Download presentation
Presentation is loading. Please wait.

1
hepatitis c and tuberculosis Tumelo Roestoff FCP(SA) Fellow of Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital
 Fellow of Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital")
2
is there a link between the two entities?

3
>10%2.5–10% 1–2.5% WHO. Wkly Epidemiol Rec 2002; 77: 41 Epidemiology

7
Impact of hepatitis C infection on TB treatment

9
1)normal liver chemistry before starting anti-tuberculosis treatment; 1)the patient was receiving INH, RMP or PZA alone or in combination for at least 5 days before the development of abnormal liver chemistry; 2)an increase in ALT and/or AST to 3 times the upper limit of normal (ULN) with symptoms, or an increase in ALT and/or AST to 5 times the ULN without symptoms; 3)no other apparent cause for the elevation of liver chemistry, such as excessive alcohol intake; and 1)removal of the medications re- sulted in a normalisation or at least a 50% improve- ment of the abnormal liver chemistry. Definition of DIH (DILI)
.")
13
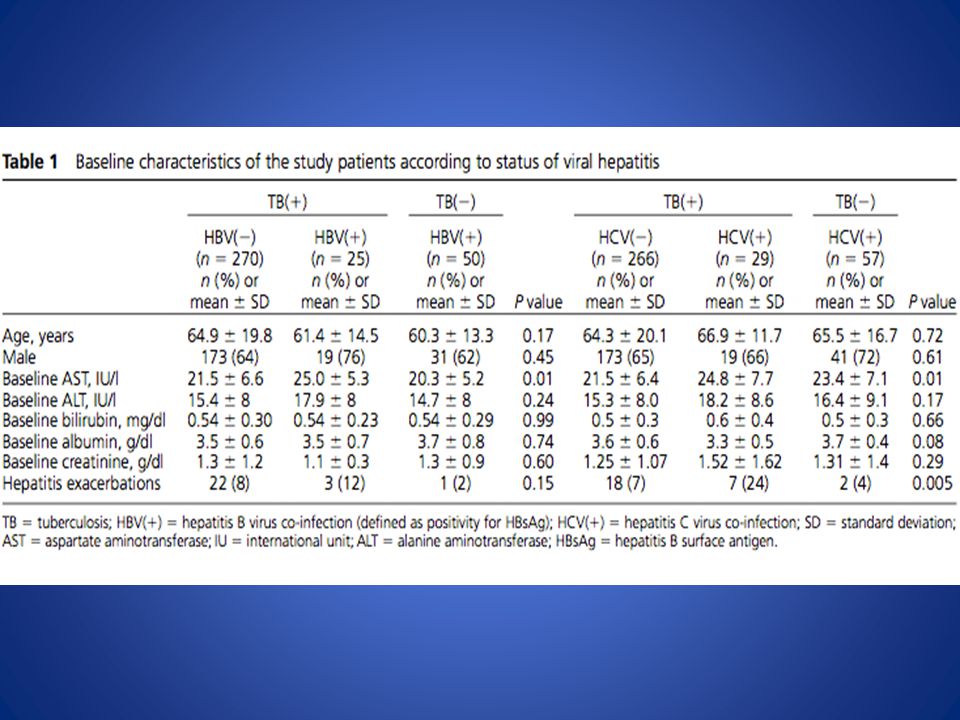
“Co-infection with HBV was not associated with a higher rate of hepatitis but was associated with later onset (102 ± 68.7 vs. 37.0 ± 31.9 days, P = 0.01), higher peak alanine amino- transferase level and slower recovery (55.5 ± 62.9 vs. 15.4 ± 10.8 days, P = 0.01).” JY chien et al. Int J tuberc lung disease, 2010; 14(5): 616 - 621
, higher peak alanine amino- transferase level and slower recovery (55.5 ± 62.9 vs ± 10.8 days, P = 0.01). JY chien et al. Int J tuberc lung disease, 2010; 14(5):")
14
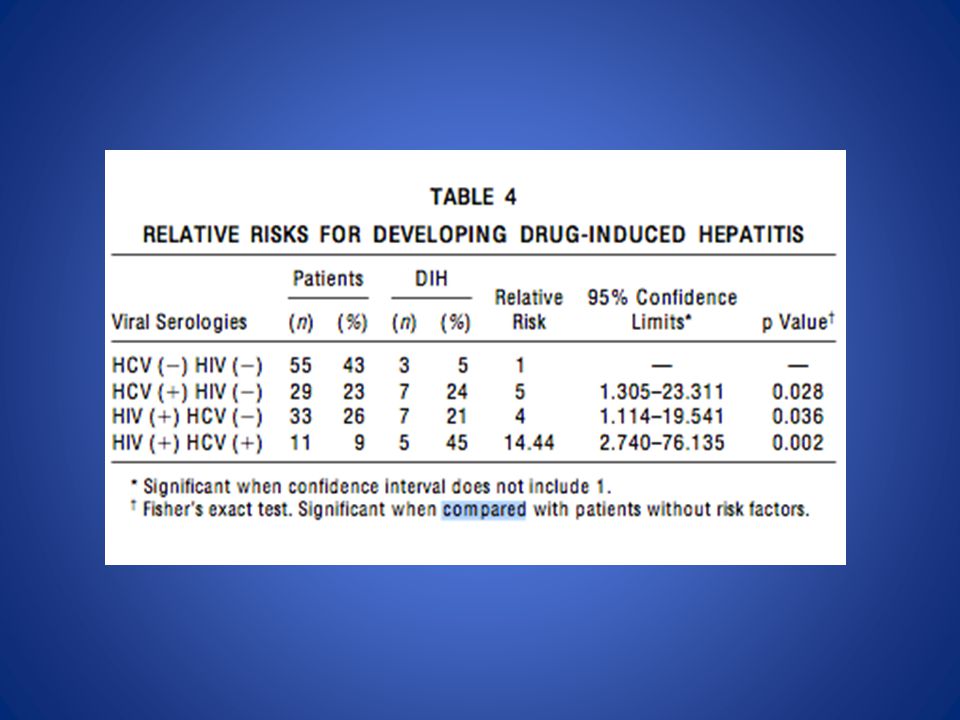
AM J RESPIR CRIT CARE MED 1998;157:1871–1876.

