Download presentation
Presentation is loading. Please wait.

1
Bronchiolitis Obliterans Organizing Pneumonia

2
History 68 y female admitted to H6 X smoker 4y 40 pack Unresolving respiratory symptoms since Jan/04 Cough, SOB, Fever since Jan/04 Cough, SOB, Fever

3
History SOBE on minimal exertion Cough with minimal sputum Fever low grade & occasional night sweating SR: wt loss 10 lb, bilateral lower costal pain No orthopnea, PND,wheeze

4
History NO GI, Renal, CTD symptoms PMH: HTN & Hypothyroidism Rx: HCTZ, L Thyroxine PSH& FH –ve

5
History Office job, No travel & No pets Had received multiple Abx without significant improvement

6
Examinations Afebrile RR 18 Sat95% BP 130/70 HR 90 No clubbing, LN, Skin rash Chest : tender lower ribs minimal crackles & wheeze bilateral minimal crackles & wheeze bilateral CVS : S1+S2+0 Abd & LL N

7
Investigation WBC 12 Poly 10.8 Lymph0.7 Hb 99 MCV N Coagulation N BUN, Creat, Lytes & LFT N UA & microscopy N

8
Investigation ESR 99 ABG PH 7.46 PAO2 66 Sat 93% PCO2 38 HCO3 26.8 PCO2 38 HCO3 26.8 CXR & CT Chest PFT

9
Investigation BAL -ve cultures & cytology ANA, Anti DNA, RF & ANCA -ve Bone Scan single non specific uptake focus ?fracture Open Lung Bx RML & RLL

10
Open Lung Bx BOOP

13
BOOP Multiple etiologies Extensive proliferation of granulation tissue in the small airways Inflammation of the surrounding alveoli Incidence 6 /100,000 hospital admission

14
BOOP Equal male : female 5 th -6 th decades Smoking is not a risk factor Mimicker of CAP Symptoms, Signs, Radiological & Laboratory findings are not specific Good response to steroids

15
Etiologies Idiopathic Post Infectious Atypical,Viral,PCP, Malaria Drug Abx, Chemo, Gold,Amiodarone CTD SLE, Rheumatoid,PM, Sjogren

16
Etiologies Organ transplantation BMT,Renal, Lung Radiotherapy Autoimmune diseases PBS, IBD,Thyroditis Environmental textile printing dye

17
?Steroid Response Higher vasculrization Higher levels of VEGF vascular endothelial growth factor & its receptors in BOOP > UIP J Pathology Feb 2002 J Pathology Feb 2002 Higher Apoptotic Activity Higher apoptotic activity index in BOOP > UIP Similar levels of apoptosis regulating proteins Lung 1999 Lung 1999

18
Relapse Predictors Retrospective study GERM “O”P Registry 1100 cases by 1999 Looking for relapse characteristics & possible predictors & possible predictors Inclusion criteria 1) Bx diagnosis 1) Bx diagnosis 2)Compatible clinical & radiological picture 2)Compatible clinical & radiological picture 3)Absence of etiology 3)Absence of etiology 4) Treatment with steroid 4) Treatment with steroid Am Jr Respir Crit Care Med vol 162 2000 Am Jr Respir Crit Care Med vol 162 2000
 Bx diagnosis 1) Bx diagnosis 2)Compatible clinical & radiological picture 2)Compatible clinical & radiological picture 3)Absence of etiology 3)Absence of etiology 4) Treatment with steroid 4) Treatment with steroid Am Jr Respir Crit Care Med vol Am Jr Respir Crit Care Med vol")
19
Study Population 1993 1997 48 / 92 cases were included 65% Female 35% Male Mean Age 61y 71% Non smoker

20
Study Population Symptoms duration prior to Dx 13weeks Dx was made by surgical Bx 69% Transbronchial Bx 31% Transbronchial Bx 31% Follow up 35 months

