Download presentation
Presentation is loading. Please wait.

1
Information Skills for the Clinician or “feeling good about not knowing everything” 1 Evans Whitaker, M.D., M.L.I.S. Keck School of Medicine Norris Medical Library Los Angeles, CA 90089-9130 ewhitake@usc.eduewhitake@usc.edu; (323) 442-1128 1 stolen from Slawson, D.C., Shaughnessy, A.F., Bennett, J.H. (1994). Becoming a medical information master: feeling good about not knowing everything. Journal of Family Practice, 38(5), 505-517.
 stolen from Slawson, D.C., Shaughnessy, A.F., Bennett, J.H. (1994). Becoming a medical information master: feeling good about not knowing everything. Journal of Family Practice, 38(5),")
2
Technology interlude Get a “Turning Point” remote Synchronize Press “GO” flashing red/green light Enter “4”, “1”, “GO” Press “1/A”, yellow flash = working We will use this periodically today Add feedback about Turning Point system on evaluation form

3
SHAMELESS LIBRARY PLUG: Call, email, IM your local medical librarian early and often!! Go to Norris homepage -- http://www.usc.edu/nml. Click on the HELP link in right upper corner to reach us.http://www.usc.edu/nml ASK QUESTIONS!

4
Introduction No EBM today…previous groups felt they knew enough Pick up (3) handouts and (1) evaluation form Time is cut by 15 minutes – we will move briskly As a long-time clinician I use a practical approach to getting information – whatever works as long as the quality of the information is good I will not spend time reviewing sources from1 st and 2 nd year At the end of the session please complete the evaluation forms -- so we can continue to improve! Thanks in advance

5
I believe I need more training in Evidence-Based Medicine… 1. Strongly Agree 2. Agree 3. I’ve had about the right amount 4. Disagree 5. I’ve had too much already!

6
How comfortable are you with EBM? 1. Very comfortable 2. Comfortable 3. So-so 4. Uncomfortable 5. Very uncomfortable

7
I search MEDLINE (PubMed/Ovid)… *The second full moon in a calendar month, happens about once every 2.5 years 1. Weekly or more frequently 2. Once a month 3. Once in a blue moon 4. Never

8
I use MeSH when I search MEDLINE (Ovid, PubMed)… 1. Always 2. Sometimes 3. Never 4. What’s MeSH?
… 1. Always 2. Sometimes 3. Never 4. What’s MeSH")
9
MeSH Medical Subject Headings Collects all synonyms for a term/ concept under one agreed-upon (by NLM) term Example: heart attack, MI, myocardial infarctionheart attack Searches using MeSH retrieve more articles than those using title or text words Scope Note and Tree help find right term Expand, Focus, Subheadings, and Limits are all much less important
 term Example: heart attack, MI, myocardial infarctionheart attack Searches using MeSH retrieve more articles than those using title or text words Scope Note and Tree help find right term Expand, Focus, Subheadings, and Limits are all much less important")
10
When I search MEDLINE… 1. I am confident I will find what I want (or know the information doesn’t exist) 2. I usually find something useful 3. I sometimes find useful material, but almost always wonder what I am missing. 4. I am not confident searching Ovid/PubMed, I’ll stick with UpToDate!
 2. I usually find something useful 3. I sometimes find useful material, but almost always wonder what I am missing. 4. I am not confident searching Ovid/PubMed, I’ll stick with UpToDate!.")
11
Preferred source for clinical information? 1. eMedicine 2. Google (Scholar) 3. AccessMedicine 4. UpToDate 5. MEDLINE 6. Wikipedia 7. Other
 3. AccessMedicine 4. UpToDate 5. MEDLINE 6. Wikipedia 7. Other.")
12
Introduction 2 Today’s Session: Discuss an approach to finding and using information in the course of your clinical practice Objectives: At the end of the session you will o have heard one way to address this issue o have had a little practice with the resources.

13
Introduction 3 The Problem: Too many questions o 15/d or 2 per 3 patients seen = number of questions generated in a clinical day (Covell, 1985) Not enough time o Little time to search for information Expanding universe o 2 year doubling time on biomedical information How to solve the problem? Have adequate baseline subject specific knowledge Know your information resources Develop good technology and information skills.

