Download presentation
Presentation is loading. Please wait.

1
Care of the Preterm Infant: Non-invasive Ventilation and Other Related Important Stuff
SE Courtney, MD MS Professor of Pediatrics Stony Brook University Medical Center

2
Opening the Lung

3
Congratulations! Baby is at OPTIMAL MEAN AIRWAY PRESSURE

4
Optimal Mean Airway Pressure
Benefit Overdistension Atelectasis Pressure

5
CPAP/PEEP: DR and beyond
CPAP/PEEP should be used from the beginning If a self-inflating bag must be used, equip it with a PEEP valve Consider T-piece resuscitator

6
Finer NN et al, Resuscitation 2001
A = residents B = neonatologists C= RRTs Finer NN et al, Resuscitation 2001

7
Use of oxygen

9
Oxygen Toxicity Retinopathy of prematurity
Increased days on ventilator Increased days on oxygen Increased incidence/severity of BPD

10
Finer N and Leone T. Oxygen saturation monitoring for the preterm infant: The evidence basis for current practice. Pediatr Res 2009;65:

11
Oxygen in the Delivery Room
A blender and pulse oximeter should be used Start with 30 or 40% oxygen in the preterm infant Saturations of around 80% at 5 minutes are normal

12
Oxygen in the NICU Saturations of 85-93% appear to be safe

13
Temperature control Admission temperature <36 degrees centigrade is an independent risk factor for mortality in the preterm infant.

16
CPAP and Non-invasive Ventilation

17
Goal of Mechanical Ventilation
To get the patient OFF mechanical ventilation! Airway trauma Infection Decreased mucus clearance Over-ventilation Air leak Contribution to BPD

18
NCPAP is probably a good thing
CPAP Reduces mortality and respiratory failure in RDS Early CPAP reduces need for mechanical ventilation CPAP post-extubation can prevent extubation failure NO STUDY has shown reduction in BPD with use of CPAP under any conditions (testimonials don’t count)
")
19
NCPAP/NIV Constant-flow Variable-flow NIPPV conventional bubble
Infant Flow Bi-level NIPPV

20
Not all CPAP is created equal: Know your equipment
Variable-flow NCPAP recruits lung volume well and decreases work of breathing. Care must be taken to avoid nasal trauma. Bubble NCPAP: pressures must be monitored; they will be higher than the depth of the underwater expiratory tube.

21
CPAP by Conventional Ventilator
Constant flow of air/oxygen. CPAP provided by changing orifice size at expiratory port of the ventilator, thus providing back-pressure. Variety of prongs, usually bi-nasal. Convenient, easily available, inexpensive.

22
“Bubble” NCPAP

23
“Bubble” NCPAP – Do We Know What We’re Doing?
Kahn DJ et al, Pediatric Research 2007;62:343.

24
Kahn et al, Pediatrics, 2007

25
Courtney et al, Bubble vs ventilator NCPAP, J Perinatol 2010
Pp=0.01 Courtney et al, Bubble vs ventilator NCPAP, J Perinatol 2010

26
Variable-Flow (Infant Flow) CPAP
Flow is varied to deliver the required CPAP pressure. The direction of flow depends on the pressures generated by the patient. On inspiration, the CPAP flow is towards the nasal cavity, assisting in inspiration On exhalation, the flow is down the expiratory branch of the CPAP tubing.

27
Childs, Neonatal Intensive Care, 2000

28
What Do We Know About Variable-Flow NCPAP?
Provides a very stable mean airway pressure Decreases work of breathing Increases lung volume recruitment

29
Adapted from Moa G and Nilsson K. Acta Paediatr 1993;82:210.

30
A = Aladdin (Infant Flow)
C = Cannula A = Aladdin (Infant Flow) I = Inca Prongs (Conventional Ventilator) Courtney SE, Pyon KH, Saslow JG et al. Pediatrics 2001;107:
 I = Inca Prongs (Conventional Ventilator) Courtney SE, Pyon KH, Saslow JG et al. Pediatrics 2001;107:")
31
Pandit PB, Courtney SE, Pyon KH et al. Pediatrics 2001;108: 682-685

