Download presentation
Presentation is loading. Please wait.

1
CASE #1

2
Crash em up... 18 yo belted male, MVC on 2 lane, rollover 2 a.m., car is all smashed up... -Awake, GCS 15, HR=125, RR 14, BP 80/60 –”I can’t move my arms and legs….” -Head atraumatic - Neck, chest/abd ok - Extremities atraumatic -Neuro exam – what do you want to know?

3
Crash em up... 18 yo belted male, MVC on 2 lane, rollover 2 a.m., car is all smashed up... -Awake, GCS 15, HR=125, RR 14, BP 80/60 –”I can’t move my arms and legs….” -Neuro exam – no motor function to lower or upper extremities, no sensory function below neck.

4
Smash em up... Arrive at Trauma Center: 3 liter IVF (1 prehospital, 2 in ED) HR 125, BP 85/60 Still can’t move arms/legs…
 HR 125, BP 85/60 Still can’t move arms/legs….")
5
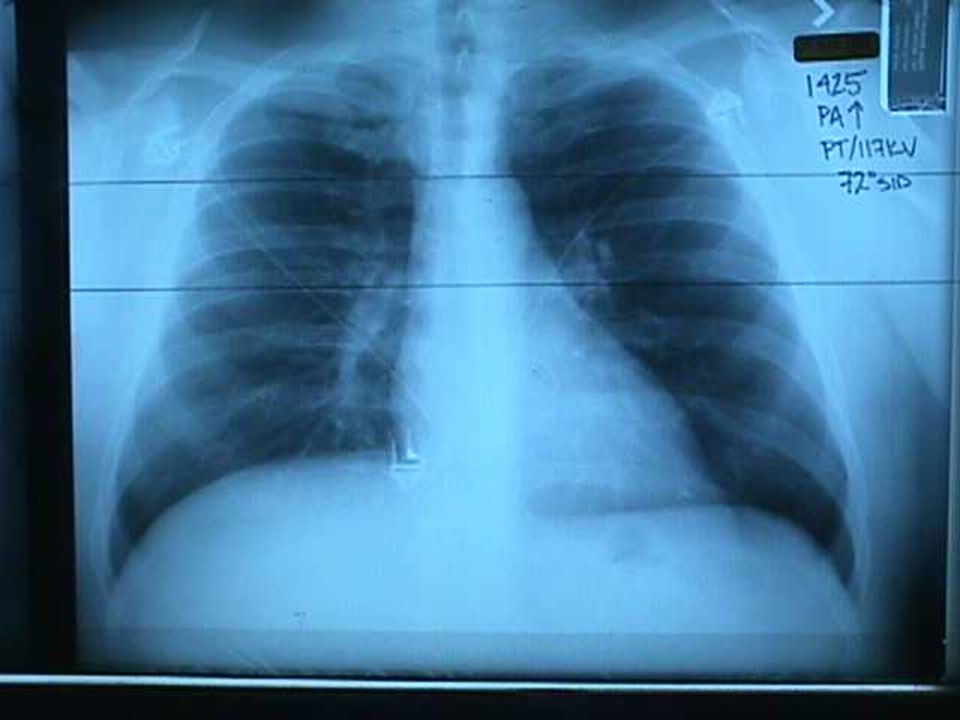
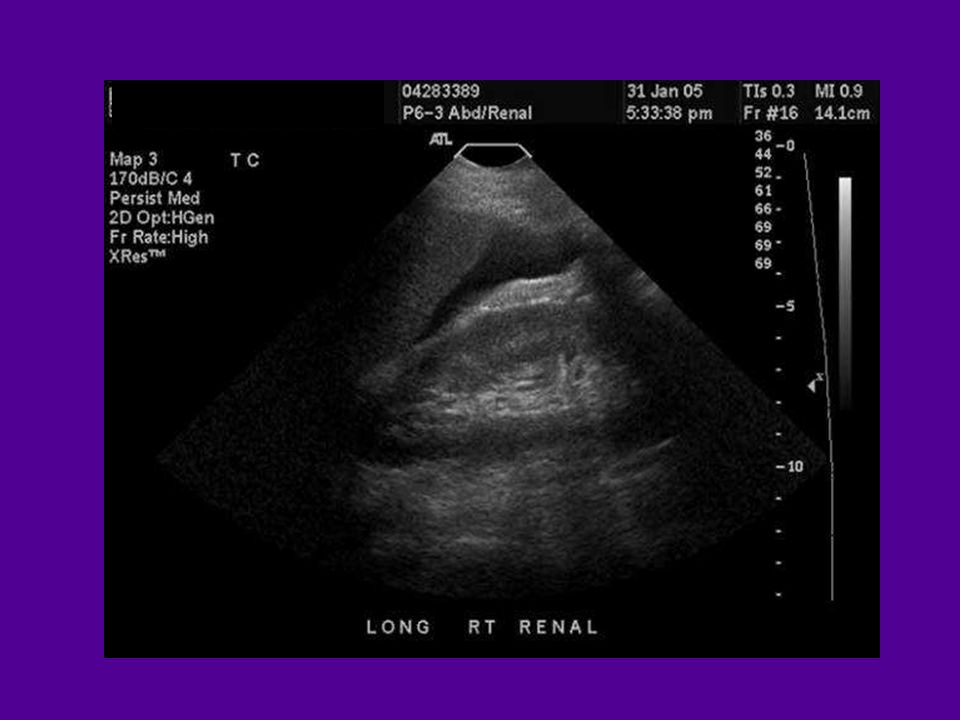
Where’s the blood? Chest… Abdomen… Pelvis… Thigh… Spine… Head... CXR U/S FAST, CT Pelvis XR Thigh Exam Spine XR/CT, exam Head exam, CT