14
Introduction 4 Of those 15 questions per clinical day o a few are urgent - the results will change the care of your patient o other questions can wait for answers Today we will focus on urgent questions. o require the ability to find valid, relevant answers in 1-5 minutes The other questions o write them down for later o (you will not remember them otherwise)
.")
15
Where do we get this quick information? Point-of-Care Evidence Pyramid (with apologies to the EBM Evidence Pyramid) “Raw” Primary Literature Opinions of Experts “Curbside Consult” Opinion of Colleagues --varying levels of experience and expertise Predigested Primary Medical Literature UpToDate, ACP Pier, Essential Evidence, Clinical Evidence Ovid EBM Databases, National Guideline Clearinghouse, TRIP database, SUMSearch OvidSP Basic Search A Very Traditional Source Another Very Traditional Source *
 Raw Primary Literature Opinions of Experts Curbside Consult Opinion of Colleagues --varying levels of experience and expertise Predigested Primary Medical Literature UpToDate, ACP Pier, Essential Evidence, Clinical Evidence Ovid EBM Databases, National Guideline Clearinghouse, TRIP database, SUMSearch OvidSP Basic Search A Very Traditional Source Another Very Traditional Source *.")
16
Evidence at Clinical Speed From Y1 and Y2 (will not repeat today) UpToDate ACP Pier Essential Evidence Clinical Evidence National Guideline Clearinghouse New today GoogleScholar Scirus.com Ovid Basic Search TRIP Database Clinical Information Tools
 UpToDate ACP Pier Essential Evidence Clinical Evidence National Guideline Clearinghouse New today GoogleScholar Scirus.com Ovid Basic Search TRIP Database Clinical Information Tools")
17
Google Scholar The library world’s “elephant in the room”* Good resource, like all “tools” it has its “best uses” Pros: o Scholar limits Google searches to “scholarly sites” o Familiar interface o Can link to USC resources (change “Scholar Preferences”) o "Sensitive" - searches full text of articles Cons: o Wide range of validity, currency, relevance – requires careful screening of materials o Exclusive users miss the most specific, powerful medical information tools o Not "specific" - includes articles not truly related to topic *”an English idiom for an obvious truth that is being ignored or goes unaddressed” – stolen from Wikipedia (which is another pachyderm).
 o Sensitive - searches full text of articles Cons: o Wide range of validity, currency, relevance – requires careful screening of materials o Exclusive users miss the most specific, powerful medical information tools o Not specific - includes articles not truly related to topic * an English idiom for an obvious truth that is being ignored or goes unaddressed – stolen from Wikipedia (which is another pachyderm).")
18
Google Scholar What is it good for? o To begin exploration of a new topic area o To find search terms Limitations o Too much information to sort o Validity, currency, relevancy vary widely Thing to know: o Set Scholar Preferences for Library to "University of Southern California" on your home computer (full text links)
.")
19
Scirus.com Massive database of “scientific websites” Product of Elsevier Material is better screened than Google Scholar, but still variable in quality Same uses as Google Scholar Can set library preferences like GS

20
OvidSP Basic Rapid “Google-like” searches “Include related terms” must be checked ≥500 hits is the norm o “Good ones” in first 20 to 30 hits o Nothing good? reword your search or go to Advanced For this class only use Ovid training account: o http://ovidsp.ovid.com http://ovidsp.ovid.com o username: sci001; password: medical Create a personal account o save searches o have new articles from saved searches sent to you o annotate articles

21
OvidSP Basic Search Search for “laparoscopic colectomy” “Complete reference” of a good article “MeSH Subject Headings” -- can be used to construct a search similar to Advanced Ovid Search Example Ovid Basic can combine with AND or OR can use limits

22
TRIP Database (Turning Research Into Practice) tripdatabase.com tripdatabase.com Free EBM database Information pulled from multiple sources Lacks full text links Keyword searches Contains: o EBM information o patient handouts o medical images Try - “Ottawa ankle rules” in EBM for X-ray decision rule
 tripdatabase.com tripdatabase.com Free EBM database Information pulled from multiple sources Lacks full text links Keyword searches Contains: o EBM information o patient handouts o medical images Try - Ottawa ankle rules in EBM for X-ray decision rule")
23
Hands on exercise 1: Lumps Two simple clinical scenarios follow… Copies of the scenarios are on your desks.

