Download presentation
Presentation is loading. Please wait.

1
The evidence: is 24-hour intensivist coverage beneficial? Richard H. Savel, MD, FCCM Associate Professor of Clinical Medicine & Neurology Albert Einstein College of Medicine New York, NY Richard H. Savel, MD, FCCM Associate Professor of Clinical Medicine & Neurology Albert Einstein College of Medicine New York, NY

2
Talk Overview Evidence for benefit of 24/7 Potential downsides of 24/7 Conclusions

3
Conflicts of interest Nothing to disclose

4
24/7 intensivist coverage Better patient care (presumably) Few hospitals have 24/7 (10-20%) Why?
 Few hospitals have 24/7 (10-20%) Why")
5
24/7: What are the questions? What is the data? Is it cost-effective? Are there any downsides?

6
What does the data show? Is 24/7 intensivist coverage effective?

7
Night/weekend admissions Increased mortality of acutely ill patients admitted on nights, weekends, and holidays Partially attributed to lower staffing levels Bell et al. NEJM 2001; 345: 663.

9
Bell et al. Analyzed all acute care admissions from emergency departments in Ontario, Canada, between 1988 and 1997 (3,789,917 admissions). Bell et al. NEJM 2001; 345: 663.
. Bell et al. NEJM 2001; 345:")
10
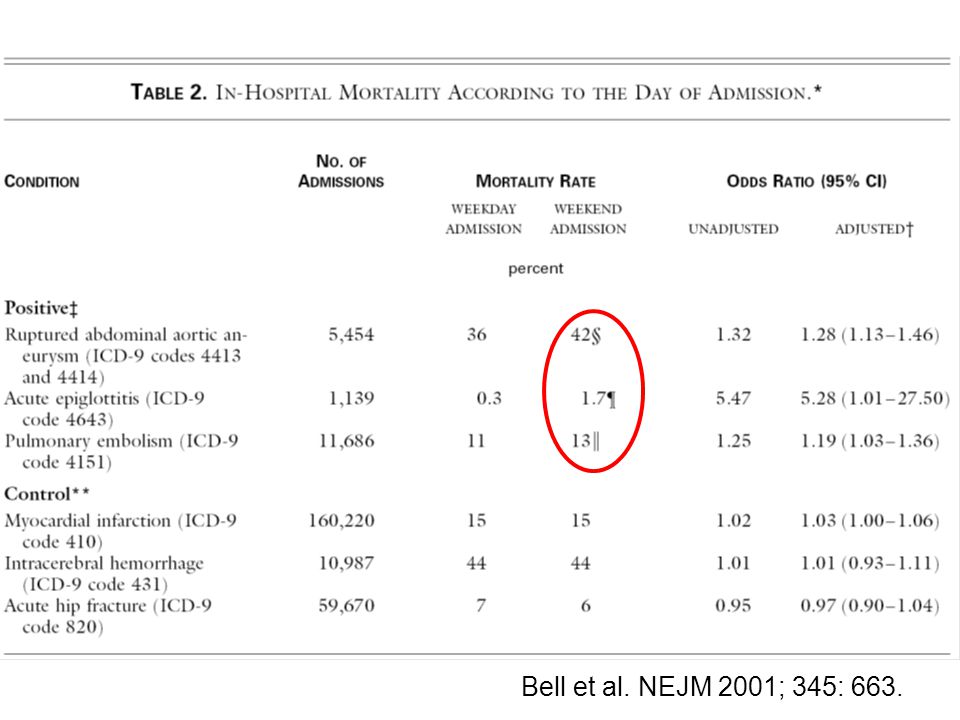
Bell et al. cont. compared weekend vs. weekday in-hospital mortality among patients with three pre-specified diseases: –ruptured abdominal aortic aneurysm (5454 admissions), –acute epiglottitis (1139) –pulmonary embolism(11,686) Also compared weekend vs. weekday in-hospital mortality among patients with three control diseases: –Myocardial infarction (160,220) –intracerebral hemorrhage(10,987) –acute hip fracture (59,670) Bell et al. NEJM 2001; 345: 663.
, –acute epiglottitis (1139) –pulmonary embolism(11,686) Also compared weekend vs. weekday in-hospital mortality among patients with three control diseases: –Myocardial infarction (160,220) –intracerebral hemorrhage(10,987) –acute hip fracture (59,670) Bell et al. NEJM 2001; 345:")
11
Bell et al, cont. as well as for the 100 conditions that were the most common causes of death (accounting for 1,820,885 admissions). Bell et al. NEJM 2001; 345: 663.
. Bell et al. NEJM 2001; 345:")
13
23/100 dx

