Download presentation
Presentation is loading. Please wait.

1
POSITIONAL CLONING TWO EXAMPLES

2
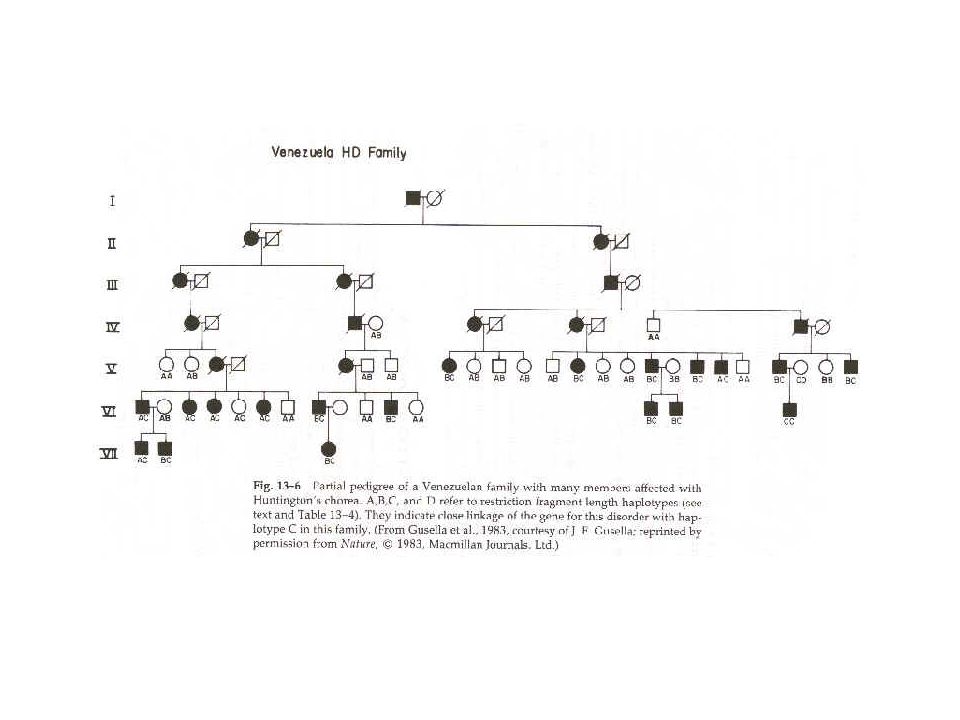
Inheritance pattern - dominant autosomal Entirely penetrant and fatal Frequency - about 1/10,000 live births Late onset - age 35 to 45 No biochemical defect known, until very recently No methods of treatment Because of late onset, many have had children before symptoms appear Huntington's disease

3
Influence of the Wexler family

4
Families with a history of Huntington's disease Indiana University maintains a National Research Roster for Huntington's Patients Large family with a history of Huntington's disease discovered living on shore of lake Maracaibo in Venezuela

6
For both families with a history of Huntington's disease: Blood samples taken from each member Permanent cell lines established Each family member analyzed by a neurologist for disease symptoms Paternity verified

7
Objective: Finding a probe that uncovered an RFLP that was linked to Huntington's disease. 1981 - Gusella's group started with a group of anonymous probes that uncovered RFLPs - very few available. They were incredibly lucky - the 12th probe they tried -called G8 - indicated linkage.

10
Disease associated with the A haplotype in the American family and the C haplotype in the Venezuelan family.

11
LOD Scores

12
1983 - G8 (also called D4S10) mapped approximately 4 cM from the HD locus. It took 10 more years to clone the gene. Why?

13
1986-87 DNA markers were used and D4S10 was localized by in situ hybridization and somatic cell genetics to chromosome region 4p16.3

15
Further linkage studies for isolating HD

17
Identification of Putative Coding Sequences Exon Trapping Use trapped exons to identify candidate genes from cDNAs

18
Four transcripts were analyzed.

20
IT15 - Huntingtin

21
Repeat Sequence Diseases

22
Implications No cure yet Testing is possible Ethical issues arise

23
Cystic fibrosis Autosomal recessive Not late onset Average life expectancy 27 years Treatment but no cure

24
About 1/20 to 1/25 Caucasians are carriers of the defective gene (two carriers have to mate to produce an affected individual). Why is the prevalence of this defect so high?