24
Lumps 1 34 y.o. woman G1 P1 L1 (1.5 year old girl) noticed a lump in her left breast while doing a self breast exam. Menarche 12.5Y Her last period was three weeks ago, cycles are regular 28d. No hormonal medications. FMHx: Maternal aunt died from premenopausal breast cancer. PE: Your exam confirms a 1.5 cm smooth, mobile non-tender nodule in the upper outer quadrant of the left breast. Otherwise breast and axillary exam are normal for age. What do you do? You have two or three minutes while your patient dresses. You do not have a subscription to UpToDate, your books are still in a box at home, your partners all took vacation for 2 weeks when you started work, and your parents are not doctors.
 noticed a lump in her left breast while doing a self breast exam. Menarche 12.5Y Her last period was three weeks ago, cycles are regular 28d. No hormonal medications. FMHx: Maternal aunt died from premenopausal breast cancer. PE: Your exam confirms a 1.5 cm smooth, mobile non-tender nodule in the upper outer quadrant of the left breast. Otherwise breast and axillary exam are normal for age. What do you do. You have two or three minutes while your patient dresses. You do not have a subscription to UpToDate, your books are still in a box at home, your partners all took vacation for 2 weeks when you started work, and your parents are not doctors..")
25
Lumps 2 Same clinical setting as “Lumps 1” 67 y.o. male in for routine exam. He has no health concerns, no current symptoms, no significant past medical history. His wife “made him come in.” PE: Incidentally discovered on exam is a 1.2 cm non- tender nodule low in the anterior neck, slightly to the right of midline. You think this is located in his thyroid gland. You point it out to your patient and he states he never noticed anything, and in fact isn’t sure he feels it now. What do you do? Same information dearth as before.

26
In-class Assignment 1 Divide into groups of 2-4 One half of room gets neck nodule, other half gets breast lump No UpToDate, use electronic sources at Norris Medical Library You have 6 minutes to come up with a plan. I want to know o The plan o What resources you drew on to make your plan o How reliable is your information? o What else would you like to know? Each group prepare to present... o Pick a spokesperson, we’ll discuss afterwards.

27
Points of Discussion -- Breast Breast Patient is premenstrual, aunt’s hx does not appreciably increase risk. SBE finding most common reason for visit to PCP for breast lump evaluation. Waiting until 3-10d post next menses is reasonable, although this kind of waiting and re-exam is only specifically mentioned in one guideline I found. Persistent nodule merits aspiration, consideration of US, Mammography, referral to Surgery (or OB/GYN, depending on community). Breast cyst aspiration is potentially a primary care procedure. "Triple-test" Answers found in UTD, EE, ACP Pier, NGC, Multi- eBook search, etc.
. Breast cyst aspiration is potentially a primary care procedure. Triple-test Answers found in UTD, EE, ACP Pier, NGC, Multi- eBook search, etc..")
28
Points of Discussion -- Thyroid Thyroid 4-7% of population have thyroid nodules (Mazzaferri, E.L.,1993) Increased cancer risk in those >60 y.o. Overall cancer risk in a given nodule is <5%. Women constitute >75% of those with thyroid nodules; men have higher risk of cancer in a given nodule This patient is asymptomatic Bottom line is that FNA needs to be performed by experienced practitioner. Many recommend TSH or ultrasound before FNA. That is debated Answers found in multiple sites. The answers consistent with one another

29
Other things…philosophical It is OK to tell your patient that you don’t know the answer... Tell them you will investigate and get back to them Do not forget to follow up!! Set an agenda for yourself to get back in touch with your patient and follow through on it. Some clinicians re-schedule patients a day to a week later to “guarantee” closure.

30
Hands-on interlude 2: Blood Similar to the Lumps exercise. Stay in your same groups. Try using different resources this time, continue to stay away from UpToDate!

31
Blood Two problems: First 50 y.o. man in for routine exam requests PSA testing. Father with prostate cancer at 75 y.o. Prostate exam (DRE) normal today. Wants free and total PSA. What do you tell him? What is your advice based on?
 normal today. Wants free and total PSA. What do you tell him. What is your advice based on .")
32
Blood 2 Second 47 y.o. woman requesting BRCA1/2 genetic testing. She is a mother of 2 and healthy. Mother and older sister with breast cancer -- both before menopause. Neither family member has been genetically tested. Do you order the test?