14
Bell et al., conclusions Certain causes of admission seemed to be associated with higher risk of death if admitted on weekend 23 out of the top 100 reasons for death had a higher likelihood of death if admitted on weekend Reasons unclear

15
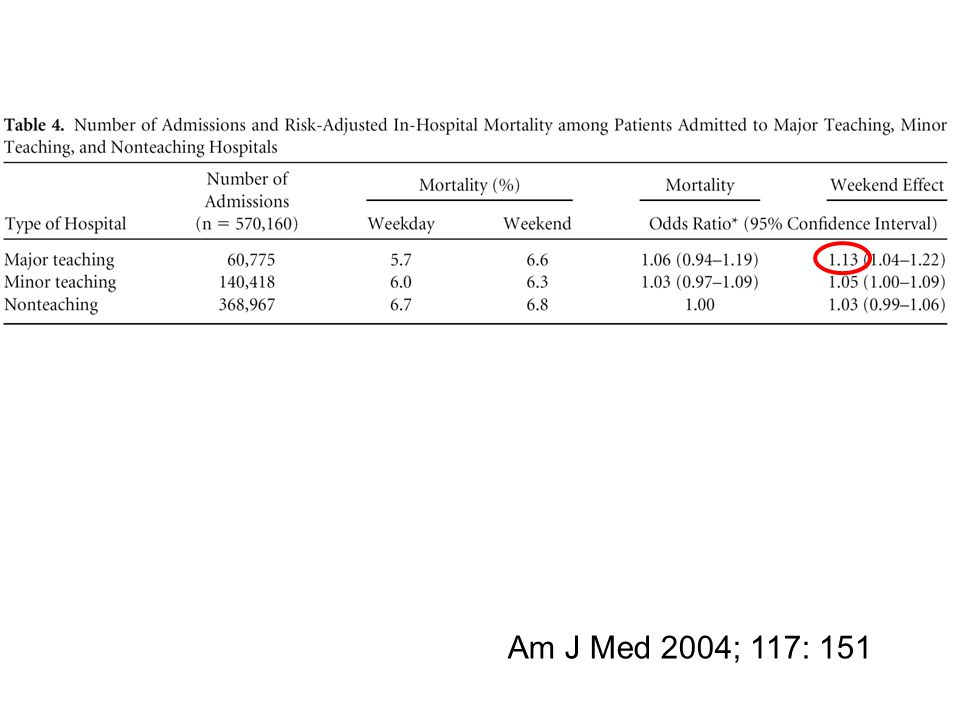
Night/weekend admissions: Larger “weekend” effect shown in major teaching hospitals Even after adjustment for severity of illness Barnett et al. Med Care 2002;40:530 Cram et al. Am J Med 2004; 117: 151. Uusaro et al. Intensive Care Med 2003; 29: 2144.

16
Correlation with day of admission and ICU outcome? Med Care 2002;40:530

17
Barnett et al. Med Care 2002 156,000 patients (1991-97, Ohio) 9% higher mortality if admitted on weekend. But also Fri and Mon Even authors state in discussion not to over interpret study. Concern for unmeasured severity of illness, or selection bias, rather than quality of care.
 9% higher mortality if admitted on weekend. But also Fri and Mon Even authors state in discussion not to over interpret study. Concern for unmeasured severity of illness, or selection bias, rather than quality of care..")
18
Am J Med 2004; 117: 151 In California…

