Download presentation
Presentation is loading. Please wait.

1
2012 TMA DQ Course AFMOA/SGAR Current as of 10 May 2012

2
Air Force TMA DQ Course Break-Out Session Overview
Organization Why Data Quality? MTF Engagement Guidance DQ Assurance Team CHCS Provider File Metrics Other DQ Efforts DQ Review List/Statement Guidance & Completion eDQ

3
ORGANIZATION

4
Organization HAF/SG8Y (Policy) AFMOA (Execution)
Chief, Financial Performance Data Quality Program Manager AF Data Quality Manager Program Analyst Data Quality SME/DBA Data Quality SME

5
Organization SGA SGAI SGAL SGAP SGAR SGAT MEPRS DQ UBO Info Services
Med Logistics SGAP Manpower SGAR Resource Mgt SGAT Health Benefits SGAX** Readiness MEPRS DQ UBO

6
AFMOA Strategic Alignment
Mission Support development and oversee execution of Air Force Surgeon General Policies Vision World-class healthcare for our beneficiaries anywhere, anytime Goals Rebuild inpatient platforms to provide clinical currency needed for readiness, GME and warrior care Medical Home to provide efficient, patient centered health care Sustain clinical currency for readiness beyond what our platforms can provide Standard processes where needed to improve quality and reduce waste Population Health Readiness Experience of Care Per Capita Cost

7
Our Mission AFMOA Data Quality
Provide Comprehensive DQ Program Management to all AF MTFs Provide reach-back support to MAJCOMs and DRUs MAJCOMS Air Force MTFs AFMOA Data Quality Standardize methodology Evaluate processes Reduce variance DRUs

8
Data Quality (DQ) Roles and Responsibilities
DQ Program Manager DQ Program Analyst DQ DBA/SME DQ SME Focal point for MTF’s DQ Mgmt Control Program/DQ Statement Teams to provide policy/MTF’s business practice improvements Biometric data consultant Measures MTF/AFMS DQ performance & influences change - Trains MTF DQ Managers Provide CHCS Database Admin SME support -- ID & assist MTFs correct: (Provider File errors, Hospital Location Files, site definable MEPRS tables, etc.) Create CHCS restrictions/business rules to promote standardization Develop CHCS training guides to promote MTF DQ Provide Ad Hoc report assistance to support MTF’s Perform MTF site visits to provide on-site technical assistance Manage performance metrics to validate improvement efforts MTF Engagement: One-on-one support (telephone/DCO/group org box) Bi-monthly meetings (CONUS/PACAF/USAFE) conducted via DCO Both business and training conducted Optimize use of Vector Check Tools/resources/announcements/schedule...eDQ AF portion of the TMA DQ Course Beyond the DQ statement Site Visit philosophy Standardized approach, exhaust other avenues first Mission: Provide Comprehensive DQ Program Management to all MTFs Provide reachback support to MAJCOMs and DRUs Key Objectives: Standardize Methodology Evaluate Processes Reduce Variance Future Initiatives: Consolidation Shape MHS/AFMS DQ efforts
 Create CHCS restrictions/business rules to promote standardization. Develop CHCS training guides to promote MTF DQ. Provide Ad Hoc report assistance to support MTF’s. Perform MTF site visits to provide on-site technical assistance. Manage performance metrics to validate improvement efforts. MTF Engagement: One-on-one support (telephone/DCO/group org box) Bi-monthly meetings (CONUS/PACAF/USAFE) conducted via DCO. Both business and training conducted. Optimize use of Vector Check. Tools/resources/announcements/schedule...eDQ. AF portion of the TMA DQ Course. Beyond the DQ statement. Site Visit philosophy. Standardized approach, exhaust other avenues first. Mission: Provide Comprehensive DQ - Program Management to all MTFs. Provide reachback support to MAJCOMs and DRUs. Key Objectives: Standardize Methodology. Evaluate Processes. Reduce Variance. Future Initiatives: Consolidation. Shape MHS/AFMS DQ efforts.")
9
Why Data Quality?

10
Data Quality Integrated Approach
MEPRS Personnel Workload Financial UBO Other Health Insurance Eligibility Demographics Coding SIDR/SADR MSDRG/RWP RVU/CPT Patient & Provider Data Quality Completeness Timeliness Accuracy

11
Why is Data Quality Important?
Monitor efficiency of the healthcare system Prospective Payment System (PPS) Base Realignment And Closure (BRAC) Medicare Eligible Retiree Health Care Fund (MERHCF) MTF Business Plans Provider/Clinic Workload Productivity Reimbursements (TPC, Coast Guard, NOAA…etc) Enable the Leadership to make informed decisions Talk about the $23.5M lost due to missing data months for MERHCF as an example For these reasons, it is vital your data accurately reflect work performed in your MTF!
 Base Realignment And Closure (BRAC) Medicare Eligible Retiree Health Care Fund (MERHCF) MTF Business Plans. Provider/Clinic Workload Productivity. Reimbursements (TPC, Coast Guard, NOAA…etc) Enable the Leadership to make informed decisions. Talk about the $23.5M lost due to missing data months for MERHCF as an example. For these reasons, it is vital your data accurately reflect work performed in your MTF!")
12
What could go wrong? WWR MDR M2 TPOCS WAM EAS IV SADR PDTS CAPER ADM
Clinical Data Mart Interface Errors Air Force TRICARE Ops Center CCQAS Worldwide Workload Report WWR (Count Visits) Service Repository (BDQAS) DoD/VA FHIE/BHIE SHARE MHS Data Repository MDR Coding Compliance Editor SADR CAPER (Encounters) CCE PDTS Pharmacy Data Transaction System ADM SADR 1/SADR 2 Standard Ambulatory Data Record Pop Health Portal EAS IV Extract With all these Systems that effect DQ, there is opportunities for failure MHS Mart M2 Essentris EAS Repository TPOCS Billable Encounters WAM Count Visits & Raw Services EAS IV “Eligible” Encounters CPT Codes Units of Service
 Service Repository (BDQAS) DoD/VA. FHIE/BHIE SHARE. MHS Data Repository. MDR. Coding Compliance. Editor. SADR. CAPER. (Encounters) CCE. PDTS. Pharmacy Data. Transaction. System. ADM. SADR 1/SADR 2. Standard Ambulatory. Data Record. Pop Health. Portal. EAS IV. Extract. With all these Systems that effect DQ, there is opportunities for failure. MHS Mart. M2. Essentris. EAS. Repository. TPOCS. Billable. Encounters. WAM. Count Visits & Raw Services. EAS IV. Eligible Encounters. CPT Codes. Units of Service.")
13
Mtf engagement

14
MTF DQ Engagement One-on-One Support
Telephone and Defense Connect Online (DCO) & optimize use of Vector Check MTF-AMFOA DQ Teleconferences Every Other Month PACAF, CONUS, USAFE (schedule on Vector Check) DCO used to conduct meetings and take attendance Business and training conducted at each meeting Site Visits AF portion of the TMA DQ Course Other Conferences/Forums Serving/supporting our MTFs occupies a large portion of our time also.
 & optimize use of Vector Check. MTF-AMFOA DQ Teleconferences Every Other Month. PACAF, CONUS, USAFE (schedule on Vector Check) DCO used to conduct meetings and take attendance. Business and training conducted at each meeting. Site Visits. AF portion of the TMA DQ Course. Other Conferences/Forums. Serving/supporting our MTFs occupies a large portion of our time also.")
15
Defense Connect Online
Link to meeting will be sent via /calendar request Share screen capability to maximize training Chat capabilities to ask questions to all or individuals To become a registered user visit:

16
Vector Check Your DQ Toolkit
Announcements Calendar Contacts FAQs Documents Electronic Data Quality Application (eDQ) Subscribe to Alerts! Vector Check is your one stop shop.
 Subscribe to Alerts! Vector Check is your one stop shop.")
17
Vector Check Gaining Access
Your Vector Check account is linked to your Knowledge Exchange (Kx) account If you don’t have a Kx account, create one at Click: If you have a Kx account, verify your address is correct (then WAIT 24 Hrs prior to signing into Vector Check). Click:
 account. If you don’t have a Kx account, create one at Click: If you have a Kx account, verify your address is correct (then WAIT 24 Hrs prior to signing into Vector Check). Click:")
18
Vector Check Gaining Access
After you have been granted a Kx account (this may take up to 24 hours), navigate to Vector Check at: The first time you visit the Vector Check site, you will be redirected to a registration page. The form will be pre- populated. Verify and submit the information.
, navigate to Vector Check at: The first time you visit the Vector Check site, you will be redirected to a registration page. The form will be pre- populated. Verify and submit the information.")
19
Vector Check Updating the RM Master Roster
Update your POC information on the RM Master Roster at: Select “New” to add a new POC, or select “Actions / Edit in Datasheet” to edit POCs. The contact information for these positions must always be kept current: MDG CC MDG Deputy CC MDSS Commander Administrator RMO RMO NCOIC DQ Manager DQ Alternate If you have any changes to these POCs, please update Vector Check. This will be the method of adding or deleting POCs from our distribution list. This will also be a roster that is used by MEPRS, UBO, Budget…

20
Vector Check Documents Training Material on VC
Review training materials posted on Vector Check “Alerts, Timeliness and Accuracy, and TUG” Pathway: Vector Check > AFMOA > SGA > SGAR > SGAR – Data Quality > Documents > Training > Administrative All DQ Review List and Statement Training Slides Pathway: Vector Check > AFMOA > SGA > SGAR > SGAR – Data Quality > Documents > Training > DQ Review List and Statement Training Slides Review the latest DQ Teleconference Notes Pathway: Vector Check > AFMOA > SGA > SGAR > SGAR – Data Quality > Documents > Data Quality Meeting Minutes- Notes

21
Guidance

22
Overview DoDI 6040.40 DQ Mgmt Control (DQMC) Procedures
DQMC Review List Data Quality Statement Annual Updates – TMA Led Recommends Data Quality Assurance Team (DQAT) Composition The DQ Review List changes every year. The Review List is a TriService product that all 3 services along with TMA review each year over a 4 month timeframe to make modifications, deletions, and additions. For FY11 we had successful compromises. You have a voice, if you would like to make any modifications, deletions, or additions please provide as feedback on any changes you would like to see made with a justification for the change. We will be glad to advocate for you.
 Composition. The DQ Review List changes every year. The Review List is a TriService product that all 3 services along with TMA review each year over a 4 month timeframe to make modifications, deletions, and additions. For FY11 we had successful compromises. You have a voice, if you would like to make any modifications, deletions, or additions please provide as feedback on any changes you would like to see made with a justification for the change. We will be glad to advocate for you.")
23
Health Services Inspection (HSI)
2012 HSI Checklist, OM.3.2.2 The Data Quality Assurance Team (DQAT) met monthly: Completed DQMC Review List Briefed Executive Committee on all Review List performance that was not compliant There was evidence corrective action plans were created, monitored and progressing to address non-compliant or underperforming DQMC items
 met monthly: Completed DQMC Review List. Briefed Executive Committee on all Review List performance that was not compliant. There was evidence corrective action plans were created, monitored and progressing to address non-compliant or underperforming DQMC items.")
24
Health Services Inspection (HSI)
2012 HSI Checklist, OM.3.2.2 Documents Required for Review: Current and past year’s DQM reports DQAT meeting minutes

25
DQ assurance Team

26
DQ Assurance Team The Data Quality Assurance Team (DQAT) or other designated structure met during the reporting month to complete the DQMC Review List. DoDI Recommended Team Composition: DQ Manager Directors of Clinical Activities MEPRS/EAS Coordinator Budget/Accounting Medical CIO Health Information Manager CHCS Administrator Group Practice Managers Patient Administration Additional team members recommended in Data Quality Team User’s Guide: Coder/coding auditor AHLTA Trainer Ancillary services representative Defense Medical Human Resources System – internet (DMHRSi) personnel (i.e., DMHRSi Manager, contract liaison, civilian liaison, volunteer liaison, and Command Support Staff (CSS) personnel) UBO Manager Clinic support staff representative Resource Management Flight CC Red indicates required members when AFI is published Red indicates required members when AFI is published
 or other designated structure met during the reporting month to complete the DQMC Review List. DoDI Recommended Team Composition: DQ Manager. Directors of Clinical Activities. MEPRS/EAS Coordinator. Budget/Accounting. Medical CIO. Health Information Manager. CHCS Administrator. Group Practice Managers. Patient Administration. Additional team members recommended in Data Quality Team User’s Guide: Coder/coding auditor. AHLTA Trainer. Ancillary services representative. Defense Medical Human Resources System – internet (DMHRSi) personnel (i.e., DMHRSi Manager, contract liaison, civilian liaison, volunteer liaison, and Command Support Staff (CSS) personnel) UBO Manager. Clinic support staff representative. Resource Management Flight CC. Red indicates required members when AFI is published. Red indicates required members when AFI is published.")
27
DQ Assurance Team Provide oversight for: Develop DQ initiatives
Provider file clean-up and maintenance TMA coding audit MEPRS ASD reconciliation DMHRSi program DD Form 2569 collection process Provide oversight for: Develop DQ initiatives Ensure there is cross-talk Recommend at your next DQ meeting, that everyone goes around the room and understands why they are a member of the team What role they have in DQ What ideas they have to make the team (ultimately your MTF) better Communication: File/Table updates, Clinic/Provider profiles Appointment standardization Proper CHCS File/Table set up Account Subset Definition (ASD) Table Reconciliation Inappropriate MEPRS Codes Assigning Workload to the Proper MEPRS/FCC Codes
 better. Communication: File/Table updates, Clinic/Provider profiles. Appointment standardization. Proper CHCS File/Table set up. Account Subset Definition (ASD) Table Reconciliation. Inappropriate MEPRS Codes. Assigning Workload to the Proper MEPRS/FCC Codes.")
28
DQ Assurance Team Initiatives - Interest Items (cont)
Verify Eligibility in DEERS Gather/Verify Demographics and OHI Patient Registration/Admissions/Front Desk Duties Documentation must record what actually occurred Ensure Accuracy/Completeness TMA Annual Coding Audit tracking Coding Patient safety CHCS Training Accountability Include critical data elements Correct critical data elements Improve data accuracy Capture workload and revenue opportunities

29
Chcs Provider file

30
CHCS Provider File Report Cards
PROCESS Eliminate CHCS Provider File error backlog and prevent future errors across AFMS ISSUES Impacts REVENUE, WORKLOAD, PATIENT SAFETY and DATA INTEGRITY Lack of expertise, ownership and guidance to resolve and prevent provider file errors ACTIONS Centrally produced MTF report cards; refined focused approach Created a library of training materials to correct backlog and prevent errors Partnered with Pharmacy community (point of entry for most external providers) to focus on prevention Conducted Focus site visits to provide training and obtain buy-in IMPACT 76% decrease in the number of Provider File errors across AFMS since Nov 09
 to focus on prevention. Conducted Focus site visits to provide training and obtain buy-in. IMPACT. 76% decrease in the number of Provider File errors across AFMS since Nov 09.")
31
Primary Effects of CHCS Provider File Errors
Revenue Patient Safety Data Integrity Workload

32
CHCS Provider File Continuity Guide
Comprehensive reference for issues related to CHCS provider file maintenance Nearing completion – release date TBD Includes step-by-step guidance to correct errors Recommendations for provider file management Includes helpful resources

33
Provider File Report Card

34
Provider Details Report
Error ID on the left; scroll to the right to view the actual field – what is actually in CHCS. Some fields are linked (ref Cont Guide).
.")
35
Outside Provider Entry Checklist
This is a checklist that your Ancillary Services can use as a quick reference tool when entering an Outside Provider into CHCS.