32
Stefanescu et al, Pediatrics 2003;112:1031

33
Secondary Outcomes Conv IF P Days on O2 77.2 65.7 0.03
Length of Stay Stefanescu et al, Pediatrics 2003;112:1031

34
Apnea Hypoxia Hypercarbia Stefanescu et al, Pediatrics 2003;112:1031

35
NCPAP with a Rate: (NIMV, NIPPV)
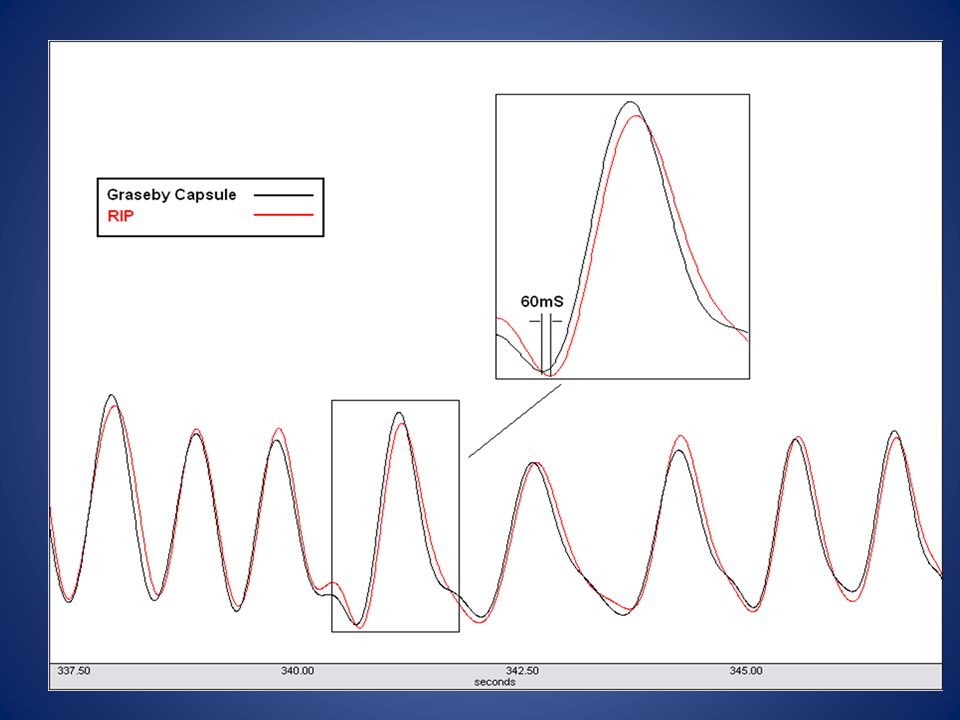
NIMV for reducing apnea and extubation failure Synchronized (?)NIMV reduces the incidence of extubation failure and possibly apnea more effectively than NCPAP. “Synchrony” done with Graesby capsule and Infant Star ventilator No information is available on non-synchronized NIMV. Current studies ongoing
NIMV reduces the incidence of extubation failure and possibly apnea more effectively than NCPAP. Synchrony done with Graesby capsule and Infant Star ventilator. No information is available on non-synchronized NIMV. Current studies ongoing.")
36
Owen LS, Morley CJ, Davis PG. PAS 2009

