Download presentation
Presentation is loading. Please wait.

1
Tutorial: Pulmonary Function--Dr. Bhutani Clinical Case 695 g male neonate with RDS, treated with surfactant and on ventilatory support @ 18 hours age: Settings: 18 / 5 cm H 2 0 x 45 breaths / min; FiO 2 = 0.65 Driving Pressure: 18-5 = 13 cm H 2 0 Arterial Gas: pH = 7.3; PaO 2 = 74 ; PaCO 2 = 55 mmHg Is this baby a candidate for permissive hypercapnia?

2
Normocapnia varies? Maternal : 32 - 34 mmHg (progesterone effect) Fetal: 40 - 42 mmHg At birthing: 45 - 65 mmHg First day : 34 mmHg (progesterone effect) After first week : 35 - 42 mmHg Term PCA: 35 - 42 mmHg (RR = 40-60/min) 52 wks PCA: 35 - 42 mmHg (RR = 20-30/min)
 Fetal: mmHg At birthing: mmHg First day : 34 mmHg (progesterone effect) After first week : mmHg Term PCA: mmHg (RR = 40-60/min) 52 wks PCA: mmHg (RR = 20-30/min).")
3
Strategies to Prevent Non-Permissive Hypercapnia Define optimum P a CO 2 levels Level to at which you will intervene Level to at which you will wean Ventilate at optimal FRC Continuous monitoring of tidal volume Use least pressure for maximal tidal volume Facilitate spontaneous breathing Consider “dual wean” of driving pressures Consider pseudo-adaptive strategies

4
Alveolar Algebra: Ventilation Alveolar Ventilation inversely correlated to PaCO 2 Alveolar Ventilation is (V T -V D ) x rate Provided dead space is constant: proportional changes in V T or rate will lead to proportional changes in alveolar ventilation and PaCO 2. Based on Pulmonary Gas Law: in a steady state, when inspired CO2 is negligible, then PACO2 = 863 (VCO2 / VA); where, VCO2 is CO2 production; PACO2 is partial pressure of carbon dioxide; 863 is body temp. x std. pressure / standard temperature ( 310 X 760/273 = 863 )
; where, VCO2 is CO2 production; PACO2 is partial pressure of carbon dioxide; 863 is body temp. x std. pressure / standard temperature ( 310 X 760/273 = 863 ).")
5
Clinical Case 695 g male neonate with RDS, treated with surfactant and on ventilatory support and is now about 18 hours age and has stable vital signs, normotensive and is normoglycemic: Settings: PIP:18 cm H 2 0; PEEP: 5 cm H 2 0; SIMV: 45 br / min; Arterial Gas: pH = 7.3; PaO 2 = 74 ; PaCO 2 = 55 mmHg Is the Alveolar Ventilation compromised? If so, by how much?

6
Clinical Case 695 g male neonate with RDS, treated with surfactant and on ventilatory support and is now about 18 hours age and has stable vital signs, normotensive and is normoglycemic: Settings: PIP:18 cm H 2 0; PEEP: 5 cm H 2 0; SIMV: 45 br / min; Arterial Gas: pH = 7.3; PaO 2 = 74 ; PaCO 2 = 55 mmHg PaCO 2 = 55 mmHg is 35% higher than 40 mmHg Alveolar Ventilation is decreased by 35%

7
Clinical Case 695 g male neonate with RDS, treated with surfactant and on ventilatory support and is now about 18 hours age and has stable vital signs, normotensive and is normoglycemic: Settings: PIP:18 cm H 2 0; PEEP: 5 cm H 2 0; SIMV: 45 br / min; Arterial Gas: pH = 7.3; PaO 2 = 74 ; PaCO 2 = 55 mmHg PaCO 2 = 54 mmHg is 35% higher than 40 mmHg Questions: Do we wean? Which option?