36
METRICS

37
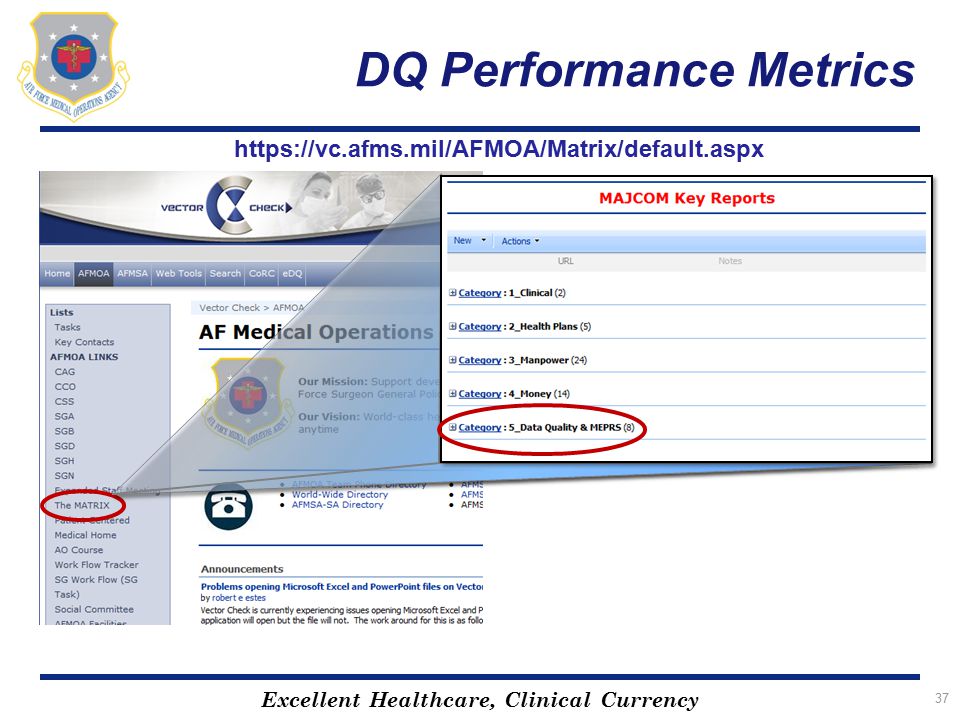
DQ Performance Metrics
38
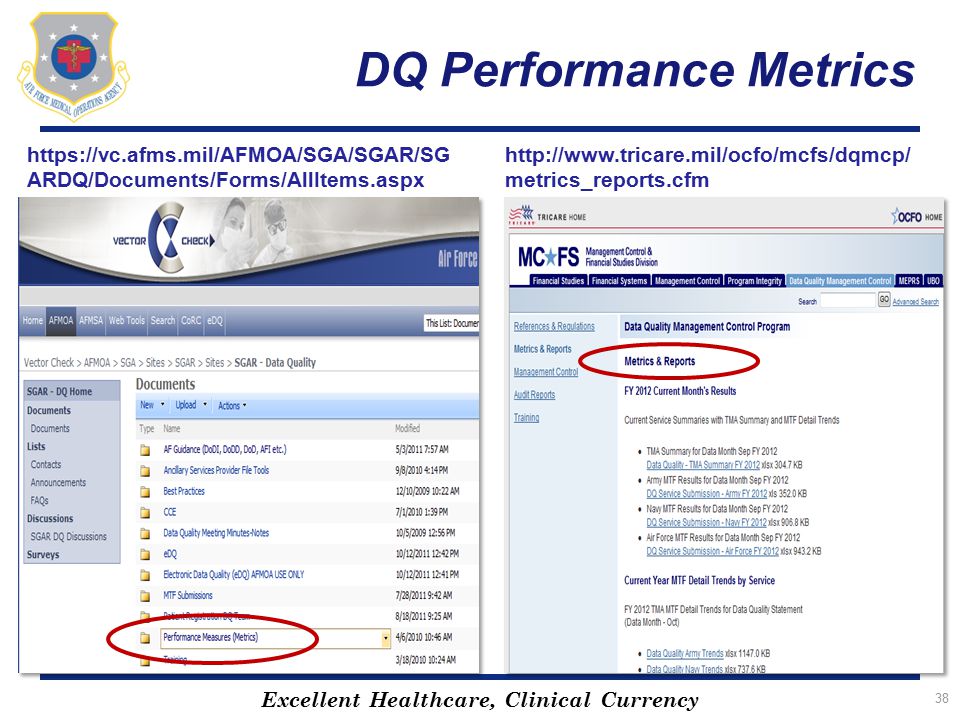
DQ Performance Metrics
39
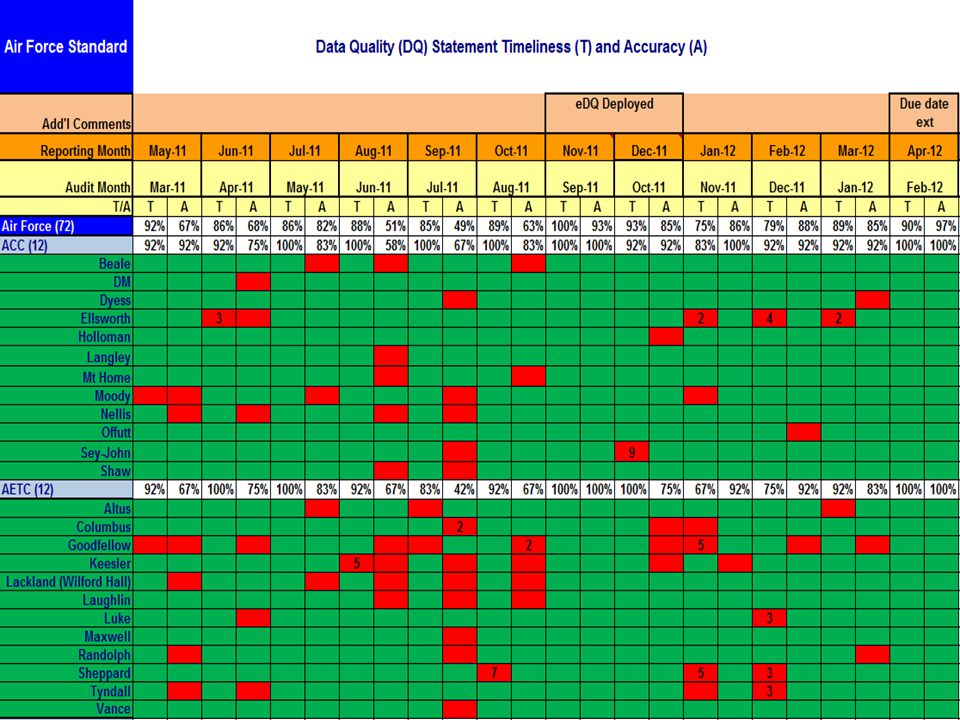
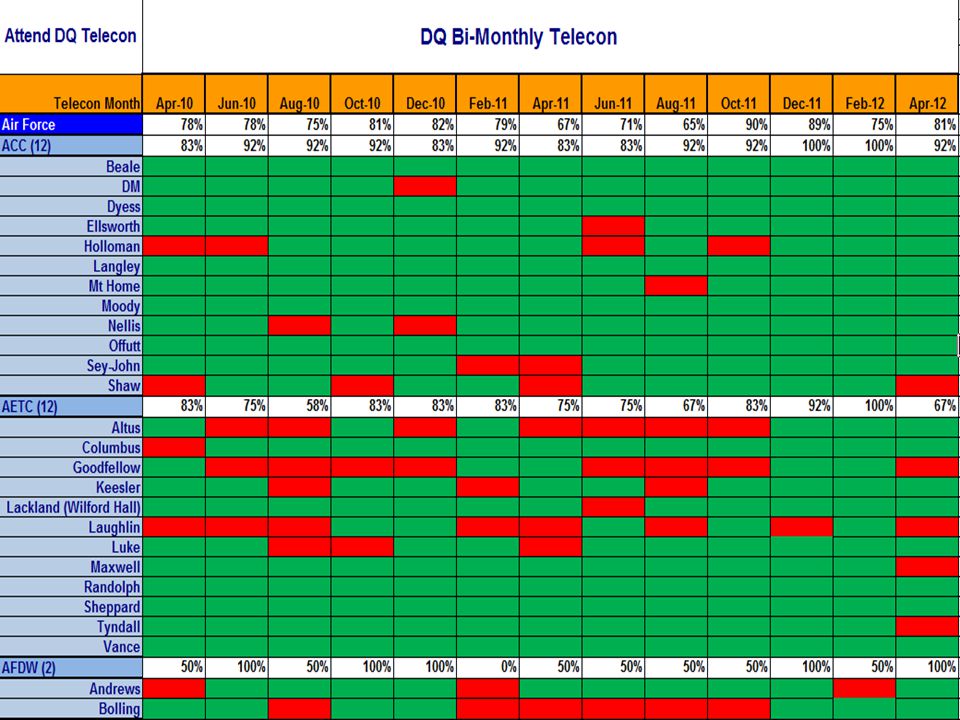
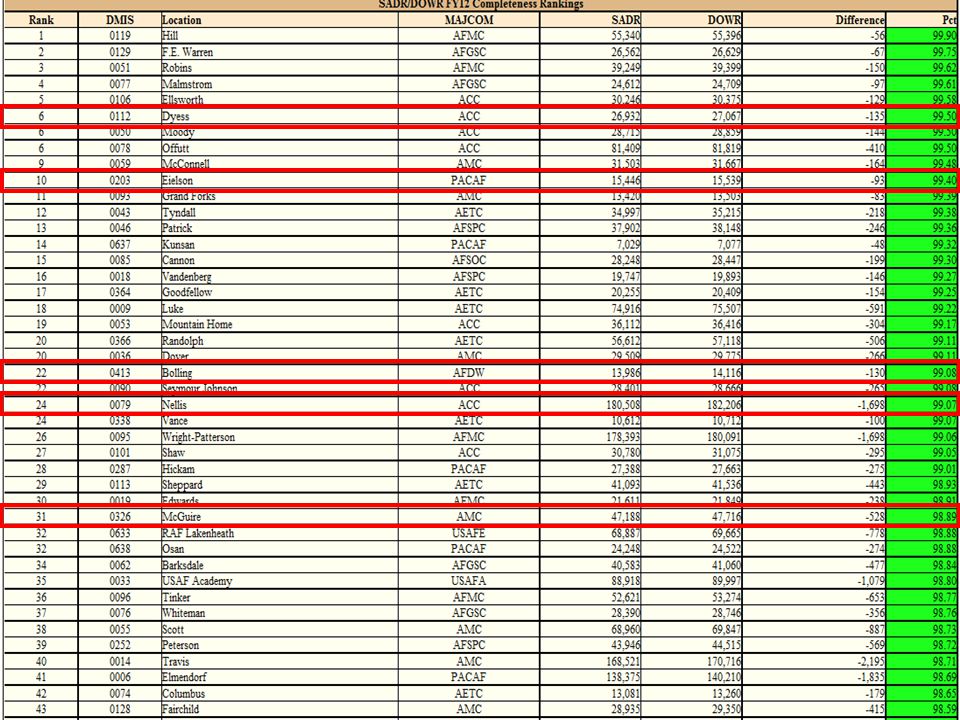
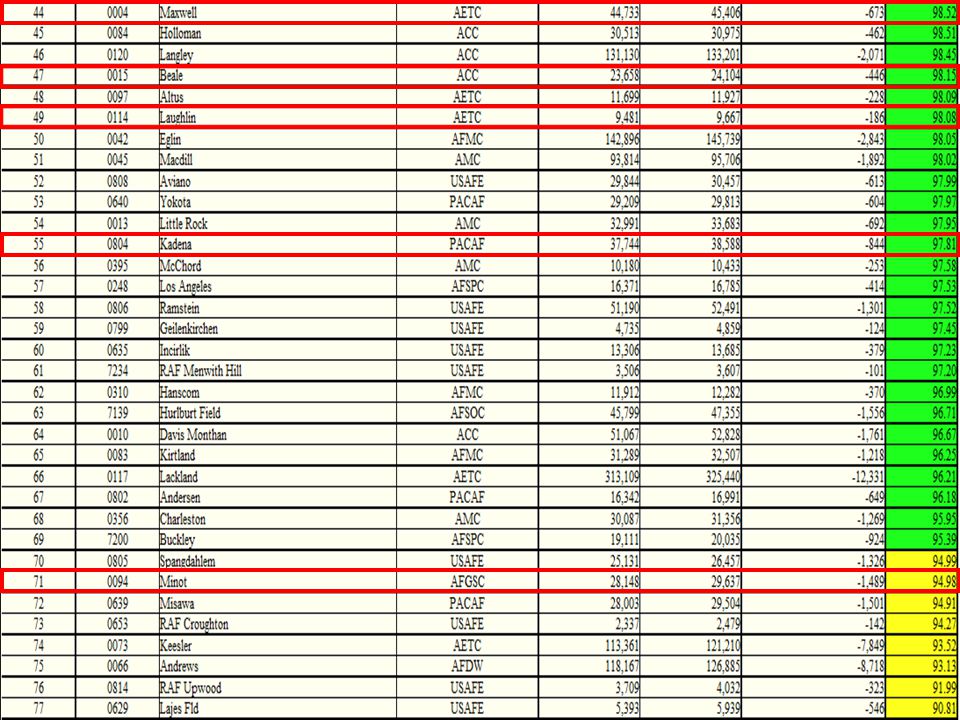
AF DQ Results