33
Would you order his PSA? 1. Yes, he wants it and evidence supports the decision. 2. Yes, he wants it, “the patient is always right”. 3. Unsure. 4. No, evidence does not support ordering it.

34
Discussion -- PSA “Contentious issue” The science is unclear discuss pros/cons with your patient informed decision What about cost aspects? If not clearly effective should we spend national healthcare dollars here? In the US the “haves” get what we want The “have nots” don’t get basic medical care Can we continue in this mode?

35
Would you order BRCA testing on your patient? 1. Yes 2. No 3. Unsure

36
Discussion – BRCA testing This woman has a high risk family history – raised her lifetime risk from US average of ~11% to ~25% She is at increased risk of carrying a BRCA mutation – 5% have the mutation If she has BRCA mutation risk is ~65-80% The consensus seems to be that she should be referred for genetic counseling To understand the implications of testing (insurance, cost, etc.) To consider asking her family members to be tested To consider whether knowing the result changes anything about: – screening – consideration of chemoprevention – prophylactic mastectomy, etc.
 To consider asking her family members to be tested To consider whether knowing the result changes anything about: – screening – consideration of chemoprevention – prophylactic mastectomy, etc.")
37
Changing topics…. PDA’s … an opinionated view

38
Do you now use a PDA or “smart phone”? 1. Yes 2. No, but I soon plan to 3. No

39
PDA users...what do you use? 1. Smartphone, not Blackberry or iPhone 2. Blackberry 3. iPhone 4. SymbianOS device 5. Google Android 6. PDA - PalmOS 7. PDA – Windows Mobile or PPC 8. Other

40
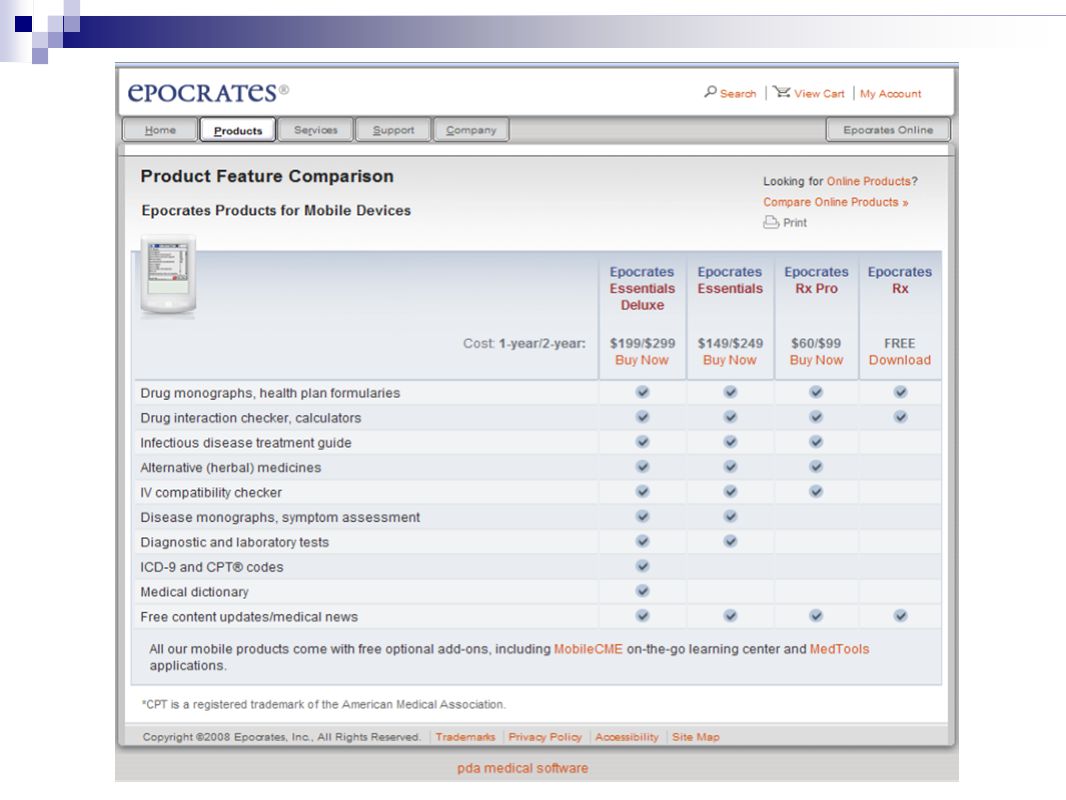
Favorite medical software for your PDA? What other medical PDA software do you recommend? What do you like about it? http://www.usc.edu/e_resources/hsl/lists/sub_1 27.php 1. Epocrates 2. Essential Evidence 3. UpToDate 4. ACP Pier 5. Other

