Download presentation
Presentation is loading. Please wait.

1
Universal Health Coverage (UHC) and the Role of Private Hospitals Presented by: Mr. Stephen Baker Director: Halcom Management Services Ltd 25 th September 2013 HMS

2
UHC – Definition HMS “a health care system which provides health care and financial protection to all its citizens” "developing health financing systems so that all people have access to services and do not suffer financial hardships paying for them” World Health Organisation 2010

3
HMS Universal Health Insurance or Universal Coverage? Much of the debate about NHI to date has focused on the breadth or population dimension. While popular perception is sometimes that those without medical schemes “have no cover”, this is not the case. It seems though that there is confusion between universal coverage for healthcare and universal coverage for health insurance. It was estimated that only some 18.6% of Namibians had health insurance cover in 2012. However everyone in the country has access to healthcare, either in the public sector or through medical schemes, or other employer- based arrangements. Dissatisfaction with the current national health system is dissatisfaction with the quality of the care in the public sector. Universal Health Insurance or Universal Coverage?

4
To Achieve UHC HMS A strong, efficient, well-run health system focused on primary, preventative, curative & Rehabilitation Affordability – a system for financing health services so people do not suffer financial hardship when using them. Access to essential medicines and technologies to diagnose and treat medical problems. A sufficient capacity of well-trained, motivated health workers to provide the services to meet patients’ needs based on the best available evidence.

5
UHC Private Stakeholders HMS Revenue Collection Individuals Employers All taxpayers Brokers Pooling Medical Schemes Medical Scheme Members Purchasing Medical Schemes Medical Scheme Administrators Delivery Private Hospitals Pharmaceutical Industry Medical Practitioners Nurses Pharmacists etc.

6
Current Private Hospital sector HMS Total Private beds 578 (very little change over prior years) 9 medical schemes cover ±182 000 lives = 546 beds Private sector running at capacity Beds per 1000 =3,1 1 GRN medical scheme covers ± 221000 lives (Psemas) = 663 beds Total lives covered 18,6% of total population Private Sector characterized by: Quality service Quality Facility & Equipment Expensive Good clinical outcomes
 9 medical schemes cover ± lives = 546 beds Private sector running at capacity Beds per 1000 =3,1 1 GRN medical scheme covers ± lives (Psemas) = 663 beds Total lives covered 18,6% of total population Private Sector characterized by: Quality service Quality Facility & Equipment Expensive Good clinical outcomes")
7
HMS

8
Current Government Hospital sector HMS Total Government beds = 5092 Approx. 1,7 million lives not insured = 5100 beds Beds per 1000 population = 3 Government has enough beds May not all be functional Old facilities May not be in the right areas or where the need is

9
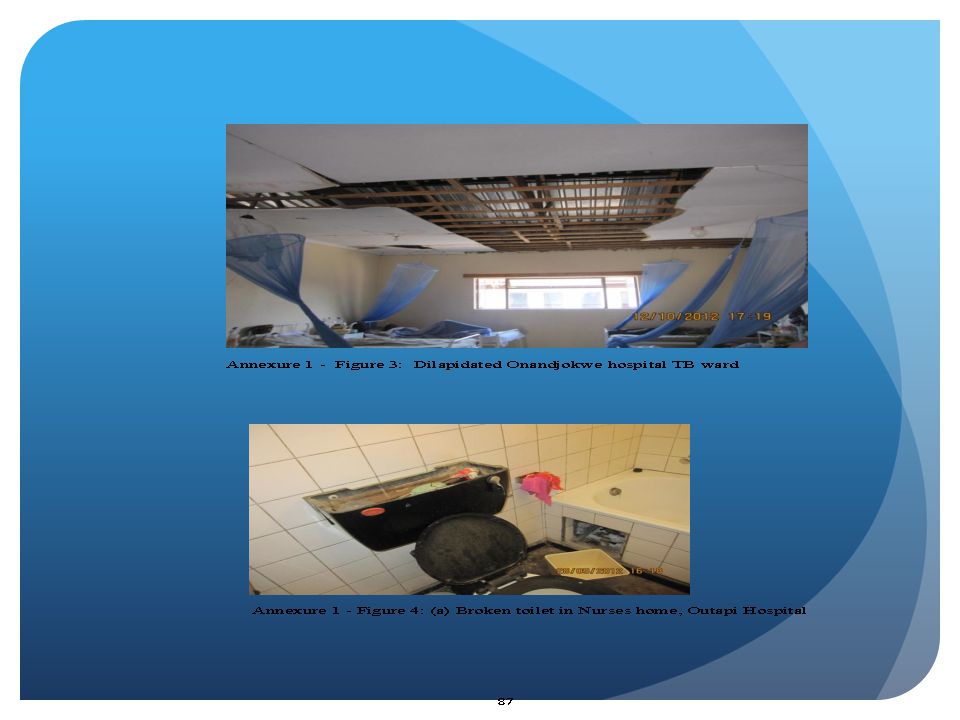
Findings of the “report of the Presidential Commission of enquiry into MOHSS Jan 2013” Shortage of health professionals Quality of patient care sub optimal Quality of training of doctors and nurses needs improvement Quality of facilities – “dilapidation and decay” Poor status of medical equipment Poor transport systems for referred patients HMS