42
DQ Statement Signed by?

43
Provider File Progress Metrics

44
Workload Guidelines Sample
Encounter Activity Provider Type Provider Specialty Code MEPRS Code for Time Capture MEPRS Code for Workload Count/Non-Count Indicator Patient Encounter Business Rules Coding Required Billing Required Nutritionist/Dietitian Privileged Provider 704 – Dietician/ Nutritionist B*** Count Registered dieticians or licensed nutrition Professionals are responsible for providing medical nutrition therapy (MNT). Yes Supplements AF Coding Guidelines - Published by AF Coding Experts MHS Coding Guidelines, inpatient and outpatient, dated 1 January 2011
. Yes. Supplements AF Coding Guidelines. - Published by AF Coding Experts. MHS Coding Guidelines, inpatient and outpatient, dated 1 January")
45
Other DQ Efforts

46
Support Provided Correct CHCS patient registration errors for all Air Force MTFs Primary Care Manager Information Transfer (PIT) Errors Correct Patient Registration Errors (FY11-558K Patients) Merge CHCS Duplicate Patients Identify AHLTA Multiples and Log MHS tickets Subject Matter Expertise Support Partner with DoD to develop policies and processes to reduce patient registration errors Identify and correct systemic issues, which contribute to the duplication of clinical records and put patient safety at risk AFMS Record Reconciliation Initiative 46 46
 Merge CHCS Duplicate Patients. Identify AHLTA Multiples and Log MHS tickets. Subject Matter Expertise Support. Partner with DoD to develop policies and processes to reduce patient registration errors. Identify and correct systemic issues, which contribute to the duplication of clinical records and put patient safety at risk. AFMS Record Reconciliation Initiative")
47
Support Provided Training
Conduct Pt Reg, PIT Error, Duplicate Patient training at MTFs, Conferences, DCO Connect, etc. Phone consultations as needed Enterprise Health Data Optimization System (eHDOS) Reports Summary Reports by MAJCOM and MTFs on Vector Check Users with Registration Capability Number of New Patients Added to CHCS with Critical Errors Number of Potential CHCS Duplicate Patients Number of Patients with Patient Category Mismatches Number of PIT Errors Managed Care File/Table Concerns Affecting PIT Errors
 Reports. Summary Reports by MAJCOM and MTFs on Vector Check. Users with Registration Capability. Number of New Patients Added to CHCS with Critical Errors. Number of Potential CHCS Duplicate Patients. Number of Patients with Patient Category Mismatches. Number of PIT Errors. Managed Care File/Table Concerns Affecting PIT Errors.")
48
AFMOA Data Quality Vector Check
MTF Reports are posted to the AFMOA Data Quality Vector Check monthly Menu path: Vector Check-AFMOA-SGA-SGAR-Data Quality-Documents-Patient Registration MAJCOM_MTF Reports

49
AFMOA Vector Check-The MATRIX

50
DQ Review List/Statement guidance & completion

51
TUG Primary AF-specific DQ guidance
Clarifies questions on the DQMC Review List Includes formulas, background information, and how to get the data Available on Vector Check Share with the DQAT Discuss at your DQ meeting to ensure it is read and understood by those answering DQ statement and review list question Organization mirrors the review list Updated during the year as needed

52
TUG: Six Linked Worksheets
Click the options box and select "enable this content" Tab 1: Forward Tab 2: TUG Contents Filtered & Linked Tab 3: TUG Tab 4: TUG Appendix Tab 5: DQ Review List Tab 6: DQ Statement The FY 11 TUG consists of six linked worksheets: Forward, TUG Contents Filtered & Linked, TUG, TUG Appendix, DQ Review List, and DQ Statement. In order for each to work properly the macros will have to be activated. Each time the document is opened, in the upper left corner of the workbook there will be a Security Warning stating that "macros have been disabled" with an option box next to it. Click the options box and select "enable this content" then click ok. All the links will be activated.