19
Am J Med 2004; 117: 151

21
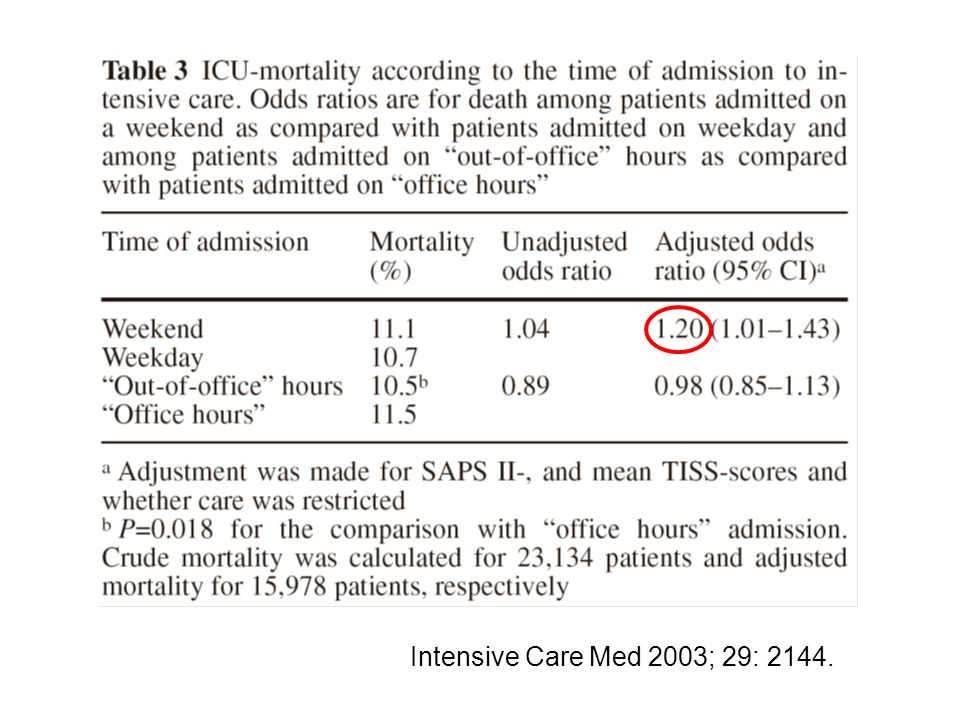
…as well as in Finland. Intensive Care Med 2003; 29: 2144.

23
Outcome: attending vs. fellow/resident Evidence to suggest improved outcome with attendings Decreased resource utilization with attendings Exaggerated “weekend” effect with fellows Higgins et al. CCM 2003; 31: 45 Ensminger et al. Chest 2004; 126:1292 Cram et al. Am J Med 2001; 117: 151

24
CCM 2003; 31: 45 Both long ward stays before ICU admission and lack of full-time ICU physician involvement in care increase the probability of long ICU stays. These latter two factors are potentially modifiable and deserve prospective study.

25
Higgins study: Presence of Critical Care fellow: Independent risk factor for increased: –Weighted hospital days (OR 1.3) –ICU LOS (OR 1.5) “Lack of full-time ICU physician involvement increased the probability of prolonged ICU stay.” Higgins et al. CCM 2003; 31: 45