37
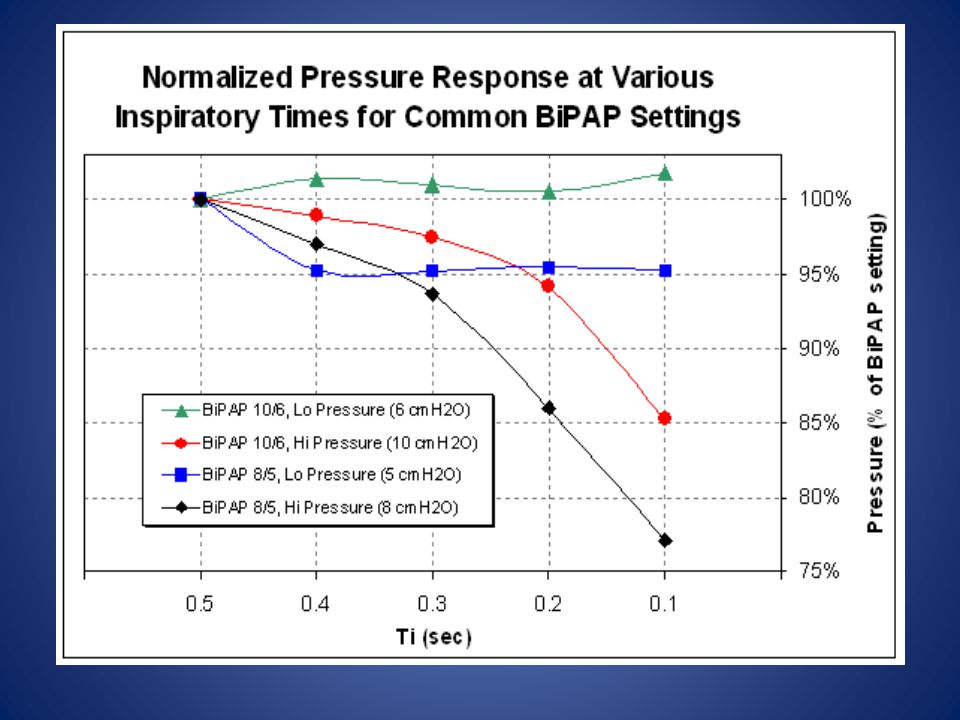
SiPAP What is SiPAP? A small (2-3 cmH2O), slow, intermittent increase in CPAP pressure for a duration up to 3 seconds to produce a “Sigh” Enables the infant to spontaneously breathe throughout the cycle

38
Small increases in IF CPAP pressure can change lung
volume by 4-6 ml/kg. Unlike NIPPV, SiPAP pressure rise is only 2-3 cmH2O 5.5 ml/kg Adapted from Pandit PB, Courtney SE, Pyon KH et al. Pediatrics 2001;108:

39
Decrease work of breathing Stimulate the respiratory center
SiPAP can therefore potentially: Recruit lung volume Decrease work of breathing Stimulate the respiratory center

40
Patients who may benefit from SiPAP:
Infants weaning from mechanical ventilation Premature infants that don’t require aggressive support Infants with apnea

41
Nasal Bilevel vs Continuous Positive Airway Pressure in Preterm Infants. Migliori C et al, Pediatr Pulmonol 2005;40:426.