53
TUG Contents The following is provided for each review list and statement question: Performance threshold Calculation (if applicable) Details (may include “step-by-step” guidance) Process Additional Information
 Details (may include step-by-step guidance) Process. Additional Information.")
54
DQ Review List/Statement Reminders
Refining/expanding beyond DQ statement…TUG Internal tool to assist in identifying & correcting financial & clinical workload data problems DQMC Review List requires all supporting summary documentation kept on file for 5 years Monthly Requirement All variances on the REVIEW LIST should be briefed with DQ Team and Executive Committee MTFs need back up plans for Data Quality and all other areas that support completing the Review List eDQ is based on the Review List

55
25th DQ Statement Due Date Aggressive follow up if late:
Day One – Notify RMO Day Two – Notify MDSS/CC Day Three – Notify MDG/CC DUE THE LAST DUTY DAY OF THE MONTH

56
DQ Review List Comments
Evaluate all comments non-compliant Review comments to ensure complete and concise Problem, corrective action plan, ECD required Do not use “I”, “AFMOA”, “John Doe”, etc… Do use functional area, ie. DQ Manager, Coding Auditor, AFMOA Coding… If stating contractor, system or AFMOA has impacted a metric negatively, require back up documentation These comments will be validated before approved Review comments with Contracting Officer Representative (COR) (if comment provided by contractor) for comments requiring further clarification Comments included on your MTF Statement are posted word for word on TMA and vector check websites
 (if comment provided by contractor) for comments requiring further clarification. Comments included on your MTF Statement are posted word for word on TMA and vector check websites.")
57
DQ Review List DQ Assurance Team Meeting
Question A.3: The DQ Assurance Team or other designated structure met during the month to complete the DQ Management Control Review List (recommend attaching meeting minutes) Date Completed: __________ Data Month: ______________ Yes No (comment required) N/A (not appropriate for this question)
 Date Completed: __________. Data Month: ______________. Yes. No. (comment required) N/A. (not appropriate for this question)")
58
DQ Review List DQ Assurance Team Meeting
Question A.4: The DQ Manager briefed last month’s Data Quality Management Control Review List, and Financial and Workload Data Reconciliation and Validation results to the MTF Executive Committee Yes No (comment required) N/A (not appropriate for this question)
 N/A. (not appropriate for this question)")
59
DQ Review List TMA DQ Course
Question A.7a: TMA Data Quality Course (DQ Manager in the last three years)? Recommend using the A.7 a-c to highlight training needs to your MTFs leadership Yes No (comment required) N/A (not appropriate for this question)
 Recommend using the A.7 a-c to highlight training needs to your MTFs leadership. Yes. No. (comment required) N/A. (not appropriate for this question)")
60
DQ Review List Negative Findings
Question A.8: Was there evidence in meeting minutes or other sources of corrective plans, of appropriate resourcing and actions to follow-up on the previous month's negative findings? Yes No (comment required) N/A (not appropriate for this question)
 N/A. (not appropriate for this question)")
61
DQ Review List Rejected Data
Question B.4: Were all rejected data corrected and retransmitted? (As applicable.) a) ADM - ADM SADR CAPER Error Report b) AHLTA - AHLTA ADM Exceptions Report c) CCE - ADM SADR/TPOCS Extract Status Display & CCE Interface Error Report d) CHCS - PIT Errors e) DMHRSi % Timecards approved? g) MEPRS (EAS) - Error Correction Unit h) TPOCS – File Upload Status Report Yes No (comment required) N/A (Only use when no rejected data needed to be corrected or retransmitted)
 a) ADM - ADM SADR CAPER Error Report. b) AHLTA - AHLTA ADM Exceptions Report. c) CCE - ADM SADR/TPOCS Extract Status Display & CCE Interface Error Report. d) CHCS - PIT Errors. e) DMHRSi - 100% Timecards approved g) MEPRS (EAS) - Error Correction Unit. h) TPOCS – File Upload Status Report. Yes. No. (comment required) N/A. (Only use when no rejected data needed to be corrected or retransmitted)")
62
DQ Review List/Statement End of Day
Question B.5.a. (DQ Statement question 1a): In the reporting month (include only B*** and FBN* accounts): a) What percentage of appointments were closed in meeting your “End of Day” processing requirements, “Every appointment – Every day?” Source: BDQAS Number of closed CHCS appointments Total CHCS appointments for the month ≥ 97% ≥ 80% but < 97% (comment required) < 80% (comment required)
: In the reporting month (include only B*** and FBN* accounts): a) What percentage of appointments were closed in meeting your End of Day processing requirements, Every appointment – Every day Source: BDQAS. Number of closed CHCS appointments. Total CHCS appointments for the month. ≥ 97% ≥ 80% but < 97% (comment required) < 80% (comment required)")
63
BDQAS Biometric Data Quality Assurance Service (BDQAS) is a source for many DQ statement questions ( Updated on the 10th or 11th for non-EAS data EAS data on BDQAS is updated between the 16th and 20th If EAS transmission did not occur on-time, questions that are applicable to EAS must be manually calculated and annotated on the review list

64
BDQAS Metrics you can drill down to clinic level and get AFMS rankings
DQ Review List / Statement Report data is found here:

