Download presentation
Presentation is loading. Please wait.

2
2008 Guidelines 2.4 DIAGNOSIS IN ADULTS (1) -based on the recognition of a characteristic pattern of symptoms and signs and the absence of an alternative explanation for them -the key is to take a careful clinical history -if asthma is a likely diagnosis, the history should explore possible causes, particularly occupational -even in relatively clear-cut cases, to try to obtain objective support for the diagnosis
 -based on the recognition of a characteristic pattern of symptoms and signs and the absence of an alternative explanation for them -the key is to take a careful clinical history -if asthma is a likely diagnosis, the history should explore possible causes, particularly occupational -even in relatively clear-cut cases, to try to obtain objective support for the diagnosis")
3
2008 Guidelines 2.4 DIAGNOSIS IN ADULTS (2) -whether or not this should happen before starting treatment depends on the certainty of the initial diagnosis and the severity of presenting symptoms -repeated assessment and measurement may be necessary before confirmatory evidence is acquired.
 -whether or not this should happen before starting treatment depends on the certainty of the initial diagnosis and the severity of presenting symptoms -repeated assessment and measurement may be necessary before confirmatory evidence is acquired.")
4
2008 Guidelines 2.4 DIAGNOSIS IN ADULTS (3) Confirmation hinges on demonstration of airflow obstruction varying over short periods of time Spirometry is preferable to measurement of peak expiratory flow because it allows clearer identification of airflow obstruction, and the results are less dependent on effort
 Confirmation hinges on demonstration of airflow obstruction varying over short periods of time Spirometry is preferable to measurement of peak expiratory flow because it allows clearer identification of airflow obstruction, and the results are less dependent on effort")
5
2008 Guidelines 2.4 DIAGNOSIS IN ADULTS (4) Spirometry should be the preferred test where available (training is required to obtain reliable recordings and to interpret the results) A normal spirogram (or PEF) obtained when the patient is not symptomatic does not exclude the diagnosis of asthma.
 Spirometry should be the preferred test where available (training is required to obtain reliable recordings and to interpret the results) A normal spirogram (or PEF) obtained when the patient is not symptomatic does not exclude the diagnosis of asthma.")
6
2008 Guidelines With airflow obstruction COPD Bronchiectasis* Inhaled foreign body* Obliterative bronchiolitis Large airway stenosis Lung cancer* Sarcoidosis* *may also be associated with non-obstructive spirometry Differential diagnosis of asthma in adults, according to the presence or absence of airflow obstruction (FEV1/FVC <0.7) Without airflow obstruction Chronic cough syndromes Hyperventilation syndrome Vocal cord dysfunction Rhinitis Gastro-oesophageal reflux Cardiac failure Pulmonary fibrosis
 Without airflow obstruction Chronic cough syndromes Hyperventilation syndrome Vocal cord dysfunction Rhinitis Gastro-oesophageal reflux Cardiac failure Pulmonary fibrosis")
7
7 ADULT with symptoms that may be due to asthma Clinical History and examination Spirometry (or PEF if spirometry not available) High Probability Low Probability Intermediate Probability Yes No Obstructive FEV/FVC <70% Manage according to alternative diagnosis Response? Investigate and treat alternative diagnosis Yes Trial of Treatment Response? Asthma diagnosis confirmed Continue Rx No Assess compliance and inhaler technique. Reconsider the diagnosis Consider further tests or referral Normal FEV/FVC >70% Reconsider probable diagnosis Further investigation

8
8 High Probability Patient with symptoms that may be due to asthma Clinical History and examination Spirometry (or PEF if spirometry not available) 1)Symptoms (cough, wheeze, SOB or chest tightness): worse at night and in the morning in response to exercise, allergen exposure and cold air after taking aspirin or beta blockers 2) History of atopic disease 3) Family history of asthma or atopic disease 4) Widespread wheeze 5) Evidence of airway narrowing (NB Normal spirometry when free of symptoms does not exclude asthma)
 1)Symptoms (cough, wheeze, SOB or chest tightness): worse at night and in the morning in response to exercise, allergen exposure and cold air after taking aspirin or beta blockers 2) History of atopic disease 3) Family history of asthma or atopic disease 4) Widespread wheeze 5) Evidence of airway narrowing (NB Normal spirometry when free of symptoms does not exclude asthma)")
9
9 Patient with symptoms that may be due to asthma Clinical History and examination Spirometry (or PEF if spirometry not available) High Probability Trial of Treatment Response? Asthma diagnosis confirmed Continue Rx Yes