41
Assumptions One gadget is better than two Availability of medical software is driven by demand for the device Browsing capability is important Choose a company with a future Smartphone Blackberry, iPhone are ascendant As above

42
Blackberry vs. iPhone True keyboard (except Storm) 3G connectivity microSD card storage 1-2GB Medical applications now, many more to come Bold $299 (with current discount) and $40/mo. phone, $30/mo. Data Several service providers “What you need” Touch screen “keyboard” with “intelligent fill” 3G connectivity 8 vs. 16 GB (iTunes fxn.) Medical applications few at present, with unclear plans to encourage development in the future iPhone 3G 16GB $299, with same mo. Costs Must switch to AT&T “What you want”
 3G connectivity microSD card storage 1-2GB Medical applications now, many more to come Bold $299 (with current discount) and $40/mo. phone, $30/mo. Data Several service providers What you need Touch screen keyboard with intelligent fill 3G connectivity 8 vs. 16 GB (iTunes fxn.) Medical applications few at present, with unclear plans to encourage development in the future iPhone 3G 16GB $299, with same mo. Costs Must switch to AT&T What you want .")
43
Review of Reviews Reviewers complained about slow typing/ high error rate with iPhone vs. BlackBerry Reviewers felt that all other aspects seemed similar (and good) Noted on recent poll that 79% iPhone users were “very satisfied” or better, vs. 54% of BlackBerry users Reviewers felt that Apple planned to tightly control software development – unknown future for new medical products. BlackBerry software development moving rapidly.
 Noted on recent poll that 79% iPhone users were very satisfied or better, vs. 54% of BlackBerry users Reviewers felt that Apple planned to tightly control software development – unknown future for new medical products. BlackBerry software development moving rapidly..")
44
Wrap Up

45
Strategy…1 Bookmark Norris home page - starting point for all information seeking during your USC career First UpToDate (Off-campus? … Use ACP Pier, Essential Evidence, Clinical Evidence) Enter one central concept; scan results; select best match. Interesting Study: ACP Pier, InfoRetriever (now Essential Evidence), UpToDate, FirstCONSULT, and DISEASEDEX were compared (Campbell, 2006). The 18 participant were each given 3 clinical questions, and given 3 minutes to answer each question. Results showed that users found significantly more answers with UTD than other products. They heavily preferred UTD interface, and felt more confident about the results from UTD!
 Enter one central concept; scan results; select best match. Interesting Study: ACP Pier, InfoRetriever (now Essential Evidence), UpToDate, FirstCONSULT, and DISEASEDEX were compared (Campbell, 2006). The 18 participant were each given 3 clinical questions, and given 3 minutes to answer each question. Results showed that users found significantly more answers with UTD than other products. They heavily preferred UTD interface, and felt more confident about the results from UTD!.")
46
Strategy…2 If you are not finding what you want in the clinical information tools… Second Option OvidSP Basic Search You may be able to find a paper, scan it for information within a short time frame. OR Consider EBM sources Tripdatabase.com OR Clinical Evidence Third Use GoogleScholar, Scirus.com for failures of more specific biomedical sources.

47
Thanks for your attention!! Please fill out evaluations before you leave! Feel free to contact me if you have information questions.

