Download presentation
Presentation is loading. Please wait.

1
Maitland K et al ,N Engl J Med 2011;364:2483-95
Journal Club 18/04/13 “Mortality after fluid bolus in African children with severe infection” Maitland K et al ,N Engl J Med 2011;364: Robert Morton

2
Clinical scenario Called to resus to see an 18 month old boy admitted with fever & lethargy. On arrival, child is very quiet, respiratory distress and agitated. Cool peripheries and mottled limbs. Cap refill 3 seconds

3
Observations HR 160 BP 95/50 O2 sats 98% in 15L via non re-breathe
Temp 39.5°C RR 40 BM 5.3

4
Management (APLS) A B - high flow 02 C - Gain IV/IO access
Take blood for FBC, U/E ,LFTs, culture, clotting, cross match Give 20ml/kg rapid bolus of crystalloid to all patients except those with signs of heart failure as their primary pathology. Apart from septic shock, it is uncommon to need more than one or two 20ml/kg boluses of fluid. In septic shock, the first bolus of fluid may be given as 4.5% Human albumin solution. Give 80ml/kg 3rd generation cephalosporin

5
?

7
Background Due to lack of intensive care facilities in Africa, WHO recommends reserving the practice of fluid resuscitation for children with advanced shock (CR> 3 seconds, weak fast pulse). Therefore most children admitted with shock in Africa receive no specific fluid management. Study was designed to investigate the practice of early resuscitation with a saline bolus or albumin bolus to improve outcomes.
. Therefore most children admitted with shock in Africa receive no specific fluid management. Study was designed to investigate the practice of early resuscitation with a saline bolus or albumin bolus to improve outcomes.")
8
FEAST trial Fluid Expansion as Supportive Therapy
Population- Children with severe febrile illness & impaired perfusion Intervention ml/kg N. saline or 5% albumin solution Control- No bolus Outcome- Mortality at 48 hrs

9
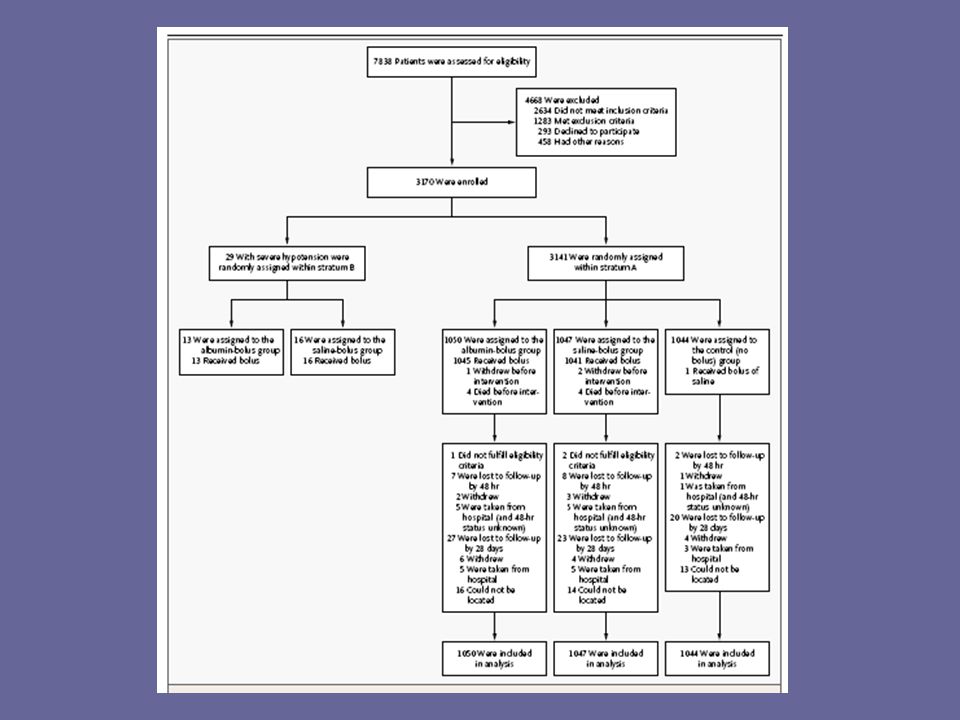
Methods Multi centre RCT (Kenya, Tanzania, Uganda.
Children with septic shock assigned to early intervention with 20ml/kg N. saline or 5% albumin or no bolus. 2 strata, with/ without hypotension