24
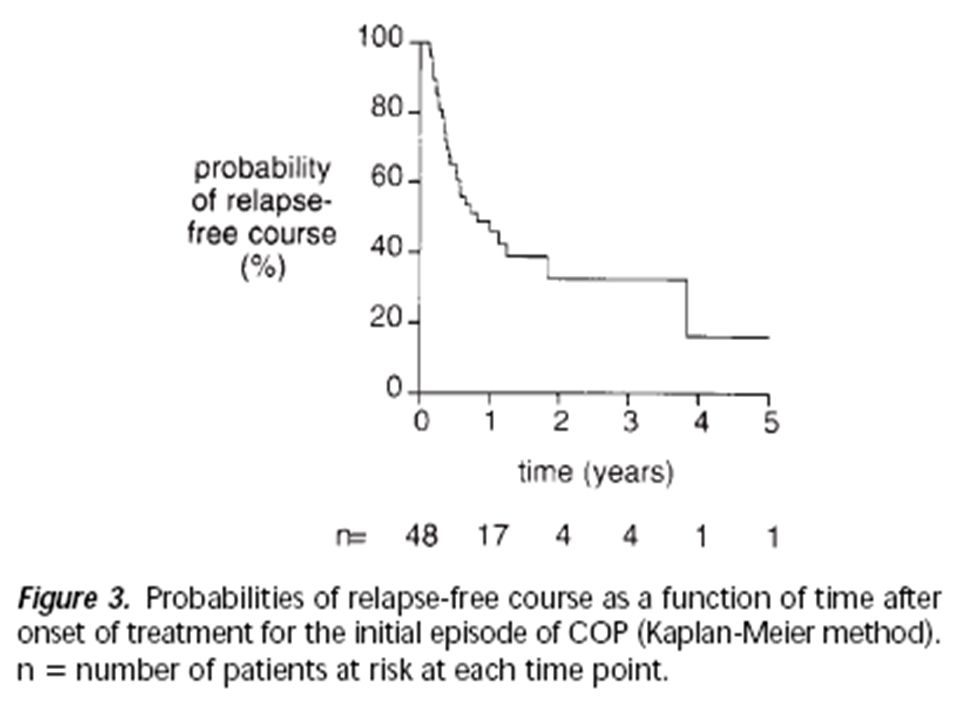
Relapse Predictors 42% had no relapse NR 31% experience single relapse 27% experience >1 relapse MR Time of relapse 6 months from initial episode Highest probability of relapse in the first year

27
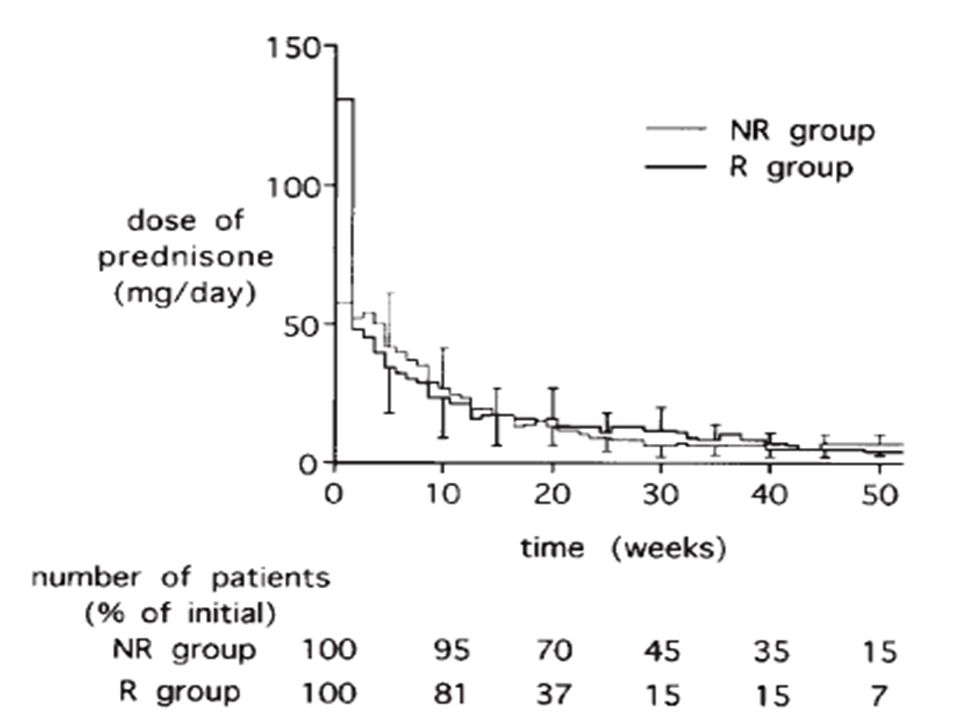
Relapse Predictors 68% were still on prednisone at time of relapse Mean dose at relapse time 12 mg Statistical significant predictors NR Vs MR Delay between symptoms & diagnosis Delay between symptoms & diagnosis Elevated GGT, Alk Phos & ALT Elevated GGT, Alk Phos & ALT NO difference in Age, Gender, Smoking, PFT or BAL or steroid dose in Age, Gender, Smoking, PFT or BAL or steroid dose

29
Outcomes No significance difference NR Vs MR clinical, radiological & PFT at last follow up clinical, radiological & PFT at last follow up 5 y survival 95% 2 Mortality PE & rupture AAA 2 Mortality PE & rupture AAA Steroid Side effects were similar NR Vs MR

30
Will Low Dose Steroid Do the Job 12/28 MR treated with <20 mg prednisone 16/28 MR >20 Similar relapse number & clinical course Slower radiological improvement in Low dose More steroid side effects in High dose

Similar presentations









 Fellow of Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital.>")
 Admitted D6 with 1 week H/O: SOBE, Cough, minimal sputum SOBE, Cough, minimal sputum ? Fever &>")