48
References Adair, R.F., Holmgren, L.R., (2005) Do drug samples influence resident prescribing behavior? A randomized trial. American Journal of Medicine, 118, 881-884. Allison, J.J., Kiefe, C.I., Weissman, N.W., Carter, J., Centor, R.M. (1999). The art and science of searching MEDLINE to answer clinical questions: Finding the right number of articles. Intl J Tech Assess in Health Care, 15(2), 281- 296. Barry, H.C., Ebell, M.H., Shaughnessy, A.F., Slawson, D.C., Nietzke, F. (2001). Family physicians’ use of medical abstracts to guide decision making: style or substance? Am Board of FP, 14(6), 437-442. Campbell, R. (2006). An evaluation of five bedside information products using a user-centered, task-oriented approach. J Med Lib Assoc, 94(4), 435-440. Covell, D.G., Uman, G.C., Manning, P.R. (1985). Information needs of office practitioners: are they being met? Annals of Internal Medicine, 103, 596-599. Guyatt, G., Rennie, D. (2002). Users’ Guides to the Medical Literature: Essentials of Evidence-Based Clinical Practice. Chicago: AMA. Greenhalgh, T. (2006). How to read a paper: The basics of evidence-based medicine, 3rd ed. Malden, MA: Blackwell. Mazzaferri, E.L. (1993). Management of a solitary thyroid nodule. N Engl J Med, 328, 553-559. Michaud, G., McGowan, JL., van der Jagt, R., Wells, G., & Tugwell, P. (1998). Are therapeutic decisions supported by evidence from health care research? Archives of Internal Medicine158(15),1665-1668. Shaughnessy, A.F., Ebell, M.H., Slawson, D.C. (2008). Information mastery: Basing care on the best available evidence. In Essentials of Family Medicine, 5th ed. Philadelphia: Wolters. Slawson, D.C., Shaughnessy, A.F., Bennett, J.H. (1994). Becoming a medical information master: feeling good about not knowing everything. Journal of Family Practice, 38(5), 505-517. Slawson, D.C. (2005). Teaching evidence-based medicine: should we be teaching information management instead? Acad Med, 80(7), 685-689 Wilczynski, N.L., Walker, C.J., McKibbon, K.A., Haynes, R.B. (1995). Reasons for the loss of sensitivity and specificity of methodologic MeSH terms and textwords in MEDLINE. Proc Annu Symp Comp Appl Med Care, 19, 436-440.
. The art and science of searching MEDLINE to answer clinical questions: Finding the right number of articles. Intl J Tech Assess in Health Care, 15(2), Barry, H.C., Ebell, M.H., Shaughnessy, A.F., Slawson, D.C., Nietzke, F. (2001). Family physicians’ use of medical abstracts to guide decision making: style or substance. Am Board of FP, 14(6), Campbell, R. (2006). An evaluation of five bedside information products using a user-centered, task-oriented approach. J Med Lib Assoc, 94(4), Covell, D.G., Uman, G.C., Manning, P.R. (1985). Information needs of office practitioners: are they being met. Annals of Internal Medicine, 103, Guyatt, G., Rennie, D. (2002). Users’ Guides to the Medical Literature: Essentials of Evidence-Based Clinical Practice. Chicago: AMA. Greenhalgh, T. (2006). How to read a paper: The basics of evidence-based medicine, 3rd ed. Malden, MA: Blackwell. Mazzaferri, E.L. (1993). Management of a solitary thyroid nodule. N Engl J Med, 328, Michaud, G., McGowan, JL., van der Jagt, R., Wells, G., & Tugwell, P. (1998). Are therapeutic decisions supported by evidence from health care research. Archives of Internal Medicine158(15), Shaughnessy, A.F., Ebell, M.H., Slawson, D.C. (2008). Information mastery: Basing care on the best available evidence. In Essentials of Family Medicine, 5th ed. Philadelphia: Wolters. Slawson, D.C., Shaughnessy, A.F., Bennett, J.H. (1994). Becoming a medical information master: feeling good about not knowing everything. Journal of Family Practice, 38(5), Slawson, D.C. (2005). Teaching evidence-based medicine: should we be teaching information management instead. Acad Med, 80(7), Wilczynski, N.L., Walker, C.J., McKibbon, K.A., Haynes, R.B. (1995). Reasons for the loss of sensitivity and specificity of methodologic MeSH terms and textwords in MEDLINE. Proc Annu Symp Comp Appl Med Care, 19,")
49
Opinionated recommendations regarding hand held devices in medicine