11
Private Hospitals Perspective of UHC HMS Committed to the goals of achieving Universal access to quality healthcare in Namibia Willing to engage Government to develop solutions and be part of the decision making process Able to share data, expertise and in-depth understanding of the private sector in discussions of national health system reform

12
What can the Private Hospital Sector offer HMS Skills Development and Transfer Gap Hospitals Hospital management Services PPP’s Managed Care

13
Skills Development and Transfer HMS Financial Management & Cost accounting expertise Benchmarking techniques Risk Management Clinical Standards Critical Pathways Information Technology Productivity Training Internships

14
Financial Management Zero Based Budgeting Never assume that any cost is forever! Review every structure and process to determine what might have changed and how it has affected cost profile Review patient profile and also detremine what changes might have taken place and how it might affect service delivery and linked resources e.g. staffing, equipment and services Activity based costings “costing methodology that identifies activities in a hospital and assigns the cost of each activity with resources to all products and services according to the actual utilisation”. HMS

15
Benchmarking “The comparison of one’s own hospital to other similar systems (not every hospital is the same and the objective is not meet what others are achieving but to stimulate the thinking as to find better ways of delivering the same, if not improved, services and at more cost effective levels)” “If you can’t measure it, you can’t improve it” Statistics based on Unit Values Nursing Staff cost per patient Average Length of Stay Medicine costs per patient day (PPD) Catering costs PPD Laundry costs PPD Fixed overheads per bed Maintenance costs per bed Admin cost per bed
 If you can’t measure it, you can’t improve it Statistics based on Unit Values Nursing Staff cost per patient Average Length of Stay Medicine costs per patient day (PPD) Catering costs PPD Laundry costs PPD Fixed overheads per bed Maintenance costs per bed Admin cost per bed")
16
Clinical Standards Standards Determine the “best practice” way of doing things, documenting then measuring compliance Identify what needs to be done to achieve optimum quality of service and clinical outcomes Develop, implement, monitor and continuous improvement of SOP’s Hospital accreditation

17
Information Technology Use of Technology Professional resources are in seriously short supply therefore, it is compelling that management finds ways to complement available resources, particularly Nursing staff The “digital” or “paper-less” hospital which implements IT solutions to develop an electronic patinet record (EPR/EMR) Less forms and less people intervention thereby reducing propensity for errors HMS
 Less forms and less people intervention thereby reducing propensity for errors HMS")
18
GAP Hospitals HMS “ Gap Hospitals are typically private hospitals designed, built and operated to cater for lower revenue models than existing medical insurance pays: i.e. for NHI, UHC, Psemas etc.” Typical state of the art hospital costs N$ 2.5 – N$ 2.7 million per bed i.e.: N$ 250 –N$ 270 million for a 100 bed hospital GAP hospital costs > N$ 1.7 million per bed More compact, optimally designed: 60 sq. per bed compared to 90-100 Single story (lifts cost 1 million each) Conservative finishes Rationalise on the latest medical equipment Short point to point distances, optimising efficiency Financial focus is on balancing project capex with revenue streams and opex from proposed case mix
 Conservative finishes Rationalise on the latest medical equipment Short point to point distances, optimising efficiency Financial focus is on balancing project capex with revenue streams and opex from proposed case mix.")
19
HMS Result: GAP hospitals are cheaper to operate and staff Can produce the same IRR on 26% less fees, can also allow risk sharing models i.e.: Per Diems, Capitation etc. Produce the same quality of patient care Can be scaled according to demand (30-40 bed hospitals are viable) Due to flexibility can be located in lower population areas, increasing access to care. GAP hospitals are viable in an NHI setting
 Due to flexibility can be located in lower population areas, increasing access to care. GAP hospitals are viable in an NHI setting.")
20
Hospital Management Services HMS Provide management services to existing hospitals Develop centers of excellence i.e.: (Psychiatric, Level 1 Trauma, Radiation Oncology, Cardiology units)
")
21
PPP’s HMS To develop UHC private sector is able and willing to engage in PPP’s Proposals were made for the Level 1 Trauma Hospital in 2012, inclusive of N$ 200 million in funding in response to MVA requests. MVA are now going to issue another expression of interest. The bulk of forecasted expenditure on PPP’s from the private sector would be hospital construction/renovation

22
HMS

23
Why PPP’s in Healthcare HMS Improving cost efficiency Improving quality of services Modernizing facilities, equipment & services Increasing access to underserved areas & populations

24
What is a PPP in healthcare HMS Government pays Private Operator service payments but only once facility is operational Government defines service and output requirements. Inputs, design, etc. to bidders Buying services, not equipment & facilities. Private party is typically responsible for all or part of the capital financing Payment is tied to performance not inputs/milestones

25
Managed Care HMS “The management of an episode of care from pre- admission to discharge” Objectives: Reduce cost of each episode of care Reduce length of stay Improve patient outcomes Ensure appropriateness of treatment

26
Summary HMS

27
Thank You HMS

Similar presentations


 Saly – Senegal, 15 th - 17 th March 2011 Di McIntyre Chair, AfHEA Scientific.>")







 in Bangladesh Md. Ashadul Islam Director General Health Economics Unit Ministry of Health and.>")


 Sarah Bales Public Policy in Asia,>")