26
Yet not all data clear Chest 2004; 126:1292

27
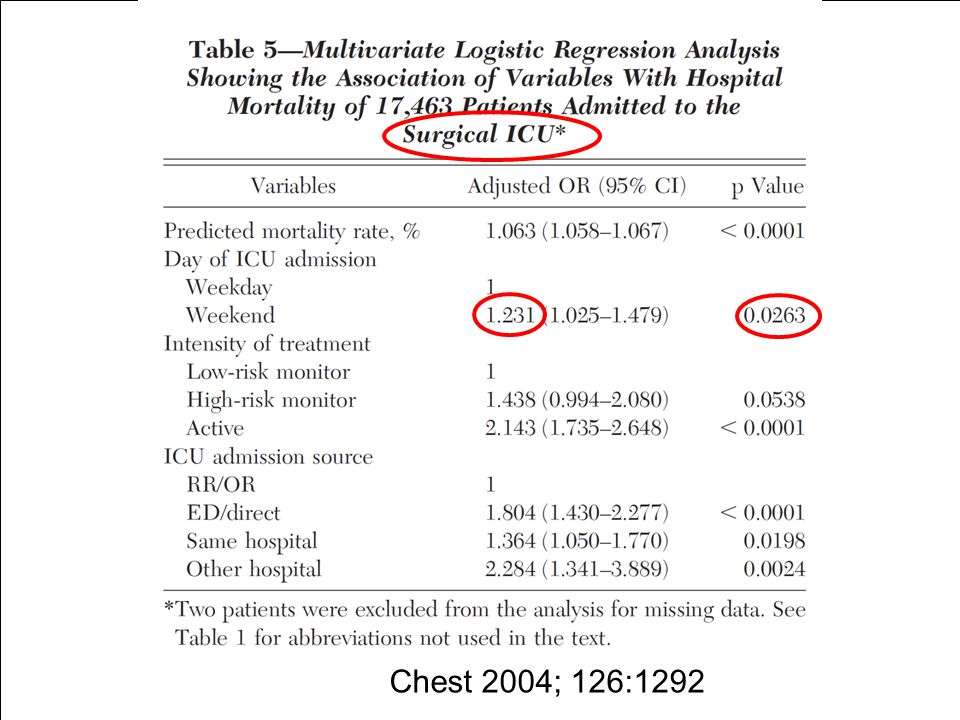
Ensminger 2004 Mayo Clinic Attending present during day By phone at night, present as needed Chest 2004; 126:1292

28
Ensminger 2004 In that study of 29,000 admissions Being admitted to the ICU at night or on weekend did not increase mortality Except in surgical ICU (OR 1.23) Chest 2004; 126:1292
 Chest 2004; 126:1292")
30
Wunsch 2004 Another important study with no differences found with regard to mortality of weekend admissions –After appropriate adjustment for severity of illness

31
So…

32
It appears that patients admitted during nights/weekends may do worse than those admitted during regular hours. What about data that presence of intensivists helps? Some data that being cared for by trainees may not be so great. (an argument for 24/7 coverage)
.")
33
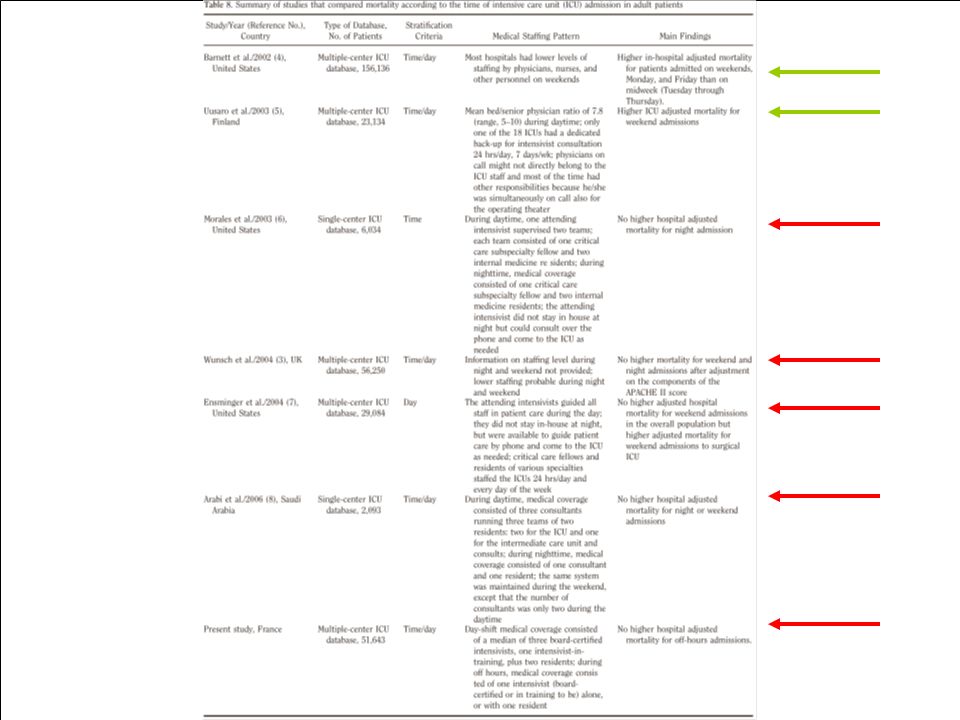
Continuous on-site intensivists A few recent studies formally exploring the relationship between: Hixson, Arabi, Luyt, Gajic Presence of 24/7 intensivistsOutcome and