17
6 patients relapsed with reintroduction of TB treatment 2 were excluded because of HIV co- infection 4 patients consented to interferon alpha 2a therapy – This allowed succesful re-introduction of TB therapy and completion of treatment – Variable response in terms of Hep C viral loads, but no SVR attained in any of the patients UNGO J.R et al, AM J RESPIR CRIT CARE MED 1998;157:1871–1876.

18
Impact of TB on Hepatitis C therapy

19
Respiratory: Bronchitis (≥1% to ≤5%), epistaxis (≥1% to ≤5%), nasal congestion (≥1% to ≤5%), nasopharyngitis (≥1% to ≤5%), pharyngolaryngeal pain (≥1% to ≤5%), rhinitis (≥1% to ≤5%), sinus congestion (≥1% to ≤5%), throat sore (≥1% to ≤5%), upper respiratory infection (≥1% to ≤5%), pneumonia (HIV-HCV coinfection: ≥1% to ≤3%) UPTODATE Pegylated Interferon alpha 2a and Ribavarin Adverse reactions significant ( 1 – 10%) Warnings/Precautions Disease related concerns: Infectious disorders: Interferon therapy may cause or aggravate fatal or life-threatening infectious disorders; discontinue if signs and symptoms occur. Investigate the etiology of any persistent fever during therapy.

20
Numbers are not overwhelming – controversial as to whether treatment can result in TB infection Mostly case reports One study looking at HepC and HIV co- infected population Adverse effects in treatment

21
Reactivation?

22
Scandinavian journal of infectious diseases; 2006

23
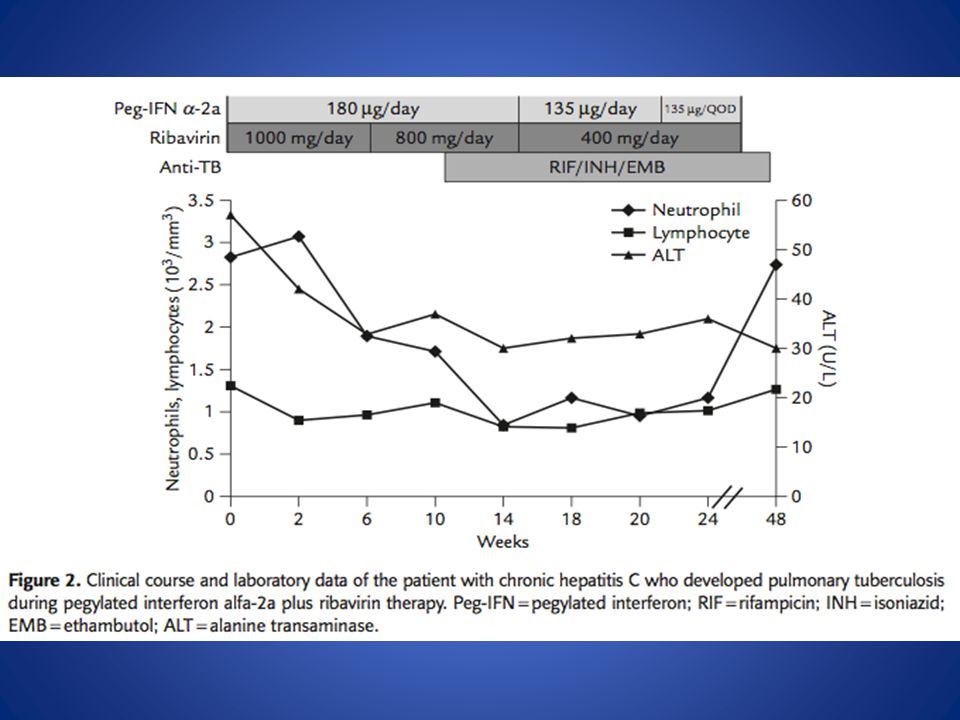
62yr old gentleman Developed cough and haemoptysis 7months into therapy with Pegylated Interferon and Ribavarin CT chest suggestive and Montoux was positive, bronchoscopy and sputum– both smear positive and MTB was cultured

