrous oxide pipeline supply. Anaesth Intensive Care. 1998 Apr;26(2):207-9. Failure of operating room oxygen delivery due to a structural defect in the ceiling column Masui. 2000 Oct;49(10):1165-8. Pollution of the medical air at a university hospital in the metropolitan Tokyo area. Journal of Clinical Anesthesia. 14(3):193-5, 2002. Wrong connection of a flexible medical air hose to a nitrous oxide outlet caused by a defective safety device. Annales Francaises d Anesthesie et de Reanimation. 15(5):683-5, 1996. Contamination of the medical air supply with oxygen: a clinical engineering incident investigation. Journal of Clinical Engineering. 15(4):295-300, 1990. Medical air contamination with oxygen associated with the BEAR 1 and 2 ventilators. Critical Care Medicine. 16(4):362, 1988. Delivery of an hypoxic gas mixture due to a defective rubber seal of a flowmeter control tube. Eur J Anaesthesiol. 2000 Jul;17(7):456-8. Oxygen contamination of the nitrous oxide pipeline supply. Anaesth Intensive Care. 1998 Apr;26(2):207-9. Failure of operating room oxygen delivery due to a structural defect in the ceiling column Masui. 2000 Oct;49(10):1165-8. Pollution of the medical air at a university hospital in the metropolitan Tokyo area. Journal of Clinical Anesthesia. 14(3):193-5, 2002. Wrong connection of a flexible medical air hose to a nitrous oxide outlet caused by a defective safety device. Annales Francaises d Anesthesie et de Reanimation. 15(5):683-5, 1996. Contamination of the medical air supply with oxygen: a clinical engineering incident investigation. Journal of Clinical Engineering. 15(4):295-300, 1990. Medical air contamination with oxygen associated with the BEAR 1 and 2 ventilators. Critical Care Medicine. 16(4):362, 1988.
: Oxygen contamination of the nitrous oxide pipeline supply. Anaesth Intensive Care Apr;26(2): Failure of operating room oxygen delivery due to a structural defect in the ceiling column Masui Oct;49(10): Pollution of the medical air at a university hospital in the metropolitan Tokyo area. Journal of Clinical Anesthesia. 14(3):193-5, Wrong connection of a flexible medical air hose to a nitrous oxide outlet caused by a defective safety device. Annales Francaises d Anesthesie et de Reanimation. 15(5):683-5, Contamination of the medical air supply with oxygen: a clinical engineering incident investigation. Journal of Clinical Engineering. 15(4): , Medical air contamination with oxygen associated with the BEAR 1 and 2 ventilators. Critical Care Medicine. 16(4):362, Delivery of an hypoxic gas mixture due to a defective rubber seal of a flowmeter control tube. Eur J Anaesthesiol Jul;17(7): Oxygen contamination of the nitrous oxide pipeline supply. Anaesth Intensive Care Apr;26(2): Failure of operating room oxygen delivery due to a structural defect in the ceiling column Masui Oct;49(10): Pollution of the medical air at a university hospital in the metropolitan Tokyo area. Journal of Clinical Anesthesia. 14(3):193-5, Wrong connection of a flexible medical air hose to a nitrous oxide outlet caused by a defective safety device. Annales Francaises d Anesthesie et de Reanimation. 15(5):683-5, Contamination of the medical air supply with oxygen: a clinical engineering incident investigation. Journal of Clinical Engineering. 15(4): , Medical air contamination with oxygen associated with the BEAR 1 and 2 ventilators. Critical Care Medicine. 16(4):362,")
34
Fixation: Everything is OK Patient complaining of pain Free air the abdomen Cost center discrepancies Patient complaining of pain Free air the abdomen Cost center discrepancies