67
DQ Review List Monthly Statistical Report
Question B.5.c: Were all workload discrepancies on the CHCS Monthly Statistical Report corrected prior to processing the WWR and WAM files? MINI_CAPER_DQ adhoc – Use frequently throughout the month to encourage correcting workload in a timely manner Yes No (comment required) N/A (not appropriate for this question)
 N/A. (not appropriate for this question)")
68
MINI CAPER DQ REPORT Designed to help Medical Treatment Facilities (MTFs) identify and correct patient appointment workload discrepancies prior to running the MSR Some examples on how to utilize report: Appts Closed at EOD (B.5.a) Workload Count By Provider Type (B.5.c) Ensuring Providers Sign T-cons and Encounters on Time (B.6.a) Determining whether the “ADMIN” status is properly utilized (B.5.d) Report generates a significant amount of appointment data, it can also be used for statistical analysis.
 identify and correct patient appointment workload discrepancies prior to running the MSR. Some examples on how to utilize report: Appts Closed at EOD (B.5.a) Workload Count By Provider Type (B.5.c) Ensuring Providers Sign T-cons and Encounters on Time (B.6.a) Determining whether the ADMIN status is properly utilized (B.5.d) Report generates a significant amount of appointment data, it can also be used for statistical analysis.")
69
DQ Review List ADMIN Closed
Question B.5.d: Do you have a process or policy in place to ensure the appropriate use of using "admin" when closing encounters in CHCS? NOTE: Administratively closing an appointment is as if the appointment never existed. "Admin" should be used for one of the following reasons: Training and Testing purposes Duplicate encounters Appointment created in error # of admin closed appointments: ______ Yes No (comment required) N/A (not appropriate for this question)
 N/A. (not appropriate for this question)")
70
DQ Review List/Statement Outpatient Timeliness
Question B.6.a (DQ Statement question 2a): What percentage of Outpatient Encounters, other than APVs, has been coded within 3 business days of the encounter? Source: BDQAS Nurses and Techs with “count” encounters will negatively impact metric; FY12 data has 32K encounters with incorrect workload Sum of Non-APV CAPER Encounters Coded W/in 3 Business Days Sum of Non-APV Daily Outpatient Workload Reports (DOWR) ≥ 95% ≥ 80% but < 95% (comment required) < 80% (comment required)
: What percentage of Outpatient Encounters, other than APVs, has been coded within 3 business days of the encounter Source: BDQAS. Nurses and Techs with count encounters will negatively impact metric; FY12 data has 32K encounters with incorrect workload. Sum of Non-APV CAPER Encounters Coded W/in 3 Business Days. Sum of Non-APV Daily Outpatient Workload Reports (DOWR) ≥ 95% ≥ 80% but < 95% (comment required) < 80% (comment required)")
71
DQ Review List/Statement APV Timeliness
Question B.6.b (DQ Statement question 2b): What percentage of APVs have been coded within 15 days of the encounter? Source: BDQAS If non-compliant, a time study is required each month until compliant Where are your delays? Transcription Records Provider Coder Sum of APV CAPER Encounters Coded W/in 15 Calendar Days Sum of APV Daily Outpatient Workload Reports (DOWR) Sum of APV CAPERs Coded W/in 15 Calendar Days Sum of APV DOWR ≥ 95% ≥ 80% but < 95% (comment required) < 80% (comment required)
: What percentage of APVs have been coded within 15 days of the encounter Source: BDQAS. If non-compliant, a time study is required each month until compliant. Where are your delays Transcription. Records. Provider. Coder. Sum of APV CAPER Encounters Coded W/in 15 Calendar Days. Sum of APV Daily Outpatient Workload Reports (DOWR) Sum of APV CAPERs Coded W/in 15 Calendar Days. Sum of APV DOWR ≥ 95% ≥ 80% but < 95% (comment required) < 80% (comment required)")
72
DQ Review List/Statement Inpatient Timeliness
Question B.6.c (DQ Statement question 2c): What percentage of Inpatient records have been coded within 30 days after discharge? Source: Run “Inpatient Timeliness” ad hoc found on BDQAS If the MTF lacks a coder, the numerator will be “0” and the denominator will be taken from the WWR Total Dispositions Total # of Records Coded WWR Total Dispositions Total # of Records Coded WWR Total Dispositions ≥ 95% ≥ 80% but < 95% (comment required) < 80% (comment required)
: What percentage of Inpatient records have been coded within 30 days after discharge Source: Run Inpatient Timeliness ad hoc found on BDQAS. If the MTF lacks a coder, the numerator will be 0 and the denominator will be taken from the WWR Total Dispositions. Total # of Records Coded. WWR Total Dispositions. Total # of Records Coded. WWR Total Dispositions. ≥ 95% ≥ 80% but < 95% (comment required) < 80% (comment required)")
73
DQ Review List CCE B.7.a: What percentage of encounters had an encounter coding status of “Completed” for the data month? Source: CCE Denominator This question measures CCE utilization. Due to the AF coding model, AF MTFs will have a low percentage for this question. Numerator ≥ 95% ≥ 80% but < 95% (comment required) < 80% (comment required)
 < 80% (comment required)")
74
DQ Review List/Statement Reconciliation
Question C.1.a (DQ Statement question 3a): Was the monthly MEPRS (EAS) financial reconciliation process completed, validated and approved by the MTF Resource Manager (i.e., AF Budget Officer or Analyst prior to MEPRS monthly transmission? Source: MEPRS Manager and RMO Office EAS Transmission does not impact this question. . Yes No (comment required) N/A (not appropriate for this question)
: Was the monthly MEPRS (EAS) financial reconciliation process completed, validated and approved by the MTF Resource Manager (i.e., AF Budget Officer or Analyst prior to MEPRS monthly transmission Source: MEPRS Manager and RMO Office. EAS Transmission does not impact this question. . Yes. No. (comment required) N/A. (not appropriate for this question)")
75
DQ Review List/Statement Reconciliation
Question C.1.b: Has the MTF used the Workload Generation Controller (WGC) in CHCS to generate their WWR and WAM files? Source: MEPRS Manager WGC process is an 11 step process . Yes No (comment required) N/A (not appropriate for this question)
 in CHCS to generate their WWR and WAM files Source: MEPRS Manager. WGC process is an 11 step process. . Yes. No. (comment required) N/A. (not appropriate for this question)")
76
DQ Review List/Statement MEWACS
C.1.d. (DQ Statement question 3b): Were the data load status, outlier/variance, WWR-EAS IV, and allocations tabs in the current MEWACS document reviewed and explanations provided for flagged data anomalies? Source: MEPRS Manager C.1.d.1 through C.1.d.4 must be answered If you reviewed tabs on MEWACS, C.1.d.1 - C.1.d.4, regardless of anomalies, ANSWER YES Yes No (comment required) N/A (not appropriate for this question)
: Were the data load status, outlier/variance, WWR-EAS IV, and allocations tabs in the current MEWACS document reviewed and explanations provided for flagged data anomalies Source: MEPRS Manager. C.1.d.1 through C.1.d.4 must be answered. If you reviewed tabs on MEWACS, C.1.d.1 - C.1.d.4, regardless of anomalies, ANSWER YES. Yes. No. (comment required) N/A. (not appropriate for this question)")
77
MEWACS: Will be required to register to access

78
Select: Data Load Status Summary Outliers WWR/EAS IV Outliers Allocation Test

79
AFMOA MEPRS Dashboard Launched MEPRS Dashboard Oct 2009 Objectives:
Identify variance Evaluate processes Provide training Measures: 20 Key data points with supporting detailed reports Controls: 1 or 2 standard deviations Upper-Lower controls Visibility: Resides on Vector Check – Enterprise-Wide Access Data Source: EASIV 79 79

80
AFMOA MEPRS Dashboard Nellis AFB, Nov 2009
Validated Error Error Error Research Error Error Data Source: EASIV Errors 80 80

81
AFMOA MEPRS Dashboard Nellis AFB, Apr 2010
Corrected Corrected Validated Corrected Research Research Corrected Corrected Data Source: EASIV Corrections Pending 81 81

82
DQ Review List/Statement Timecards
C.1.f. (DQ Statement question 3c): For DMHRSi, what is the percentage of submitted timecards by the suspense date? Number of Timecards Submitted On-time Total Number of Timecards for an MTF C.1.g (DQ Statement question 3d): For DMHRSi, what is the percentage of approved timecards by the suspense date? Number of Timecards Approved On-time Total Number of Timecards for an MTF Source is MEPRS Manager =100% < 100% (comment required)
: For DMHRSi, what is the percentage of submitted timecards by the suspense date Number of Timecards Submitted On-time. Total Number of Timecards for an MTF. C.1.g (DQ Statement question 3d): For DMHRSi, what is the percentage of approved timecards by the suspense date Number of Timecards Approved On-time. Total Number of Timecards for an MTF. Source is MEPRS Manager. =100% < 100% (comment required)")
83
DQ Review List/Statement Timecards
C.1.f. (DQ Statement question 3c) For DMHRSi, what is the percentage of submitted timecards by the suspense date? Source is MEPRS Manager? C.1.g. (DQ Statement question 3d) For DMHRSi, what is the percentage of approved timecards by the suspense date? Source is MEPRS Manager Remember, comments are required if under 100% Number of Timecards Submitted On-time 315 320 Total Number of Timecards for an MTF Denominators (bottom numbers) should be the same Remove the following statuses NULL NOT SUBMITTED REJECTED WORKING Remove all personnel who did not work during pay period Number of Timecards Approved On-time 310 320 Total Number of Timecards for an MTF Cannot be greater than C.1.e. Remove the following statuses NULL NOT SUBMITTED REJECTED WORKING SUBMITTED Remove all personnel who did not work during pay period Not only about submission, but also approval If the percentage you have here is less than the submitted percentage, then you need to explain what is the problem with the approval process This percentage is not calculated by the percentage of timecards approved that were submitted. This percentage is calculated out of the entire number of timecards that should have been submitted. If a personnel retires, separates, PCS’s, or no longer works at your MTF, they can be removed from the calculation as long as they did not work during a pay period.
 For DMHRSi, what is the percentage of submitted timecards by the suspense date Source is MEPRS Manager C.1.g. (DQ Statement question 3d) For DMHRSi, what is the percentage of approved timecards by the suspense date Source is MEPRS Manager. Remember, comments are required if under 100% Number of Timecards Submitted On-time Total Number of Timecards for an MTF. Denominators (bottom numbers) should be the same. Remove the following statuses. NULL. NOT SUBMITTED. REJECTED. WORKING. Remove all personnel who did not work during pay period. Number of Timecards Approved On-time Total Number of Timecards for an MTF. Cannot be greater than C.1.e. Remove the following statuses. NULL. NOT SUBMITTED. REJECTED. WORKING. SUBMITTED. Remove all personnel who did not work during pay period. Not only about submission, but also approval. If the percentage you have here is less than the submitted percentage, then you need to explain what is the problem with the approval process. This percentage is not calculated by the percentage of timecards approved that were submitted. This percentage is calculated out of the entire number of timecards that should have been submitted. If a personnel retires, separates, PCS’s, or no longer works at your MTF, they can be removed from the calculation as long as they did not work during a pay period.")
84
DQ Review List/Statement Timecards
Timecard compliance and EAS transmission DQ Statements due to AFMOA Pay period ends Member PCS’d Timeliness Timecard submission Timeliness Timecard approval Rejected timecards corrected