34
Benefits of 24/7 Conclusions: Using multivariate logistic regression to control for important clinical differences, they found that: –weekend admission –evening admission –had NO significant independent effect on mortality risk Findings are consistent with previous work demonstrating the benefit of intensive care units staffed 24 hrs/day, 7-days/wk by in-house, board- certified intensivists. Pediatr Crit Care Med 2005; 6:523–530

35
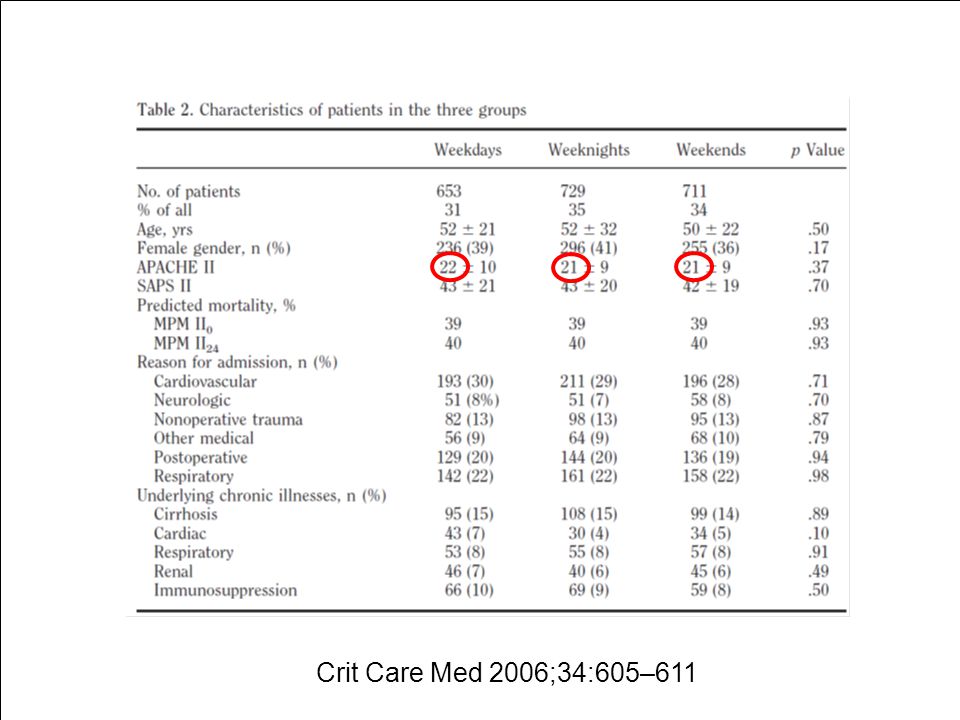
Benefits of 24/7 Arabi 06 In an intensive care unit staffed by onsite certified intensivists 24/7, we found no compromise in the care of patients admitted during weekends and weeknights. These findings suggest that such coverage helps in ensuring consistency of care and therefore represents a potentially improved model for intensive care unit practice. Crit Care Med 2006;34:605–611

36
Arabi CCM 2006 All emergency admissions from March 1 1999 to Feb 28, 2003 Crit Care Med 2006;34:605–611

39
Benefits of 24/7 Conclusions: Admission during off hours is common. Off-hours admissions were not associated with higher mortality and might even be associated with a lower death rate. Crit Care Med 2007; 35: 3-11