8
Clinical Case OPTIONS: 1.No Change 2.Reduce PIP by I cm H 2 0 (17/5) : Driving Pressure = 12 cm H 2 0 3. Reduce PEEP by I cm H 2 0 (18/4): Driving Pressure = 14 cm H 2 0 4. Reduce SIMV: Decrease minute ventilation
: Driving Pressure = 14 cm H Reduce SIMV: Decrease minute ventilation.")
9
Clinical Case: Use of Tidal Volume 695 g male neonate with RDS, treated with surfactant and on ventilatory support: Settings: 18 / 5 cm H 2 0 x 35 breaths / min Driving Pressure: 18-5 = 13 cm H 2 0 Tidal Volume (measured): = 4 ml (5.7ml/kg) Effective Compliance: = V / P ; 5.7 / 13 ml/cm H 2 0/kg Arterial Gas: pH = 7.3; PaO 2 = 74 ; PaCO 2 = 55 mmHg
: = 4 ml (5.7ml/kg) Effective Compliance: = V / P ; 5.7 / 13 ml/cm H 2 0/kg Arterial Gas: pH = 7.3; PaO 2 = 74 ; PaCO 2 = 55 mmHg")
10
Clinical Case 695 g male neonate with RDS, treated with surfactant and on ventilatory support: Settings: 18 / 5 cm H 2 0 x 35 breaths / min Driving Pressure: 18-5 = 13 cm H 2 0 Tidal Volume (measured): = 4.0 ml (5.7 ml/kg) Effective Compliance: = V / P ; 5.7 /13 = 0.44 ml / cm H 2 0/kg Arterial Gas: pH = 7.3; PaO 2 = 74 ; PaCO 2 = 55 mmHg
: = 4.0 ml (5.7 ml/kg) Effective Compliance: = V / P ; 5.7 /13 = 0.44 ml / cm H 2 0/kg Arterial Gas: pH = 7.3; PaO 2 = 74 ; PaCO 2 = 55 mmHg")
11
Relationship to FRC

12
Least Intervention or Barotrauma Increase Lung Volume : CPAP Adequate Lung Inflation : T insp. Adequate Lung Deflation : T exp. Adjust T insp. / T exp. : by estimating Time Constants Ventilate at Optimal FRC