8
Cervical Alignment l Anterior vertebral body l Posterior vertebral body l Spinolaminal line l Spinous process tips

10
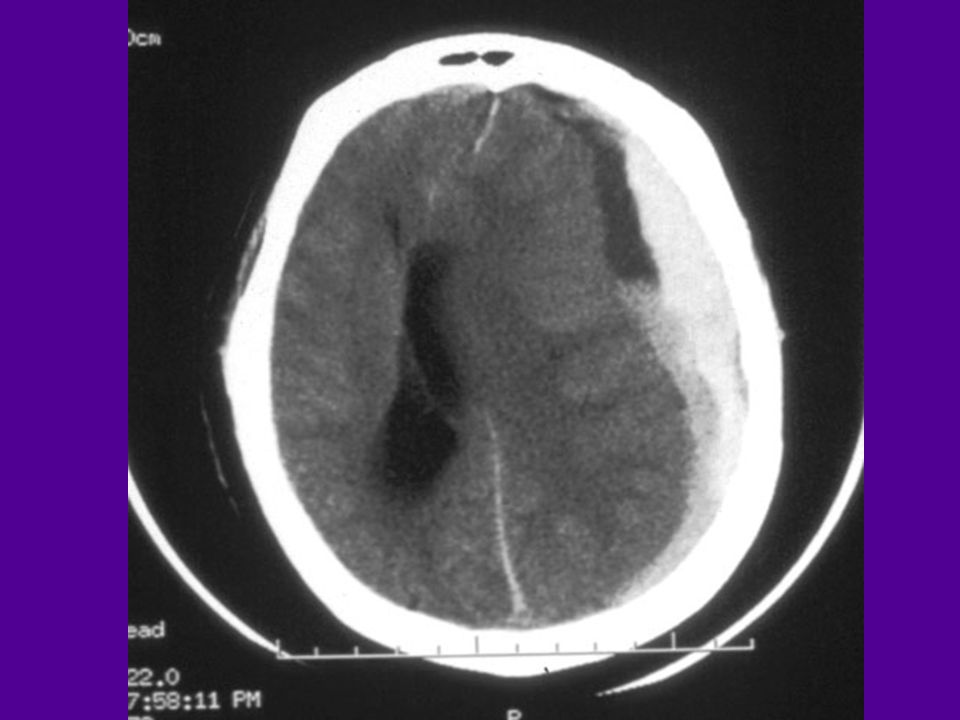
Compression/Burst fracture

13
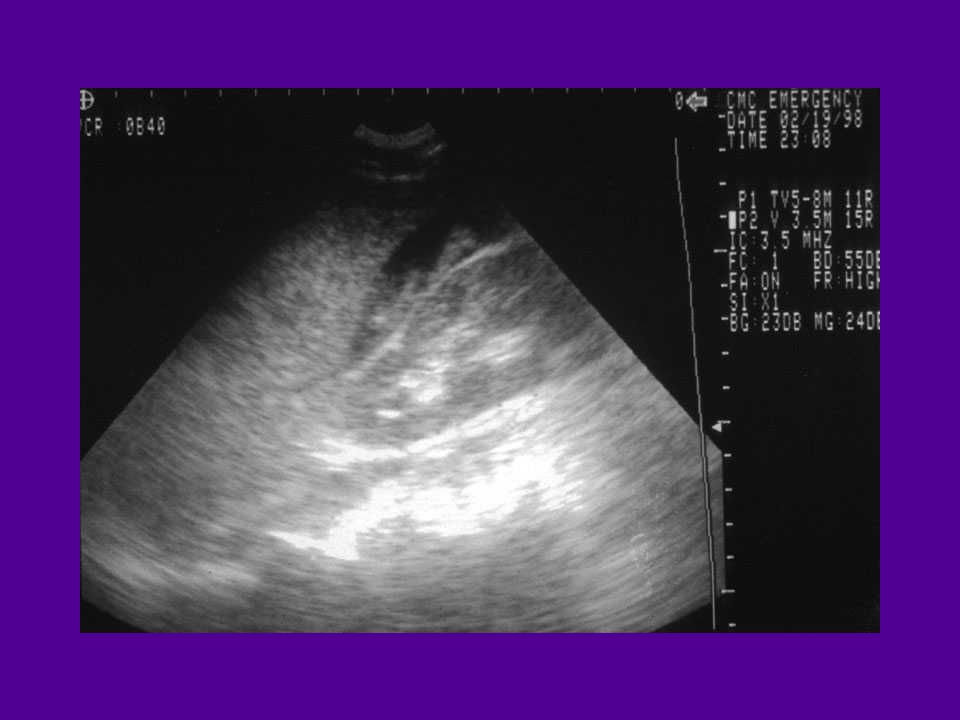
Where’s the blood? Chest… Abdomen… Pelvis… Thigh… Spine… Head... CXR