40
Luyt CCM 2007 34% day

41
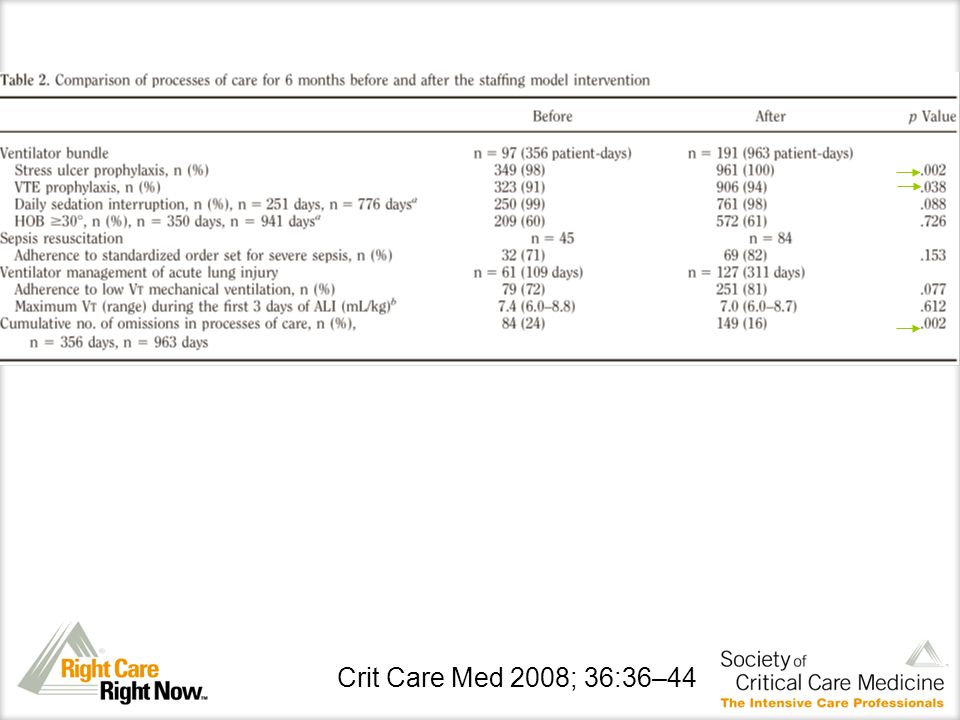
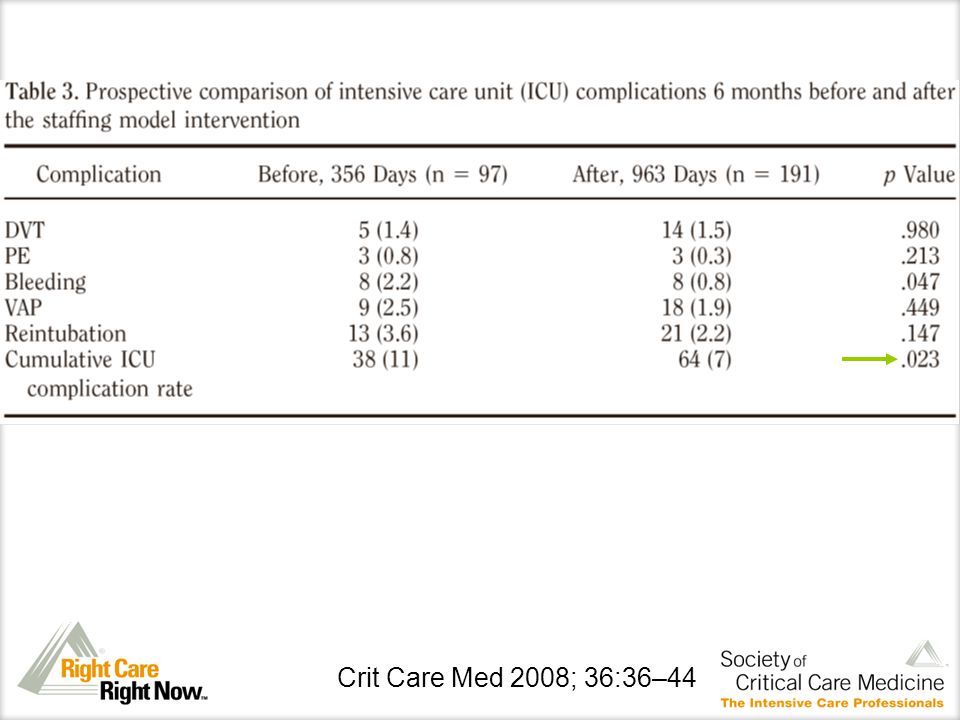
Benefits of 24/7 Crit Care Med 2008; 36:36–44