13
Clinical Case 695 g male neonate with RDS, treated with surfactant and on ventilatory support: Settings: 18 / 5 cm H 2 0 x 45 breaths / min Driving Pressure: 18-5 = 13 cm H 2 0 Tidal Volume (measured): = 4.0 ml (5.7 ml/kg) Effective Compliance: = V / P ; 5.7 /13 = 0.44 ml / cm H 2 0 Arterial Gas: pH = 7.3; PaO 2 = 74 ; PaCO 2 = 55 mmHg
: = 4.0 ml (5.7 ml/kg) Effective Compliance: = V / P ; 5.7 /13 = 0.44 ml / cm H 2 0 Arterial Gas: pH = 7.3; PaO 2 = 74 ; PaCO 2 = 55 mmHg")
14
(PEEP) 518 (PIP) P = 13 cm H 2 0 V = 5.7 ml/kg Graphic Representation of Ventilator Settings
 518 (PIP) P = 13 cm H 2 0 V = 5.7 ml/kg Graphic Representation of Ventilator Settings")
15
(PEEP) 518 (PIP) P = 13 cm H 2 0 V = 5.7 ml/kg V / P = 5.7 / 13 = 0.44 ml/cm H 2 0 /kg Graphic Representation of Ventilator Settings
 518 (PIP) P = 13 cm H 2 0 V = 5.7 ml/kg V / P = 5.7 / 13 = 0.44 ml/cm H 2 0 /kg Graphic Representation of Ventilator Settings")
16
5 TLC RV 19 P = Driving pressure V V PRESSURE (cmH 2 0) VOLUME Peak Inflating Pressure PEEP 18 17 Linear Change in V/ P V / P = 5.7 / 13 = 0.44 ml/cm H 2 0
 VOLUME Peak Inflating Pressure PEEP Linear Change in V/ P V / P = 5.7 / 13 = 0.44 ml/cm H 2 0")
17
5 TLC RV 19 P = Driving pressure V V PRESSURE (cmH 2 0) VOLUME Peak Inflating Pressure PEEP 18 17 Imaginary P-V relationship
 VOLUME Peak Inflating Pressure PEEP Imaginary P-V relationship")
18
Clinical Case OPTIONS: 1.No Change 2.Reduce PIP by I cm H 2 0 (17/5) : Driving Pressure = 12 cm H 2 0 3. Reduce PEEP by I cm H 2 0 (18/4): Driving Pressure = 14 cm H 2 0 4. Reduce SIMV: Decrease minute ventilation
: Driving Pressure = 14 cm H Reduce SIMV: Decrease minute ventilation.")
19
5 17 18 TLC RV 19 16 P = 12 V V PRESSURE (cmH 2 0) VOLUME Peak Inflating Pressure PEEP Wean Peak Inflating Pressure Tidal Volume decreases with weaning Driving pressure decreased
 VOLUME Peak Inflating Pressure PEEP Wean Peak Inflating Pressure Tidal Volume decreases with weaning Driving pressure decreased")
20
Clinical Case OPTIONS: 1.No Change 2.Reduce PIP by I cm H 2 0 (17/5) : Driving Pressure = 12 cm H 2 0 3. Reduce PEEP by I cm H 2 0 (18/4): Driving Pressure = 14 cm H 2 0 4. Reduce SIMV: Decrease minute ventilation
: Driving Pressure = 14 cm H Reduce SIMV: Decrease minute ventilation.")
21
5 18 TLC RV 19 17 P = 14 V V PRESSURE (cmH 2 0) VOLUME Peak Inflating Pressure PEEP 4 Wean PEEP Tidal Volume increases with weaning Driving pressure increased
 VOLUME Peak Inflating Pressure PEEP 4 Wean PEEP Tidal Volume increases with weaning Driving pressure increased")
22
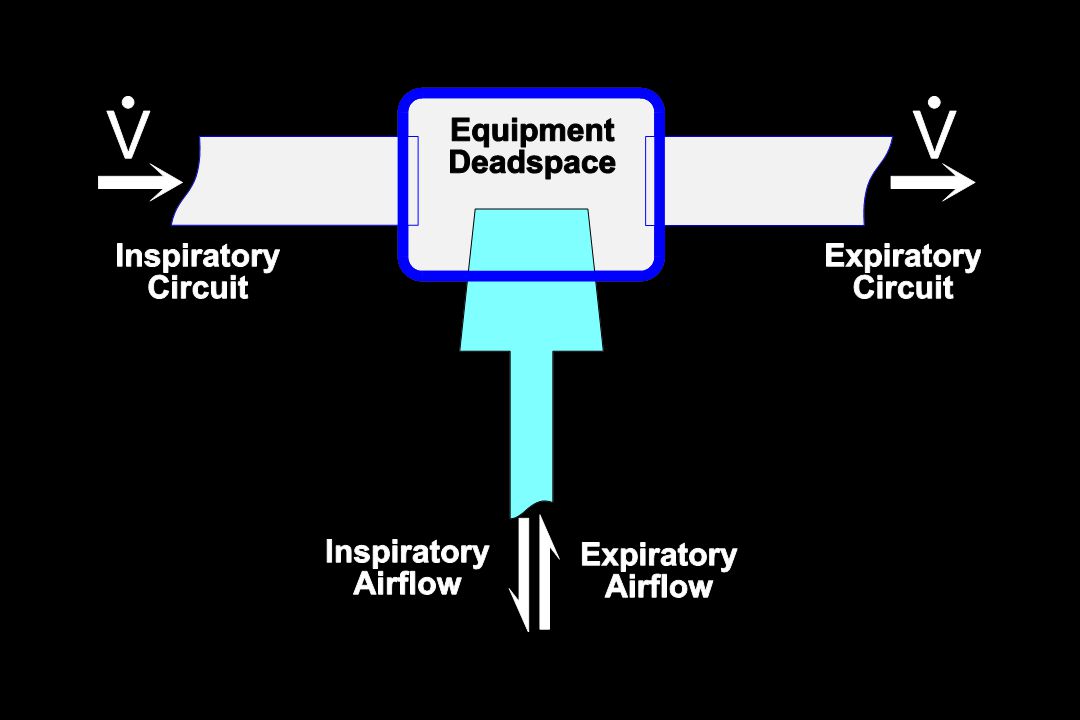
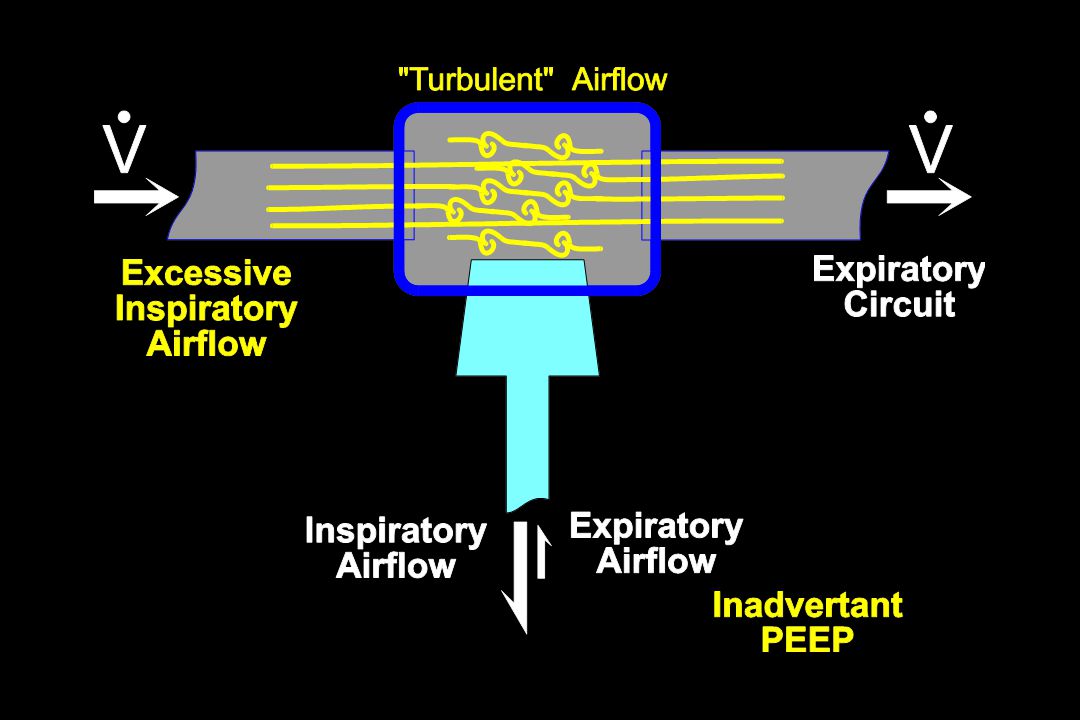
Circuit Airflow Airflow that is set, at operator’s discretion, to flow from inspiratory to expiratory circuits. Magnitude dependent on patient’s minute ventilation Excessive circuit airflow can lead to turbulence and may impede expiratory flow from the patient Low flow may limit inspiratory airflow Optimal circuit flow is about 5 to 8 fold minute ventilation