50
Should a discussion of PDAs be a part of this class? 1. Yes 2. No

51
The Usefulness Equation A quasi-mathematical model of the value of information. (Relevance) x (Validity) x (Size of Effect) (Work) R -- Do the articles, findings and recommendations apply to your patient V – Are the findings true? Are they current? W – Usually synonymous with time, could be synonymous with money if you paid someone to do your research for you. S – How much effect will the intervention have on your patient? (this factor is included in some models)
 x (Validity) x (Size of Effect) (Work) R -- Do the articles, findings and recommendations apply to your patient V – Are the findings true. Are they current. W – Usually synonymous with time, could be synonymous with money if you paid someone to do your research for you. S – How much effect will the intervention have on your patient. (this factor is included in some models).")
52
Evidence at Clinical Speed - Sources CLINICAL INFORMATION TOOLS UpToDate – fast, easy, good quality. Is it evidence- based? Is it expert opinion? Does it matter? UpToDate Essential Evidence – previously InfoRetriever Essential Evidence ACP Pier EBM SOURCES (some quicker than others) Clinical Evidence – Search NLM box in RUQ “clinical evidence” Clinical Evidence Ovid EBM databases –Databases OvidSP select a database, remember Change Databases and Open And Re-execute to speed through Cochrane Systematic Reviews, DARE, ACP Journal Club Ovid EBM databases National Guidelines Clearinghouse (guidelines.gov)- free National Guidelines Clearinghouse TRIP database (tripdatabase.com) – EBM, free TRIP database
 Clinical Evidence – Search NLM box in RUQ clinical evidence Clinical Evidence Ovid EBM databases –Databases OvidSP select a database, remember Change Databases and Open And Re-execute to speed through Cochrane Systematic Reviews, DARE, ACP Journal Club Ovid EBM databases National Guidelines Clearinghouse (guidelines.gov)- free National Guidelines Clearinghouse TRIP database (tripdatabase.com) – EBM, free TRIP database.")
53
PDAs PDA’s date from the mid-90s; they were not more than electronic calendars/rolodexes At this point most users want a device that can “do it all”. The SmartPhone takes care of phone, email, pager, web browsing, plus more traditional PDA tasks of providing drug information, clinical guidelines, performing calculations, organizing addresses and keeping track of your calendar.

54
PDAs 2 This is a rapidly changing area for which I will not even try to provide specifics. OSs are Palm, Windows Mobile/PPC, RIM (BlackBerry), and Symbian (open-source handheld OS). PalmOS has the largest amount of software. Vast amounts of freeware/shareware. WindowsMobile (PocketPC) has caught up on commercial side. Freeware and shareware limited. BlackBerry offerings are rapidly increasing, making this a much more attractive offering. Little free/share ware Symbian is making inroads in US.
, and Symbian (open-source handheld OS). PalmOS has the largest amount of software. Vast amounts of freeware/shareware. WindowsMobile (PocketPC) has caught up on commercial side. Freeware and shareware limited. BlackBerry offerings are rapidly increasing, making this a much more attractive offering. Little free/share ware Symbian is making inroads in US..")
55
Point-of-care clinical information software for PDA

56
Other things you could try…for these two questions… In Ovid, there are no useful answers in the 3 EBM databases o Database Systematic Reviews o DARE o ACP Journal Club Clinical Evidence from BMJ has a nice summary of thyroid nodules. Free EBM information is available from: o TRIP (Turning Research Into Practice) http://www.tripdatabase.com http://www.tripdatabase.com o Agency for Healthcare Research and Quality (http://ahrq.gov/ ) and U.S. Preventive Services Task Force (http://www.ahrq.gov/clinic/uspstfix.htm ).http://ahrq.gov/http://www.ahrq.gov/clinic/uspstfix.htm National Guidelines Clearinghouse (http://guideline.gov/ ) has good EB summaries of both entities.http://guideline.gov/ FPIN (http://www.fpin.org ) Family Physicians Inquiries Network has a searchable collection of questions from family practitioners and answers from FPIN-member FP residencies, medical libraries, etc. http://www.fpin.org
 o Agency for Healthcare Research and Quality ( ) and U.S. Preventive Services Task Force ( ). National Guidelines Clearinghouse ( ) has good EB summaries of both entities. FPIN ( ) Family Physicians Inquiries Network has a searchable collection of questions from family practitioners and answers from FPIN-member FP residencies, medical libraries, etc.")
Similar presentations

 Medical Subject Librarian Team.>")




 Emily Brennan, MLIS Eileen Eandi, MLIS Luis Franco Evans Whitaker, MD, MLIS -->")












