Download presentation
Presentation is loading. Please wait.

1
Management of Severe Dengue

2
Definition Severe dengue: DHF grade 3 and 4
Dengue with severe organ impairment: Dengue with fulminant hepatitis Dengue with myocarditis Dengue with encephalitis Dengue with respiratory distress

3
Clinical course of DHF

4
Clinical assessment for severe dengue and DHF Grade 3 & 4
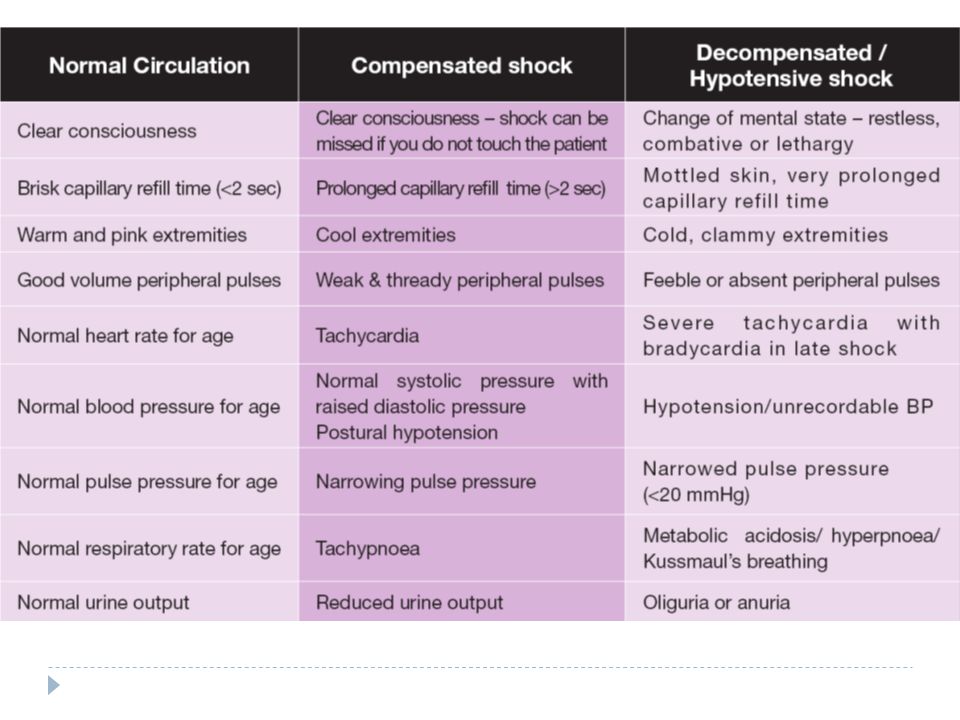
During critical phase: Plasma leakage around defervescence phase: Evidence of plasma leakage includes: raised HCT (early marker), haemodynamic instability, Skin- cool and pallor, delayed capillary refilled time Reduced pulse pressure to < 20 mmHg Tachycardia Hypotension SBP< 90 mmHg fluid accumulation in extravascular space (rathe late marker) Pleural effusion Ascitis hypoproteinemia.
, haemodynamic instability, Skin- cool and pallor, delayed capillary refilled time. Reduced pulse pressure to < 20 mmHg. Tachycardia. Hypotension SBP< 90 mmHg. fluid accumulation in extravascular space (rathe late marker) Pleural effusion. Ascitis. hypoproteinemia.")
5
DHF Grade 3 & 4-clinical assessment
Intense thirst, Abdominal pain, epigastric pain, Vomiting, Restlessness, Reduced urine output Altered conscious level, Shortness of breath and tachypnoea, Sudden change from fever to subnormal temperature

7
Fluid management - When to initiate IV fluid replacement?
Not taking orally Dehydration and rising haematocrit level Diarrhoea Vomiting Decreased sensorium Compensated shock Decompensated shock Cpg style

8
Fluid management - maintenance
Calculations for normal maintenance of intravenous fluid infusion per hour: (Equivalent to Halliday-Segar formula) 4 mL/kg/h for first 10kg body weight + 2 mL/kg/h for next 10kg body weight + 1 mL/kg/h for subsequent kg body weight *For overweight/obese patients calculate normal maintenance fluid based on ideal body weight Ideal bodyweight can be estimated based on the following formula Female: 45.5 kg (height ) cm Male: 50.0 kg (height ) cm
 4 mL/kg/h for first 10kg body weight. + 2 mL/kg/h for next 10kg body weight. + 1 mL/kg/h for subsequent kg body weight. *For overweight/obese patients calculate normal maintenance fluid based on ideal body weight. Ideal bodyweight can be estimated based on the following formula. Female: 45.5 kg (height ) cm. Male: 50.0 kg (height ) cm.")
9
Fluid management - general rules
Frequent adjustment of maintenance fluid regime, X Maintenance in critical phase, If > 1X Maintenance required, regime need to be reviewed 4-6 Hly. Rising HCT- increase infusion rate DSS – fluid resuscitation algorithm Stop fluid therapy once after critical phase and patient is stable (post defevercence).
.")
10
Dengue Shock Syndrome – DHF Grade 3 and 4 (DSS)
Medical emergency Early and prompt management lead to better outcome, Should be nursed in High dependency unit or ICU Fluid resuscitation should be prompt, Following initial resuscitation there maybe recurrent episodes of shock because capillary leakage can continue for hours

11
Fluid management – type of fluid
no clear advantage of using colloids over crystalloids in terms of the overall outcome. colloid may be preferable in patients with intractable shock in the initial resuscitation. The choice of colloids includes gelatin solution (e.g. Gelafusine) and starch solution (e.g. Voluven) Colloids seem to restore the cardiac index and reduce the level of haematocrit faster than crystalloids in patients with intractable shock
 and starch solution (e.g. Voluven) Colloids seem to restore the cardiac index and reduce the level of haematocrit faster than crystalloids in. patients with intractable shock.")
12
DSS – Fluid resuscitation
2 IV lines (largest branula possible) 1st line: for replacement/bolus 2nd line: for blood taking OR blood transfusion
 1st line: for replacement/bolus. 2nd line: for blood taking OR blood transfusion.")
13
DHF GRADE 3 & 4 (DSS) Fluid Resuscitation Algorithm
 Fluid Resuscitation Algorithm")
14
After fluid resuscitation – assessment for improvement
Clinical parameters • Improvement of general well being/ mental state • Warm peripheries • Capillary refill time < 2sec • BP stable • Improving pulse pressure • Less tachycardia • Increase in urine output • Less tachypnoea Laboratory parameters • Decrease in HCT • Improvement in metabolic acidosis

15
If no improvement after the 1st bolus

16
If no improvement after the 2nd bolus

17
If improvement after the bolus(es)
")
18
After 1st bolus fluid – IMPROVED? YES
Clinical parameters must be monitored every minutes during shock! **Fluid regime must be reviewed and readjusted every minutes. Recurrent episodes of shock can occur after initial resuscitation (due to continuing plasma leakage) – for 2nd bolus fluid resuscitation
 – for 2nd bolus fluid resuscitation.")
Similar presentations
>")















. 2 Hyperglycaemia Learning objectives >Can state what hyperglycaemia is >Is aware of the short term and.>")