25
Clinical Case OPTIONS: 1.Dual Wean: Reduce both PIP/PEEP Dual Wean: 18/5 to 17/4 cm H 2 0 = Driving Pressure = 13 cm H 2 0

26
5 17 18 TLC RV 19 16 P = 13 V V PRESSURE (cmH 2 0) VOLUME Peak Inflating Pressure PEEP 4 DUAL WEAN: concurrent wean of both PIP and PEEP Tidal Volume increases with weaning Driving pressure unchanged
 VOLUME Peak Inflating Pressure PEEP 4 DUAL WEAN: concurrent wean of both PIP and PEEP Tidal Volume increases with weaning Driving pressure unchanged")
27
5 18 TLC RV 14 P = 10 V V PRESSURE (cmH 2 0) VOLUME Peak Inflating Pressure PEEP 4 DUAL WEAN that allows for permissive hypercapnia Tidal Volume unchanged with weaning Driving pressure decreased
 VOLUME Peak Inflating Pressure PEEP 4 DUAL WEAN that allows for permissive hypercapnia Tidal Volume unchanged with weaning Driving pressure decreased")
28
Clinical Case PaCO 2 = 55 torr at 18/5: IATROGENIC HYPERCAPNIA secondary to ventilation at “flattened” portion of the P-V relationship After Dual Wean, PaCO 2 will be lowered provided ventilation is occurring closer to total lung capacity. Subsequent weaning to 14/4 may result in a PaCO 2 = 55 torr PERMISSIVE HYPERCAPNIA

29
4 5 17 18 TLC RV 19 16 P P V V PRESSURE (cmH 2 0) VOLUME Peak Inflating Pressure PEEP Iatrogenic hypercapnia with inappropriate Dual Wean Tidal Volume decreases with weaning
 VOLUME Peak Inflating Pressure PEEP Iatrogenic hypercapnia with inappropriate Dual Wean Tidal Volume decreases with weaning")
Similar presentations