85
DQ Review List/Statement Timecards
Timecard compliance and EAS transmission Pay period ends Timeliness Timecard submission Timeliness Timecard approval Rejected timecards corrected DQ Statements due to AFMOA

86
DQ Review List/Statement CHCS Duplicate Patients
Question C.2. a. (DQ Statement question 10) Use CHCS during the data month to identify duplicate patient registration. For CHCS or AHLTA hosts only, what was the number of potential duplicate patient registration in the data month for all MTFs under the host? (NOTE: Only Host sites report up.) Source is Internal Process Run the CHCS standard report – “Potential Duplicate Patient Search” Report Ran Report Not Ran (comment required) If you are not a host site, LEAVE BLANK
 Use CHCS during the data month to identify duplicate patient registration. For CHCS or AHLTA hosts only, what was the number of potential duplicate patient registration in the data month for all MTFs under the host (NOTE: Only Host sites report up.) Source is Internal Process. Run the CHCS standard report – Potential Duplicate Patient Search Report Ran. Report Not Ran. (comment required) If you are not a host site, LEAVE BLANK.")
87
DQ Review List/Statement CHCS Duplicate Patients
Run Time Statistical Report Validate the accuracy of the potential duplicate patients being reported Provide Summary Documentation (5 year requirement) Detailed Results w/out Protected Health Information (PHI) Identifies if Potential Duplicate’s are resolved The sum of these 4 columns is the potential duplicate number reported on the DQ Statement 87
 Detailed Results w/out Protected Health Information (PHI) Identifies if Potential Duplicate’s are resolved. The sum of these 4 columns is the potential duplicate number reported on the DQ Statement. 87.")
88
DQ Review List/Statement CHCS Duplicate Patients
Total # of potential duplicate patients Must add up to the total listed above Pre-populated with DMIS ID(s) and MTF(s) associated with host site
 and MTF(s) associated with host site.")
89
DQ Review List/Statement CHCS Duplicate Patients
Potential Duplicate Report Run Time Statistical Report Run the Registration report Run for the entire data month Run this report no earlier than the first day after the data month Identify, Exclude, and/or Merge potential duplicates Provide DQ Manager the potential duplicate number(s) by unresolved, identified, excluded, and merged Use this report as summary documentation Provides results of the Potential Duplicate Report Run this report for the first day after the data month to present This report captures WHEN the potential duplicate report was ran and the results The numbers in the unresolved, identified, excluded, and merged columns are all to be reported on the DQMC Review List & Statement
 by unresolved, identified, excluded, and merged. Use this report as summary documentation. Provides results of the Potential Duplicate Report. Run this report for the first day after the data month to present. This report captures WHEN the potential duplicate report was ran and the results. The numbers in the unresolved, identified, excluded, and merged columns are all to be reported on the DQMC Review List & Statement.")
90
Patient Duplicate Reporting
DISCLAIMER: We know this is not catching all duplicate patients. Do not use this to gauge the health of your patient file on your CHCS platform. Would recommend on occasion running the “ALL” report and Registration report. However, for DQ reporting purposes, the Registration report number is what should be on the Statement. Just because DQ is asking for the Potential Duplicate Patient Report, does not exclude a facility from running the required monthly PIT Error Discrepancy Report and working them separately. Two different requirements and two different problems. Might see some crossover that the same patient’s are on both reports, but this is normal

91
DQ Review List/Statement EAS Transmission
Question C.3.a (DQ Statement question 4a): MEPRS/EAS (45 days) Source: MEPRS Manager EAS transmission should not occur until 100% timecard compliance is achieved, per AF/SG policy letter Yes No (comment required) N/A (not appropriate for this question)
: MEPRS/EAS (45 days) Source: MEPRS Manager. EAS transmission should not occur until 100% timecard compliance is achieved, per AF/SG policy letter. Yes. No. (comment required) N/A. (not appropriate for this question)")
92
MEPRS Transmission (C.3.a)
Request summary documentation of timely submission is generated when MEPRS Transmission occurred Ensure transmission occurred on or before the 45th calendar day after the data month When reviewing BDQAS data, if the numerator for C.9.c is not available, MEPRS Transmission was not timely

93
DQ Review List ADM SADR/CAPER Errors
Question C.4.a: Check the ADM SADR/CAPER Error Report? Question C.4.b: Correct the errors listed on the report? Yes No (comment required) N/A (not appropriate for this question)
 N/A. (not appropriate for this question)")
94
DQ Review List/Statement Coding Accuracy Calculation
[p1]#134, 135, 136 *Note[p1] : The denominator for all categories should include codes identified by the auditor. DQ Review List/Statement Coding Accuracy Calculation The Service Headquarters will determine the specific random sample to be audited. Use the following formulas for: Q5b-d (Internal Process) 6b-d (Audit Tool) 7b-c (Audit Tool) ICD-9: # of correct ICD-9 codes Total # of ICD-9 codes E&M: # of correct E&M codes Total # of E&M codes CPT: # of correct CPT codes Total # of CPT codes Question 5 is for inpatient services, 6 is for outpatient services, and 7 is for APV services Coding accuracy *Note: The denominator for all categories should include codes identified by the auditor. *Note: If your MTF doe not have a coder; the numerator will be 0 and the denominator will be 30
 6b-d (Audit Tool) 7b-c (Audit Tool) ICD-9: # of correct ICD-9 codes. Total # of ICD-9 codes. E&M: # of correct E&M codes. Total # of E&M codes. CPT: # of correct CPT codes. Total # of CPT codes. Question 5 is for inpatient services, 6 is for outpatient services, and 7 is for APV services. Coding accuracy. *Note: The denominator for all categories should include codes identified by the auditor. *Note: If your MTF doe not have a coder; the numerator will be 0 and the denominator will be 30.")
95
Inpatient Coding/Rounds
Must audit a minimum of 30 records Question # Numerator Denominator % 5a (MS-DRG) Medical Severity Diagnosis Related Group 30 100% 5b (E&M) Evaluation & Management 29 97% 5c (ICD-9) Diagnosis 25 5d (CPT) Procedure 35 40 88% MS-DRG and E&M denominators must Expect ICD-9 codes to be higher No good indicator for CPT
 Medical Severity Diagnosis Related Group % 5b (E&M) Evaluation & Management % 5c (ICD-9) Diagnosis d (CPT) Procedure % MS-DRG and E&M denominators must. Expect ICD-9 codes to be higher. No good indicator for CPT.")
96
Availability (Outpt/APV)
If the documentation is available; however, the patient’s outpatient health record is not available, the “record of the encounter” is available for audit Calculated from the records audited by coding auditor Availability and E&M denominators should match or be close Expect ICD-9 codes to be higher than E&M No good indicator for CPT