Normal U/S: fluid! Pelvis XR Normal Thigh exam ok Abnormal neuro/XR! Norml exam

14
Manage Blood in the Abdomen: Fluid, Blood, OR Manage Neuro Shock: Pressors (dopamine)
")
15
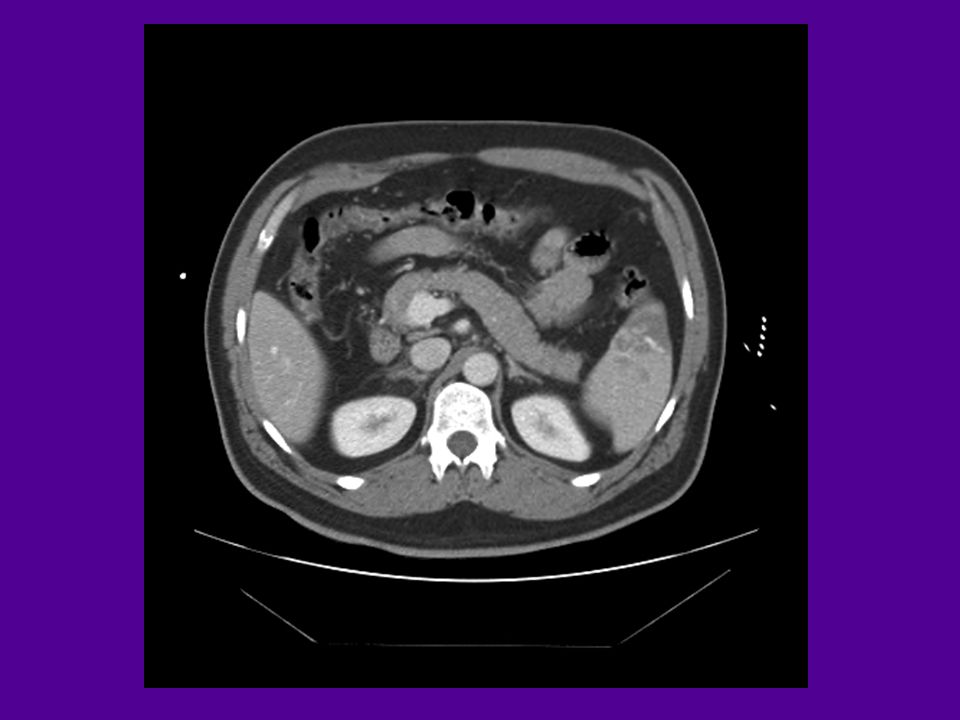
If he’s still hypotensive: OR! If BP normalizes: CT! 3 liters IVF…. BP 95/60, HR 110…

