Download presentation
Presentation is loading. Please wait.

1
Case presentation 1 Dr REESAUL R

2
Case 1 Male 25 years old Ref on 06/04/2006 to poudre d`or hospital from private GP Ref on 06/04/2006 to poudre d`or hospital from private GP Cough hemoptysis and dyspnea

3
Case 1 He had several visits AHC and private doctors for cough since early childhood : ATB, cough mixture and discharge with diagnosis acute bronchitis ATB, cough mixture and discharge with diagnosis acute bronchitis Since last 4 months severe cough and night fever he visited 4 AHC and twice casualty VH, each visits : ATB, cough mixture, PCM discharge home diagnosis acute bronchitis ATB, cough mixture, PCM discharge home diagnosis acute bronchitis Refer on 6/4/06 by private doctor to chest clinic

4
Case 1 Single work in `pizza hut` since 5 years Brother had TB 6 years back Smokes 5 cig daily since 10 years IVDA since 3 years Alcohol on/off

5
Case 1 Examination : 1m74,52 kg cachexia weight loss 10kg/4 months Temp 38.5, productive cough, dyspnoea with orthopnea, mild haemoptysis and L chest pain Crackles 2 lungs Bp 120/80, pulse 120

6
Case 1 Spo2 : 87 % at rest CXR (7/4/06): R + L opacities left effusion ABG at rest : Po2: 59 mmhg, Pco2 : 34mmhg, Ph 7.39 Po2: 59 mmhg, Pco2 : 34mmhg, Ph 7.39 Tapping Left effusion 100 ml protein: 3.5g/l, glucose: 6.5mmol protein: 3.5g/l, glucose: 6.5mmol cytology : lymphocytes +++ cytology : lymphocytes +++ no malignant cells Sputum analysis
: R + L opacities left effusion ABG at rest : Po2: 59 mmhg, Pco2 : 34mmhg, Ph 7.39 Po2: 59 mmhg, Pco2 : 34mmhg, Ph 7.39 Tapping Left effusion 100 ml protein: 3.5g/l, glucose: 6.5mmol protein: 3.5g/l, glucose: 6.5mmol cytology : lymphocytes +++ cytology : lymphocytes +++ no malignant cells Sputum analysis")
7
CXR on admission 6/4/06

8
Cytology report effusion

9
Case 1 Diagnosis young male-IVDA-bilateral DIL opacities U>L with exsudative effusion with lymphocytes hypoxia-hypocapnia young male-IVDA-bilateral DIL opacities U>L with exsudative effusion with lymphocytes hypoxia-hypocapnia Atypical pneumonia or viral pneumonia?Atypical pneumonia or viral pneumonia? Pleuro-pneumonia in IVDA?Pleuro-pneumonia in IVDA? Pulmonary tuberculosis with pleural TB?Pulmonary tuberculosis with pleural TB? Cystic fibrosis with chest infection involvement?Cystic fibrosis with chest infection involvement? Pneumocystose Jirovecy immuno-suppression?Pneumocystose Jirovecy immuno-suppression? Pulmonary oedema with endocarditis in IVDA?Pulmonary oedema with endocarditis in IVDA? Systemic disease with lung involvement?Systemic disease with lung involvement? Malignancy with lung involvement?Malignancy with lung involvement? PE?PE?

10
Case 1 FbC N with ESR 40, SGOT/SGPT raise Mantoux test : 12mm Blood culture : negative Serology HIV : negative Sputum : pseudomonas aeruginosa +++ Sputum AFB direct : +++ Sweat test normal at VH lab Serology chlamydia and mycoplasma negative ANF negative ECG normal, Echo doppler cardiac normal D-dimer negative

11
Sputum result 12/4/06

12
Blood test HIV

13
Blood test FBC ESR

14
Blood test LFT

15
case1 Positive findings AFB direct +++ AFB direct +++ Pseudomonas A +++ Pseudomonas A +++ Exsudative lymphocytic effusion Exsudative lymphocytic effusion Mantoux 12mm Mantoux 12mm other findings HIV negative Blood culture negative Serology mycoplasma chlamydia negative Sweat test normal ANF negative Cytology effusion no malignancy Echo Doppler cardiac normal D-dimer negative

16
Case 1 Diagnosis : pulmonary TB and with pseudomonas infection pulmonary TB and with pseudomonas infection Initiated on anti TB drugs : IRP and Ethambutol IV ceftazidime 1g TDS + colistin neb 1mu bd + IV amikacin 750mg od Solumedrol 40mg iv od O2 : 3-4 l/m IV fluids