97
DQ Review List/Statement DD Form 2569 Availability
Question C.8. (DQ Statement questions 8a (Inpatient), 8c (Outpatient), 8e (APVs)): What percentage of completed and current (signed within the past 12 months) DD Form 2569s (TPC Insurance Info) are available for audit? Source: UBO Manager Number of Complete and Current DD Form 2569s Available Number of Non-Active Duty Records available from Audit N/A; C.8.a) Only if outpatient facility C.8.c) not appropriate for this question C.8.e) If outpatient facility with the exception of Lackland, Andrews, Academy and Incirlik If you do not have a coding auditor, an alternate method is provided in the TUG ≥ 95% ≥ 80% but < 95% (comment required) < 80% (comment required)
, 8c (Outpatient), 8e (APVs)): What percentage of completed and current (signed within the past 12 months) DD Form 2569s (TPC Insurance Info) are available for audit Source: UBO Manager. Number of Complete and Current DD Form 2569s Available. Number of Non-Active Duty Records available from Audit. N/A; C.8.a) Only if outpatient facility. C.8.c) not appropriate for this question. C.8.e) If outpatient facility with the exception of Lackland, Andrews, Academy and Incirlik. If you do not have a coding auditor, an alternate method is provided in the TUG. ≥ 95% ≥ 80% but < 95% (comment required) < 80% (comment required)")
98
Roles and Responsibilities 2569 Pull List/Audit
Coding Auditor - COPY and PASTE the encounters from CARS then paste in a word document in a landscape format UBO Manager - Exclude all the active duty member’s and audit ALL non-active duty members Do not alter list Auditing only 30 is not acceptable DQ Manager - Provide a listing of non-active duty members to UBO Manager using alternate method only when there is not a coding auditor

99
2569 DQ Review List/Statement Questions
C.8.c. What percentage of completed and current (signed within the past 12 months) DD Form 2569s (TPC Insurance Info) is available for audit (non-active duty encounters only)? C.8.d. What percentage of available, current and complete DD Form 2569s is verified to be correct in the Patient Insurance Information (PII) module in CHCS? Number of complete and Current DD Form 2569s Available 95 100 Number of Non-Active Duty Non-APV Records Available from Audit Searching for a patients 2569 information in Mini Registration is incorrect and should not be used to conduct the audit Number of DD Form 2569s Correct in PII Module in CHCS 93 95 Number of Available, Current and Complete Non Active Duty DD Form 2569s available from the Outpatient – Non APV 2569 Audit The numerator in C.8.c. becomes your denominator in question C.8.d.
 DD Form 2569s (TPC Insurance Info) is available for audit (non-active duty encounters only) C.8.d. What percentage of available, current and complete DD Form 2569s is verified to be correct in the Patient Insurance Information (PII) module in CHCS Number of complete and Current DD Form 2569s Available Number of Non-Active Duty Non-APV Records Available from Audit. Searching for a patients 2569 information in Mini Registration is incorrect and should not be used to conduct the audit. Number of DD Form 2569s Correct in PII Module in CHCS Number of Available, Current and Complete Non Active Duty DD Form 2569s available from the Outpatient – Non APV 2569 Audit. The numerator in C.8.c. becomes your denominator in question C.8.d.")
100
DQ Review List/Statement Workload
C.9.c. (DQ Statement question 9c): Comparison of reported workload data. Number of MEPRS visits Number of Kept Appts (count only) Source: BDQAS If EAS was not transmitted on-time, manually calculate numerator ≥ 95% ≥ 80% but ≤ 95% or ≥ 105% (comment required) < 80% (comment required)
: Comparison of reported workload data. Number of MEPRS visits. Number of Kept Appts (count only) Source: BDQAS. If EAS was not transmitted on-time, manually calculate numerator. ≥ 95% ≥ 80% but ≤ 95% or. ≥ 105% (comment required) < 80% (comment required)")
101
DQ Review List/Statement Rounds
Question C.5.f-h (DQ Statement questions 5b-d): Coding Accuracy of Rounds Question C.9.e (DQ Statement question 9e): Comparison of reported workload data Source: M2 and WWR Number of “A***” CAPERS completed by attending provider or service (FCC=A***) Number of Sum WWR (Bed Days + Bassinet Days + Dispositions) C.9.e. N/A if outpatient only Questions C.5.f-h ≥ 95% ≥ 80% but < 95% < 80% Question C.9.e ≥ 80% ≥ 110% < 80%
: Coding Accuracy of Rounds. Question C.9.e (DQ Statement question 9e): Comparison of reported workload data. Source: M2 and WWR. Number of A*** CAPERS completed by attending provider or service (FCC=A***) Number of Sum WWR. (Bed Days + Bassinet Days + Dispositions) C.9.e. N/A if outpatient only. Questions C.5.f-h. ≥ 95% ≥ 80% but < 95% < 80% Question C.9.e. ≥ 80% ≥ 110% < 80%")
102
Rounding Per AF DQ TUG: Percentages must be reported to one decimal point. Rounding of actual performance calculations beyond one decimal point is prohibited. This means if percentage is 94.9% for the questions where compliance is 95%, a comment will be required and question is non-compliant

103
Edq

104
eDQ Documents Vector Check URL: https://vc.afms.mil
If you are the Data Quality Manager for your MTF, visit the AFMOA Data Quality Vector Check page, select “documents” then “eDQ” and download the eDQ Commander Role Bullet Background Paper. Share this file with your commander if they are new to eDQ. Also consider downloading the “eDQ User’s Manual” for future reference. Vector Check URL:

105
eDQ Documents …the eDQ Commander Role Bullet Background Paper. Share this file with your commander if they are new to eDQ. Also consider downloading the “eDQ User’s Manual” for future reference. Lastly, there is a test plan that provides detailed information on each question on the Review List

106
eDQ Availability Start collecting supporting documentation and data collection prior to eDQ availability so data input is all that is needed in eDQ eDQ will typically be available 2 days after the MEPRS transmission (approximately 17th) DQ Statements need to be signed by the Commander NLT the last duty day of the month
 DQ Statements need to be signed by the Commander NLT the last duty day of the month.")
107
Comments & Space Limitations
Limited to 1,000 Characters The Point of Contact boxes at the top of every Section page allow the user to input the appropriate POC’s information for that Section page. The maximum length of these boxes is 250 characters. Comment boxes are provided at the bottom of most questions to allow for free-text input. There are also comment boxes provided at the bottom of every Section page. These comment boxes allow for 1,000 characters per box. If a comment exceeds the viewable area, scroll boxes will automatically appear to allow the user to see the comment. If a comment is longer than 1,000 characters, a validation error will occur unless the user saves and exits eDQ without validating. It the user exits eDQ without validating, the comment will be automatically truncated to 1,000 characters and user will not see a validation error. Limited to 1,000 Characters Limited to 1,000 Characters

108
Take Aways Data Quality is much more than the DQ Statement END OF DAY
ANALYSIS OF DATA DMHRSi ENGAGED DQ TEAM PROVIDER FILE ASD RECONCILIATION 2569 COLLECTION APPT STANDARDIZATION BUSINESS PLANS CODING CAPERS ADM END OF DAY Data must be: Front-end processes are CRITICAL to back-end success Culture Comments….here (i.e. read/research/back-up plans/engaged) AND MUCH, MUCH MORE!
 AND MUCH, MUCH MORE!")
109
AFMOA DQ Point of Contacts
Group Box:

110
Summary Organization Why Data Quality? MTF Engagement Guidance
DQ Assurance Team CHCS Provider File Metrics Other DQ Efforts DQ Review List/Statement Guidance & Completion eDQ

111
Data Quality Program Office
Questions?

Similar presentations


 Program>")
-384-1608>")

 DQMCP Conference Navy Breakout.>")





 Program DQMC Program Review List for FY 2012.>")