18
Where’s the blood? Chest… Abdomen… Pelvis… Thigh… Spine… Head... CXR Normal U/S: fluid! CT++ Pelvis XR Normal Thigh exam ok Abnormal neuro/XR Norml exam

19
Crash em up... 18 yo belted male, MVC on 2 lane, rollover 2 a.m., car is all smashed up... -Awake, GCS 15, HR=125, RR 14, BP 80/60 –”I can’t move my arms and legs….” -Neuro exam – no motor function to lower or upper extremities, no sensory function below neck. Goes to the OR – remove the spleen. Stabilizes….. Neurosurg next – stabilize spine Discharge to a tough road ahead….

20
CASE #2

21
56 yo male -EMS Response for altered level of consciousness -Chief complaint: alcohol detox & suicidality…. Drinks every day, homeless…found in the gutter….. Negative review of systems Transported to Emergency Department and Emergency Psychiatry for medical clearance to detox Meds: NoneNKDA Pmhx: Negative Exam: intoxicated, no signs of trauma, GCS=15 Intoxicated, sobers up in the ED overnight

22
56 yo male -EMS Response for altered level of consciousness -Chief complaint: alcohol detox & suicidality…. Transported to Emergency Department and Emergency Psychiatry for medical clearance Intoxicated, sobers up in the ED overnight 8 a.m.: Psychiatrist consult to me…. “Trying to decide whether he should have a head CT, he’s been falling down a lot lately….”

23
Crocodile Hunter: The Early Years... Future Career? When do we do a Head CT?

24
The Canadian CT Head Rule for Pts with Minor Head Injury The Lancet 2001;357:1391-96 l New Orleans’ CT rule published in 2000 New England Journal Medicine. l 3121 Canadians to 10 large Canadian hospitals.

25
Lancet 01;357:1391-1396 Minor head inj = witnessed LOC, definite amnesia, or witnessed disorientation

26
Basilar Skull FX Clinical Diagnosis -Racoon’s Eyes -Hemotympanum -Battle Signs (Rhino/Otorrhea)
")
27
New Orlean’s/Charity Criteria 7 components: Headache, Vomiting, age>60, drug or Etoh Intox, memory impairment, trauma above the clavicles, seizure. (No GCS, No Mechanism) Haydel: NEJM 2000;343:100-5
 Haydel: NEJM 2000;343:")
28
Developing a decision instrument to guide CT imaging of blunt head injury pts J Trauma 2005;59:954-959 l 21 hospitals. l 13,728 Patients l 917 Injuries on CT (6.7%)
.")
29
Recursive partitioning: 8 Criteria l Evidence of Skull Fracture l Scalp Hematoma l Neurologic Deficit l Altered Level of Alertness l Abnormal Behavior l Coagulopathy l Persistent Vomiting l Age > 65 Years Mower: J Trauma 2005;59:954-959 - Unique to this study

30
Burton’s Rules: Vomiting, age>60, memory impairment, basilar skull or open/depressed, seizure, GCS 60, memory impairment, basilar skull or open/depressed, seizure, GCS <15 +/?Loss of Consciousness and nothing else = No CT

31
Solution: Wear a Helmet

32
56 yo male -EMS Response for altered level of consciousness -Chief complaint: alcohol detox & suicidality…. Transported to Emergency Department and Emergency Psychiatry for medical clearance Intoxicated, sobers up in the ED overnight 8 a.m.: Psychiatrist consult to me…. “Trying to decide whether he should have a head CT, he’s been falling down a lot lately….”