10
Outcomes Primary outcome Mortality at 48hrs Secondary outcomes
Mortality at 4 weeks Neurological sequelae 4 & 24 weeks Episodes of hypotensive shock Adverse reactions to fluids (PO, ICP, allergy)
")
11
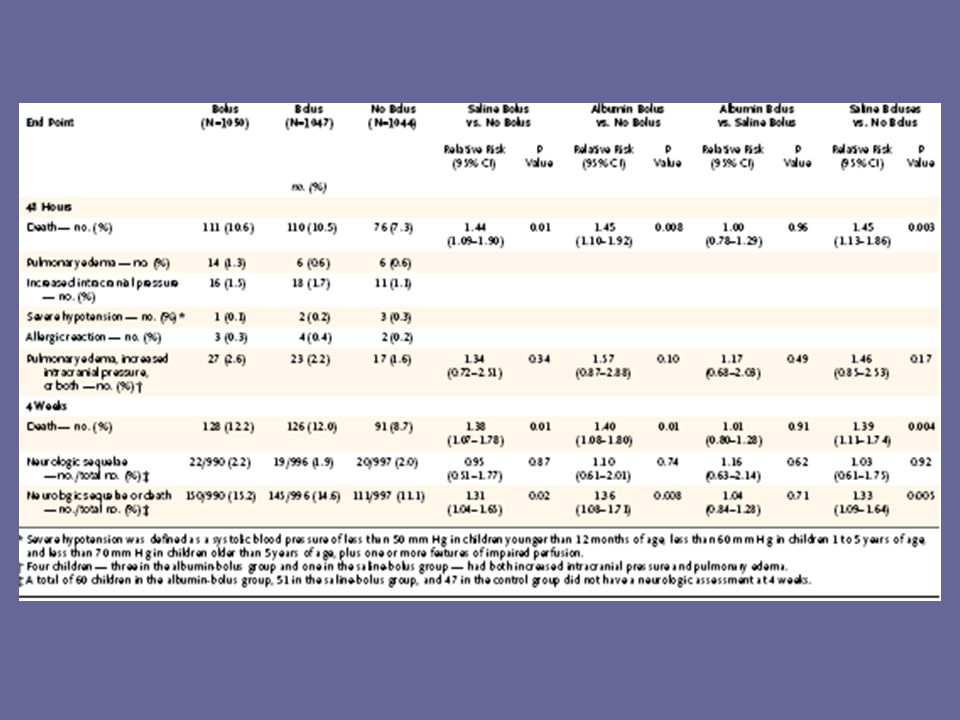
Results Study stopped early due to excess mortality in the bolus groups. 10.6% vs 10.5% vs 7.3%

12
CASP 1. Did the trial address a clearly focused issue?
Yes- Are 48 hr mortality rates increased in children with septic shock who receive fluid boluses?

13
Are the results valid? 2. Was the assignment of patients to treatments randomized? Yes Permuted blocks to achieve 1:1:1 ratio

14
Are the results valid? 3. Were all the patients who entered the trial properly accounted for at its conclusion? Yes Only 17 (0.5%) children lost to follow up at 48hrs 97, 98 & 98% f/u at 4 weeks
 children lost to follow up at 48hrs. 97, 98 & 98% f/u at 4 weeks.")
15
Are the results valid? 4. Were patients, health workers and study personnel “blind” to the treatment? No

16
Are the results valid? 5. Were the groups similar at the start of the trial? Yes

18
Are the results valid? 6. Aside from the clinical intervention, were the groups treated equally? Yes

19
What are the results?

24
Will the results help locally?
?? Different population, intensive care facilites available. Different level of assessment post fluids Different causes of sepsis, 57% malaria in study (but equal across all groups)-can cause haemodilution and anaemia
-can cause haemodilution and anaemia.")
25
Criticism of study Impaired perfusion rather than shock studied
Only 26% cap refill > 3 secs Only 52% 2 signs of shock Only 67 children (2%) fulfilled WHO criteria for shock (cold hands, weak peripheral pulse and CR >3 seconds)
 fulfilled WHO criteria for shock (cold hands, weak peripheral pulse and CR >3 seconds)")
26
Is cap refill a reliable sign of shock?
Is tachycardia? Final diagnoses not published ? SIADH- Na levels not reported

27
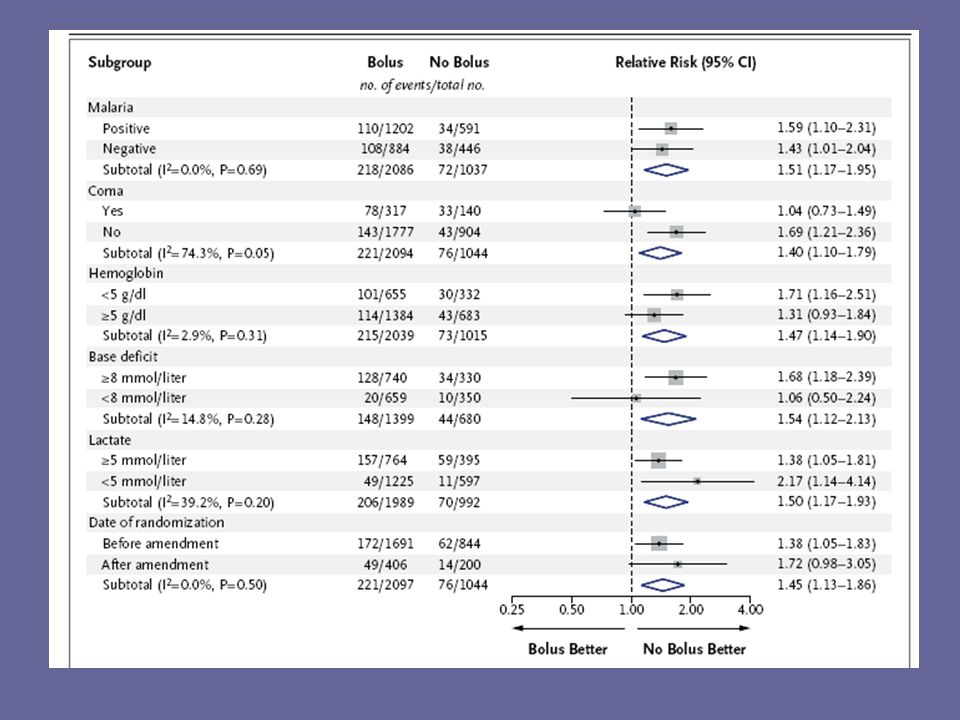
Further analysis Further results published in 2013 showed excess mortality from boluses occurred in all subgroups of children. Mode of death cardiovascular collapse rather than fluid overload

Similar presentations




 for severe sepsis and septic shock treatment>")

>")


:363-369 R. Francavilla.>")









. Formulate Clinical Question Patient/ population Intervention Comparison Outcome (s) Women with IBS Alosetron.>")