35
Anaphylaxis Forty-two anesthetists in teams of two attended training sessions with a critical incident of anaphylactic shock in a full-scale simulator. None of the teams made the correct diagnosis within 10 min and treatment according to the treatment sequence was not initiated. Only 6/21 teams considered the right diagnosis only after hints from the instructor 15 min after the start of the incident. Conclusion: Anaphylactic shock was difficult to diagnose and no structured plans were used for the treatment in the simulated incident in this study. Forty-two anesthetists in teams of two attended training sessions with a critical incident of anaphylactic shock in a full-scale simulator. None of the teams made the correct diagnosis within 10 min and treatment according to the treatment sequence was not initiated. Only 6/21 teams considered the right diagnosis only after hints from the instructor 15 min after the start of the incident. Conclusion: Anaphylactic shock was difficult to diagnose and no structured plans were used for the treatment in the simulated incident in this study. Jacobsen J, Lindekaer AL, Ostergaard HT, et al. Management of anaphylactic shock evaluated using a full-scale anaesthesia simulator. Acta Anaesthesiol Scand 2001 (Department of Anaesthesiology; Section of Simulation; Herlev Hospital; DK-2730 Herlev; Denmark)
.")
36
Drugs Involved in Perioperative Anaphylaxis Data from: Hepner: Anaphylaxis during the perioperative period. Anesth Analg, Volume 97(5).November 2003.1381-1395 12% 8% 4% 3% 1% 3% 69% Muscle Relaxants Latex Antibiotics Hypnotics Colliods Opioids Other
.November % 8% 4% 3% 1% 3% 69% Muscle Relaxants Latex Antibiotics Hypnotics Colliods Opioids Other.")
37
Treatment of Perioperative Anaphylaxis from: Hepner: Anaphylaxis during the perioperative period. Anesth Analg, Volume 97(5).November 2003.1381-1395
.November")
38
Modified from: Hepner: Anaphylaxis during the perioperative period. Anesth Analg, Volume 97(5).November 2003.1381-1395 Treatment of Perioperative Anaphylaxis
.November Treatment of Perioperative Anaphylaxis.")
39
Malignant Hyperthermia

41
Dantrolene 20mg/ampule 60 cc’s of sterile water Dose: 2.5mg/kg (1mg/lb) 100kg patient = 10 ampules
 100kg patient = 10 ampules")
43
A. Line Infection Ortega R, Rengasamy SK, Lewis KP: Infection after radial artery catheterization. Anesth Analg 2002;95:780-7

44
Amyloidosis

45
Compartment Syndrome

46
Impalement of the Brain

47
Broken Needle in Aorta

48
Ventilator Failure Ortega RA, Vrooman B, Hito r: Another Cause for Ventilator Failure. Anesthesiology. Accepted for publication Jan 2006

49
Fire Ortega RA: A Rare Cause of Fire in the Operating Room. Anesthesiology. 89(6):1608, December 1998. Ortega RA: A Rare Cause of Fire in the Operating Room. Anesthesiology. 89(6):1608, December 1998.
:1608, December Ortega RA: A Rare Cause of Fire in the Operating Room. Anesthesiology. 89(6):1608, December")
50
The Fire Triad Fire Triad Ignition Source Fuel Oxidizer