25
CD 4 + depletion to below 290 and abnormal CD4+:CD8+ ratios Patient was smear positive for a total of 13 weeks on treatment Subsequent normalisation of CD4+ count with TB treatment

26
J Formos Med Assoc 2009;108(9):746–750]
![J Formos Med Assoc 2009;108(9):746–750]](http://images.slideplayer.com/13/3864266/slides/slide_26.jpg "J Formos Med Assoc 2009;108(9):746–750]")
27
55yr old Taiwanese lady Type 2 Diabetes Mellitus HepC genotype 2a/2c Cirrhosis on liver biopsy Symptoms began 8 weeks in to therapy with combination pegylated interferon alpha 2a and Ribavarin

32
Complication of therapy? - controversial

34
n = 97

37
TB complicating Hep C therapy in the HIV population

38
Clinical Infectious Diseases 2009;48:e82–5

39
Retrospective observational study 3 hospitals in Madrid Spain Interferon based therapy for HepC between 1996 and 2007 HIV and Hep C con-infected patients Results: 570 patients 4 developed TB during therapy

40
Key points: All therapy was discontinued upon diagnosis of TB Diagnosis was severely delayed – Clinical features were attributed to the side effects of therapy

41
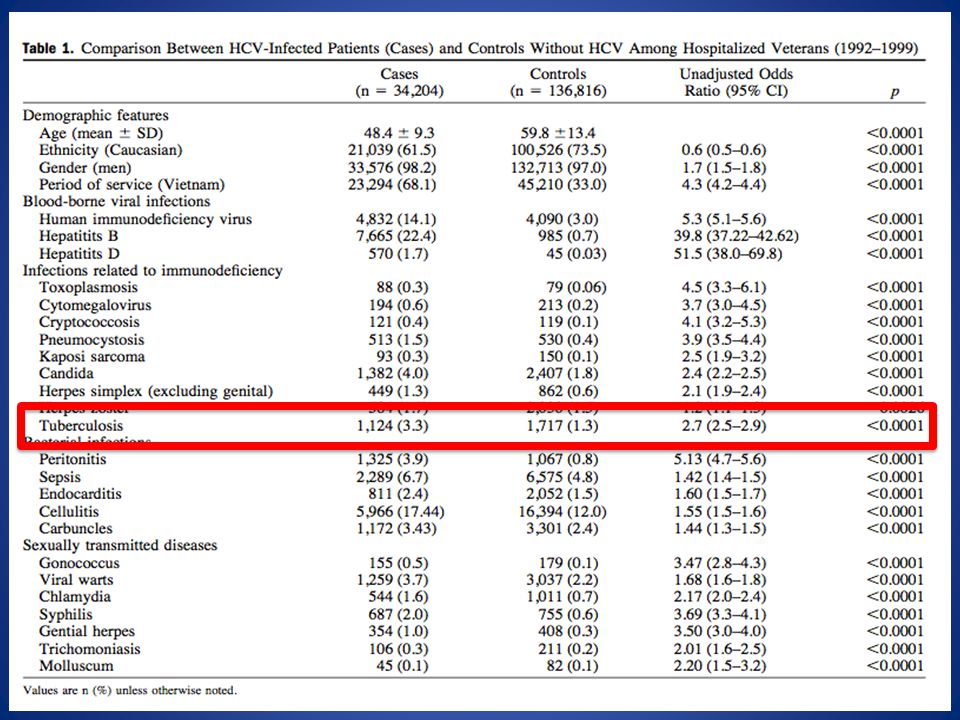
conclusion Hepatitis C is a risk factor for TB DILI It appears to be responsible for cases of reactivation of latent TB – May influence clinical practice It does rarely complicate interferon based HepC therapy in the low incidence areas of the world ?treatment impact in high TB incidence areas such as Sub-Saharan africa.

42
Thank you

Similar presentations
































 Gram (+) rod (bacilli). Acid-fast Pulmonary.>")