10
10 Patient with symptoms that may be due to asthma Clinical History and examination Spirometry (or PEF if spirometry not available) High Probability Trial of Treatment Response? Asthma diagnosis confirmed Continue Rx Yes No Assess compliance and inhaler technique. Reconsider the diagnosis Consider further tests or referral

11
11 Patient with symptoms that may be due to asthma Clinical History and examination Spirometry (or PEF if spirometry not available) High Probability Trial of Treatment Response? Asthma diagnosis confirmed Continue Rx YesNo Assess compliance and inhaler technique. Reconsider the diagnosis Consider further tests or referral Low probability equals: 1)Cough in the absence of wheeze or breathlessness 2)Prominent dizziness, light headedness, peripheral tingling 3)Repeatedly normal clinical examination even when symptomatic 4)No evidence of airway narrowing when symptomatic 5)Voice disturbance 6)Symptoms with colds only 7)Chronic productive cough 8)Significant smoking history (>20 pack years) 9)Cardiac disease Low Probability
Cough in the absence of wheeze or breathlessness 2)Prominent dizziness, light headedness, peripheral tingling 3)Repeatedly normal clinical examination even when symptomatic 4)No evidence of airway narrowing when symptomatic 5)Voice disturbance 6)Symptoms with colds only 7)Chronic productive cough 8)Significant smoking history (>20 pack years) 9)Cardiac disease Low Probability.")
12
12 Patient with symptoms that may be due to asthma Clinical History and examination Spirometry (or PEF if spirometry not available) High Probability Trial of Treatment Response? Asthma diagnosis confirmed Continue Rx YesNo Assess compliance and inhaler technique. Reconsider the diagnosis Consider further tests or referral Low Probability Manage according to alternative diagnosis Investigate and treat alternative diagnosis Response? Yes

13
13 Patient with symptoms that may be due to asthma Clinical History and examination Spirometry (or PEF if spirometry not available) High Probability Trial of Treatment Response? Asthma diagnosis confirmed Continue Rx YesNo Assess compliance and inhaler technique. Reconsider the diagnosis Consider further tests or referral Low Probability Manage according to alternative diagnosis Response? Investigate and treat alternative diagnosis Yes Reconsider probable diagnosis Further investigation No

14
14 Patient with symptoms that may be due to asthma Clinical History and examination Spirometry (or PEF if spirometry not available) High Probability Trial of Treatment Response? Asthma diagnosis confirmed Continue Rx YesNo Assess compliance and inhaler technique. Reconsider the diagnosis Consider further tests or referral Low Probability Manage according to alternative diagnosis Response? Investigate and treat alternative diagnosis Yes Reconsider probable diagnosis Further investigation No Intermediate Probability Obstructive FEV/FVC <70% Normal FEV/FVC >70%

15
15 Patient with symptoms that may be due to asthma Clinical History and examination Spirometry (or PEF if spirometry not available) High Probability Low Probability Manage according to alternative diagnosis Response? Investigate and treat alternative diagnosis Yes Reconsider probable diagnosis Further investigation No Intermediate Probability Obstructive FEV/FVC <70% Normal FEV/FVC >70% Trial of Treatment Response? Asthma diagnosis confirmed Continue Rx YesNo Assess compliance and inhaler technique. Reconsider the diagnosis Consider further tests or referral