17
Case 1 Clinical improvement on antibiotics and anti TB drugs Day 6 th sputum pathogen negative with still sputum direct AFB ++ Final Diagnosis pulmonary TB Final Diagnosis pulmonary TB Antibiotics and steroids stop after 7 days continuation of Anti TB drugs

18
Case 1 Day 10 th severe skin rash with pruritis ATT stop and initiated on anti-H1 and prednisone 40mg Reintroduction pyrazinamid then ethambutol then rifampicin On 50mg isoniazid pruritis and rash Desensitization to isoniazid

19
Case 1 Day 30 th : sudden onset dyspnea and R chest pain in ward Temp 36 BP 130/60 pulse 130 Spo2 : 87% Hypoventilation right lung Possible diagnosis ? PNO- PE

20
CXR Sudden dyspnea

21
Case 1 CXR : complete R pneumothorax Chest drain inserted R side in surgical unit SSRN 5 th day complete re-expansion R chest and drain removed transfer back to poudre d`or hospital

22
CXR insertion R chest drain

23
CXR chest drain remove day 5

24
Case 1 Sputum month 1 AFB + Sputum month 2 AFB + Sputum month 3 AFB negative CXR : improving Discharge on IR and B6 follow up OPD chest Clinic Culture sputum M tuberculosis sensitive to IRES

25
Sputum result month 1

26
Sputum result month 2

27
Sputum result month 3

28
CXR after 6 month treatment

29
Culture sputum

30
Culture/Sensitivity results

31
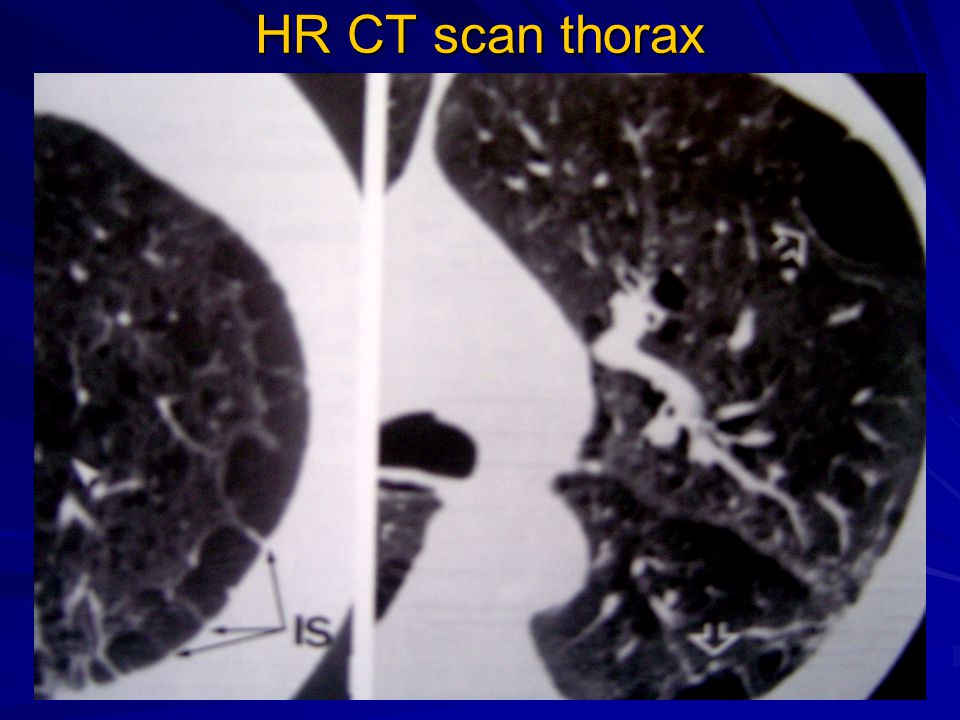
Case 1 Regular follow up at chest clinic out patient Off all respiratory symptoms CXR improving Sputum AFB negative HR CT scan thorax cause PNO : emphysema causes : smoking Deficiency alpha anti- trypsin ? Spirometry obstructive lung disease Complete course of 6 months regiment anti Tb

32
HR CT scan thorax

34
CRX after 1 year

35
we have several thousands years of TB behind us………..still 24 th march 1905 we have several thousands years of TB behind us………..still 24 th march 1905

37
Thank you Merci

Similar presentations















 Aboriginal 1 Month Cough, SOBE,Fever Cough non productive No orthopnea, PND, LL swelling Fever.>")

. -Cytological tests (>")


 Gram (+) rod (bacilli). Acid-fast Pulmonary.>")