26
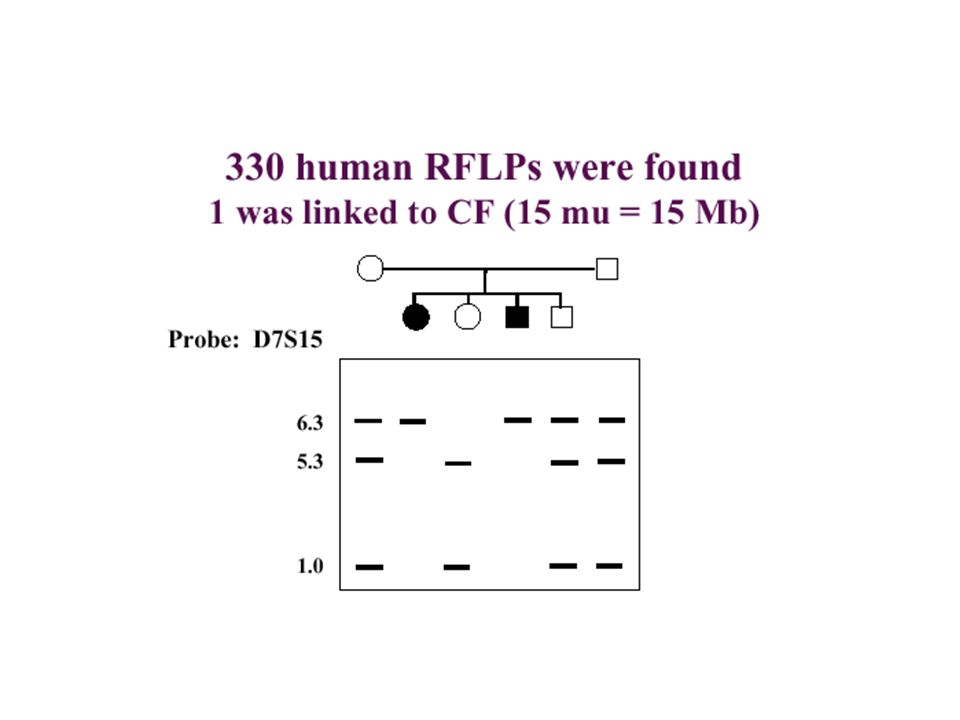
Pedigree Analysis A loosely linked RFLP marker was found. By in situ hybridization, this marker and therefore the CF gene were mapped to chromosome 7.

27
Further RFLP markers known to be located on chromosome 7 were then tested for linkage to CF. Two markers were found that flanked CF, met and D7S8 but they were 1600 kb apart. Eventually two more closely linked markers were found that narrowed the region to about 500 kb.

29
In the case of the CF gene, 7 jumps of 50 to 75 kb were made with each arrival point then serving as a new origin for chromosome walking.

30
The map position agreed with the linkage data The probe had a CpG island at the start of the coding sequence The gene was detected in Northern blots using RNA extracted from the "correct" tissue, in this case cultured epithelial (sweat gland) cells
 cells")
34
Diagnostic tests are available, but extensive testing is necessary because there are so many different mutations.

35
Since the function of the gene is known, treatment strategies can be devised.

36
Gene therapy Insert CFTR gene in adenovirus vector. Virus is used to infect CF patient by inhalation. Virus inserts itself into lung cells, where gene functions normally.

37
Why is disease so prevalent? Selective advantage of heterozygotes? Big gene, many mutations

Similar presentations












>")
Karyotype b)Fluorescence in situ hybridization c)Gene testing d)Biochemical.>")







 is a genetic disorder that is relatively common in some ethnic groups A.>")





 By Me. History First case reported in Sweden. Women and men are affected in equal numbers Common in Caucasians and.>")