34
Burton’s Rules for Head CT: Vomiting, age>60, memory impairment, basilar skull or open/depressed, seizure, GCS 60, memory impairment, basilar skull or open/depressed, seizure, GCS <15, anything abnormal and a history of alcoholism +/?LOC and nothing else = No CT

37
CASE #3

38
54 year old male Right Hip Injury History: Water Skiing – one ski, right leg Abduction injury PMHx: None Drugs: NoneAllergies: None Exam: GCS=15, pulse ox = 96%; HR=115, BP =145/78 Right hip and knee flexed – pain to right hip. Right hip and knee flexed – pain to right hip. No other injury

40
54 year old male Right Hip Injury History: Water Skiing – one ski, right leg Abduction injury - EMS - Fentanyl –multiple doses - In the ED - MSO4 – 20 mg over multiple doses -XR: Fracture/Dislocation R hip. - “Native” hip dislocation

41
“Native” Hip Dislocation 1) Every hour that passes = 10% increase in ischemic necrosis of femoral head – not to be confused with PROSTHETIC Hip Dislocation 2) Many will not have a fracture – only dislocation 3) Reduction in hip = reduction in pain! 4) Check for neurologic/vascular deficit 5)Immobilize and get moving! (to a trauma center)
 Check for neurologic/vascular deficit 5)Immobilize and get moving. (to a trauma center).")
42
54 year old male Right Hip Injury History: Water Skiing – one ski, right leg Abduction injury - In the ED Propofol for sedation… very heavy sedation, multiple doses - Failed reduction attempts - Reduced in the OR! “Native” hip dislocation

43
CASE #7

44
Fell off the ladder… 65 yom “workin on the roof….fell off the ladder onto my left chest…broke my ribs!” - Hurts when he takes a deep breath. No back/neck pain. No abdominal pain. - Exam: Vitals signs normal. No increased respiratory effort. Normal breath sounds - Tender along left ribs – 9-10 … Nontender abdomen…

45
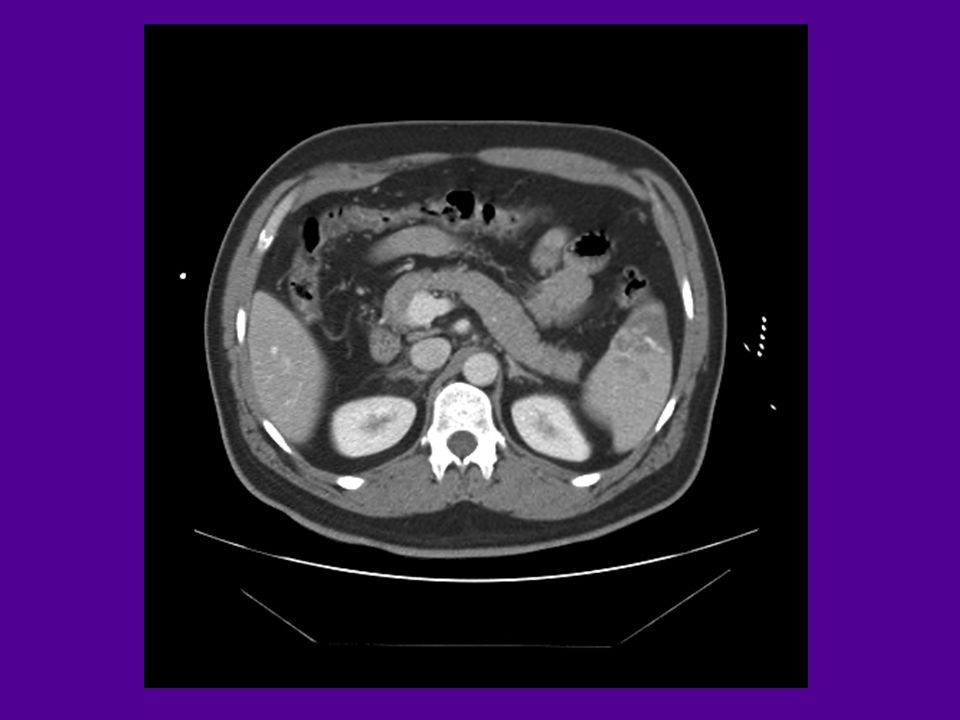
Left Chest Ribs: Fractured/Contusion Lung: Pneumothorax Lung Contusion Diaphragm: Ruptured Diaphragm Spleen: Contusion/Fracture Kidney: Contusion/Fracture Large Bowel: Rupture/Contusion

48
Fell off the ladder… 65 yom “workin on the roof….fell off the ladder onto my left chest…broke my ribs!” - Hurts when he takes a deep breath. No back/neck pain. No abdominal pain. Fractured spleen: observed til hospital day 3 – discharged to followup.

49
CASE #8

Similar presentations






>")

 advance ET tube B) needle thoracostomy.>")









 of Red Flower Oil Repeated vomiting, denied any tinnitus GCS.>")