51
MAC EDITORIAL MAC should stand for Maximum Anesthesia Caution, NOT Minimal Anesthesiology Care Hug CC: Anesthesiology: Volume 104(2) February 2006 pp 221-223 EDITORIAL MAC should stand for Maximum Anesthesia Caution, NOT Minimal Anesthesiology Care Hug CC: Anesthesiology: Volume 104(2) February 2006 pp 221-223
 February 2006 pp EDITORIAL MAC should stand for Maximum Anesthesia Caution, NOT Minimal Anesthesiology Care Hug CC: Anesthesiology: Volume 104(2) February 2006 pp")
52
Closed Claims Injury and Liability Associated with Monitored Anesthesia Care: A Closed Claims Analysis Bhananker SM, Posner KL, Cheney FW, Caplan RA et al: Anesthesiology: Volume 104(2) Feb 2006 pp 228-234 Injury and Liability Associated with Monitored Anesthesia Care: A Closed Claims Analysis Bhananker SM, Posner KL, Cheney FW, Caplan RA et al: Anesthesiology: Volume 104(2) Feb 2006 pp 228-234
 Feb 2006 pp Injury and Liability Associated with Monitored Anesthesia Care: A Closed Claims Analysis Bhananker SM, Posner KL, Cheney FW, Caplan RA et al: Anesthesiology: Volume 104(2) Feb 2006 pp")
53
Mechanism of Injury Bhananker SM et al: Anesthesiology: Volume 104(2) Feb 2006 pp 228-234
 Feb 2006 pp")
54
Fires Bhananker SM et al: Anesthesiology: Volume 104(2) Feb 2006 pp 228-234
 Feb 2006 pp")
55
MAC: Take Home Message Least qualified anesthetist assigned Diligence often less by anesthetist and surgeon History of safety (Resting On Your Laurels) Limited pre-anesthetic evaluation Surgeons may explain MAC as: “a nap” Competing goals: surgeon/anesthetist/patient Head and neck procedures: conflict with airway Antiseptic solutions disguise skin color changes Head and trunk draping reduces respiration visibility Least qualified anesthetist assigned Diligence often less by anesthetist and surgeon History of safety (Resting On Your Laurels) Limited pre-anesthetic evaluation Surgeons may explain MAC as: “a nap” Competing goals: surgeon/anesthetist/patient Head and neck procedures: conflict with airway Antiseptic solutions disguise skin color changes Head and trunk draping reduces respiration visibility
 Limited pre-anesthetic evaluation Surgeons may explain MAC as: a nap Competing goals: surgeon/anesthetist/patient Head and neck procedures: conflict with airway Antiseptic solutions disguise skin color changes Head and trunk draping reduces respiration visibility Least qualified anesthetist assigned Diligence often less by anesthetist and surgeon History of safety (Resting On Your Laurels) Limited pre-anesthetic evaluation Surgeons may explain MAC as: a nap Competing goals: surgeon/anesthetist/patient Head and neck procedures: conflict with airway Antiseptic solutions disguise skin color changes Head and trunk draping reduces respiration visibility")
56
MAC: Take Home Message continued… Monitor displays poor visibility Audible monitor signals drowned out by music/noise Impeded Auscultation of heart and lungs Personnel inexperienced in resuscitation techniques Oxygen delays Hgb desaturation while CO2 rises Drug effect onset ≠ peak effect Failure to check anesthesia/resuscitative equipment Oxygen and nitrous oxide are oxidizers Monitor displays poor visibility Audible monitor signals drowned out by music/noise Impeded Auscultation of heart and lungs Personnel inexperienced in resuscitation techniques Oxygen delays Hgb desaturation while CO2 rises Drug effect onset ≠ peak effect Failure to check anesthesia/resuscitative equipment Oxygen and nitrous oxide are oxidizers

57
Administrative Guidelines for Response to an Adverse Anesthesia Event Journal of Clinical Anesthesia. 5(1):79-84, 1993 Jan-Feb www.APSF.org Primary anesthetist concentrates on continuing patient care. Notify a physician responsible for supervision of anesthesia activities Sequester equipment Contact the hospital Risk Manager immediately anesthesiologist and other individuals document relevant information After discussion with the incident supervisor, write on medical record relevant information about what happened and actions taken Complete and file incident report as soon as practical State only facts. Do not use judgmental terms Consult early and frequently with the surgeon. Immediately call other consultants who may help improve long term care Primary anesthetist concentrates on continuing patient care. Notify a physician responsible for supervision of anesthesia activities Sequester equipment Contact the hospital Risk Manager immediately anesthesiologist and other individuals document relevant information After discussion with the incident supervisor, write on medical record relevant information about what happened and actions taken Complete and file incident report as soon as practical State only facts. Do not use judgmental terms Consult early and frequently with the surgeon. Immediately call other consultants who may help improve long term care
:79-84, 1993 Jan-Feb Primary anesthetist concentrates on continuing patient care. Notify a physician responsible for supervision of anesthesia activities Sequester equipment Contact the hospital Risk Manager immediately anesthesiologist and other individuals document relevant information After discussion with the incident supervisor, write on medical record relevant information about what happened and actions taken Complete and file incident report as soon as practical State only facts. Do not use judgmental terms Consult early and frequently with the surgeon. Immediately call other consultants who may help improve long term care Primary anesthetist concentrates on continuing patient care. Notify a physician responsible for supervision of anesthesia activities Sequester equipment Contact the hospital Risk Manager immediately anesthesiologist and other individuals document relevant information After discussion with the incident supervisor, write on medical record relevant information about what happened and actions taken Complete and file incident report as soon as practical State only facts. Do not use judgmental terms Consult early and frequently with the surgeon. Immediately call other consultants who may help improve long term care.")
58
Summary Match Simulate Avoid Fixation Respect MAC Follow Guidelines Attitude

59
The End

Similar presentations






 Job Hazard Analysis Mishap reporting 1 This class is only intended to familiarize you with the programs in place.>")












 I am encouraged by my colleagues to report any patient safety concerns.>")