42
Nasal CPAP vs Bi-level nasal CPAP in preterm infants with RDS: a randomized control study. Lista G et al, Arch Dis Child Fetal Neonatal Ed. 2009 40 infants enrolled, mean GA 30wks, BW 1400g. IF-CPAP SiPAP P Respiratory support (d) 6.2 ± ± O2 dependency (d) 13.8± ± GA at discharge (wk) ± ±
 6.2 ± ± O2 dependency (d) 13.8±8 6.5 ± GA at discharge (wk) 36.7± ±")
43
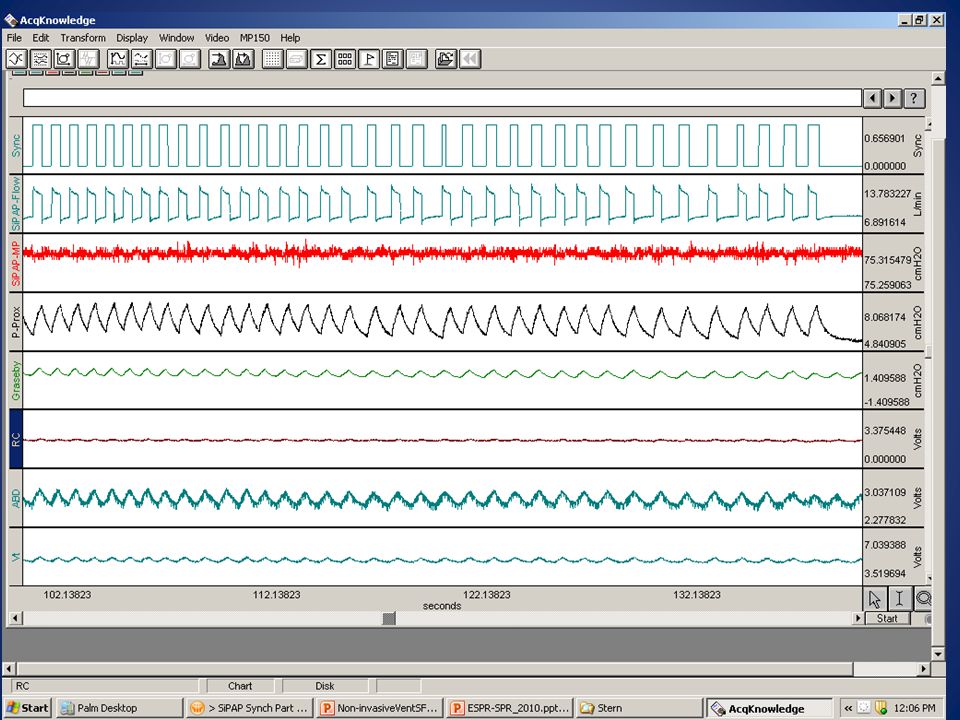
SiPAP vs NCPAP Work of Breathing and Respiratory Parameters S
SiPAP vs NCPAP Work of Breathing and Respiratory Parameters S. Courtney, M. Weisner, V. Boyar, R. Habib 17 infants <1200gms birth weight, on NCPAP for mild respiratory distress Each infant own control; order of application randomized and data collected in two periods for a minimum of one hour, with 15 min on each device in each period (ie, CPAP/SiPAP, CPAP/SiPAP Data collected using calibrated respiratory inductance plethysmography; esophageal balloon for estimation of pleural pressure Continuous monitoring of saturation, pulse, transcutaneous oxygen and carbon dioxide

45
Minute Ventilation n=13 P=0.037

46
Synchronized Non-invasive ventilation

50
Conclusions about SiPAP
Appears to be at least as effective as NCPAP May improve gas exchange and decrease minute ventilation (?decrease WOB) Synchrony may be useful
 Synchrony may be useful.")
51
NCPAP by Nasal Cannula

52
NCPAP by Cannula Uncontrolled positive pressure may be generated with nasal cannula Amount of positive pressure generated will depend on cannula size, flow rate, and shape of nasal passages. High humidity, high flow cannulas also may pose an infection risk.

53
Nasal Cannula Use Current literature would support that gas delivered by nasal cannula: be heated and humidified not exceed 1 L/min in infants <1500gm not exceed 2 L/min in infants >1500gm If CPAP is desired, a CPAP device should be used.

54
Non-invasive Ventilation is not appropriate when…
Infant cannot maintain oxygenation (FiO2 > ) PCO2 >60 pH < 7.25 Increased work of breathing Apnea
 PCO2 >60. pH < Increased work of breathing. Apnea.")
55
Questions……………. Over the long term, is any one form of NCPAP more advantageous than any other? Is non-invasive ventilation combined with NCPAP advantageous? Is S-NIPPV better? When should NCPAP be initiated? When and how should surfactant be given for babies on NCPAP only? What levels of pH and PCO2 are “safe” for babies on NCPAP?

56
Keep an open mind and something useful may fall into it.

Similar presentations



>")




>")


 NICU Population Nursing Educational Series.>")

>")