44
Gajic 2008 Conclusions: The introduction of continuous (24-hr) on-site presence by a staff academic critical care specialist was associated with – improved processes of care and staff satisfaction –decreased intensive care unit complication rate and hospital length of stay. Crit Care Med 2008; 36:36–44

45
Recent data in the cardiac surgery ICU…

46
Ann Thoracic Surg 2009; 88: 1153-61

47
Kumar et al. 2009 in CSICU By adding 24/7 intensivists: –Decreased likelihood of receiving blood 30.2% v. 42.3% (p<0.05) –Less likely to arrive in ICU intubated 43.7% v. 66.5% –Median ICU LOS decreased by 1 day –No change in ICU readmissions or mortality Ann Thoracic Surg 2009; 88: 1153-61
 –Less likely to arrive in ICU intubated 43.7% v. 66.5% –Median ICU LOS decreased by 1 day –No change in ICU readmissions or mortality Ann Thoracic Surg 2009; 88:")
48
So can we make sense of it all? How about a summary slide?

50
Why so confusing? Significant heterogeneity in: How nights and weekends are defined Night and weekend staffing Adjustment for severity of illness *Inherent limitations in study design*

51
What about cost?

52
Is it cost effective? Much increase in manpower Theoretically can increase billing, but usually not enough to cover increased cost 5 FTE for one full time intensivist position Extra funding must be secured in most cases Hendershot et al. J Trauma 2009; 67: 196-9

53
What are the downsides?

54
Downsides of 24/7 coverage (?) Unclear that it is necessary for good outcomes Interfere with training (?) Burnout issues
 Unclear that it is necessary for good outcomes Interfere with training ( ) Burnout issues")
55
24/7:Necessary? The data remain somewhat conflicted Some argue against the “shift work” mentality

56
24/7: lifestyle issues Conclusions: Though the faculty said that going from day to night shifts increased stress, when they changed the schedule, they found no difference in stress scores. Acad Emerg Med. 2004 ;11:111-4.

57
24/7: Burnout issues Conclusions: Approximately one-half of the intensivists presented a high level of burnout. Organizational factors, but not factors related to the patients, appeared to be associated with burnout. Am J Respir Crit Care Med. 2007;175(7):686-92
:")
58
24/7: Burnout issues Embriaco et al.

59
24/7: training issues Concerns that trainees might lack the ability to act independently and make decisions if attending always around Little data to support this, but an interesting topic

60
24/7: alternatives Hospitalists Telemedicine Physician extenders

61
Hospitalists Conclusions: Improved survival with hospitalists, rather than residents, providing after-hours care when an intensivist is not in house suggests that the quality of care of critically ill patients is improved when more experienced physicians are providing bedside care. Crit Care Med 2003; 31:847–852

62
Telemedicine Technology-enabled remote care can be used to provide continuous ICU patient management and to achieve improved clinical and economic outcomes. This intervention’s success suggests that remote care programs may provide a means of improving quality of care and reducing costs when on-site intensivist coverage is not available. Crit Care Med 2000; 28: 3925–3931

63
Physician extenders Crit Care Med 2008; 36:2888 –2897

64
Kleinpell et al. 2008 Crit Care Med 2008; 36:2888 –2897

65
So, in conclusion…

66
Conclusions Having 24/7 coverage by in-house attending intensivist: –Makes intuitive sense that would be associated with improved outcomes –Data not completely clear –Costly –Multiple possible downsides

67
Conclusions Must do a careful analysis of the needs of your particular institution –(patient care, education, etc.) Must look carefully at financial resources Conclusion for any particular institution will need to be individualized
 Must look carefully at financial resources Conclusion for any particular institution will need to be individualized")
68
Thank you Vladimir Kvetan, MD, FCCM Division of CCM at Montefiore/AECOM

69
Questions?

71
Contact information Richard H. Savel, MD, FCCM Email: rhsavel@gmail.comrhsavel@gmail.com telephone: 718 744 7658

Similar presentations




: A Safety Measure in Emergency Medicine Supported by The Agency for Healthcare Research and Quality, Partnerships in Patient.>")
-Score: Probability of Mass Transfusion as Surrogate for Life Threatening Hemorrhage after Multiple Trauma The.>")













. The relationship between emergency department.>")