16
16 Trial of Treatment Response? Asthma diagnosis confirmed Continue Rx YesNo Assess compliance and inhaler technique. Reconsider the diagnosis Consider further tests or referral Patient with symptoms that may be due to asthma Clinical History and examination Spirometry (or PEF if spirometry not available) High Probability Low Probability Manage according to alternative diagnosis Response? Investigate and treat alternative diagnosis YesNo Intermediate Probability Obstructive FEV/FVC <70% Normal FEV/FVC >70% Reconsider probable diagnosis Further investigation
 High Probability Low Probability Manage according to alternative diagnosis Response. Investigate and treat alternative diagnosis YesNo Intermediate Probability Obstructive FEV/FVC <70% Normal FEV/FVC >70% Reconsider probable diagnosis Further investigation.")
17
© Imperial College LondonPage 17 Assessment: Royal College of Physicians of London three questions Outcomes and audit. Thorax 2003; 58 (Suppl I): i1-i92 Applies to all patients with asthma aged 16 and over. Only use after diagnosis has been established. IN THE LAST WEEK / MONTH YES NO “Have you had difficulty sleeping because of your asthma symptoms (including cough)?” “Have you had your usual asthma symptoms during the day (cough, wheeze, chest tightness or breathlessness)?” “Has your asthma interfered with your usual activities (e.g. housework, work, school, etc)?” Date / / /
: i1-i92 Applies to all patients with asthma aged 16 and over. Only use after diagnosis has been established. IN THE LAST WEEK / MONTH YES NO Have you had difficulty sleeping because of your asthma symptoms (including cough) Have you had your usual asthma symptoms during the day (cough, wheeze, chest tightness or breathlessness) Has your asthma interfered with your usual activities (e.g. housework, work, school, etc) Date / / /.")
18
1.In the past 4 weeks, how much of the time did your asthma keep you from getting as much done at work, school or at home? 2.During the past 4 weeks, how often have you had shortness of breath? 3.During the past 4 weeks, how often did your asthma symptoms (wheezing, coughing, shortness of breath, chest tightness or pain) wake you up at night, or earlier than usual in the morning? 4.During the past 4 weeks, how often have you used your rescue inhaler or nebulizer medication (such as salbutamol)? 5.How would you rate your asthma control during the past 4 weeks? Score Patient Total Score Copyright 2002, QualityMetric Incorporated. Asthma Control Test Is a Trademark of QualityMetric Incorporated. Asthma Control Test™ (ACT)
 wake you up at night, or earlier than usual in the morning. 4.During the past 4 weeks, how often have you used your rescue inhaler or nebulizer medication (such as salbutamol). 5.How would you rate your asthma control during the past 4 weeks. Score Patient Total Score Copyright 2002, QualityMetric Incorporated. Asthma Control Test Is a Trademark of QualityMetric Incorporated. Asthma Control Test™ (ACT).")
19
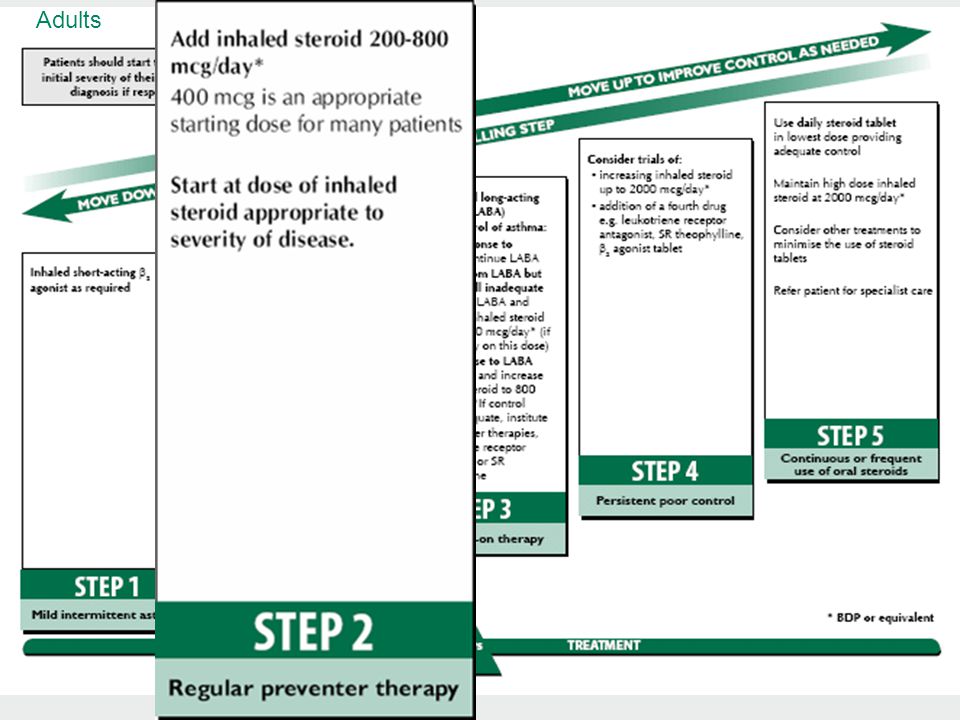
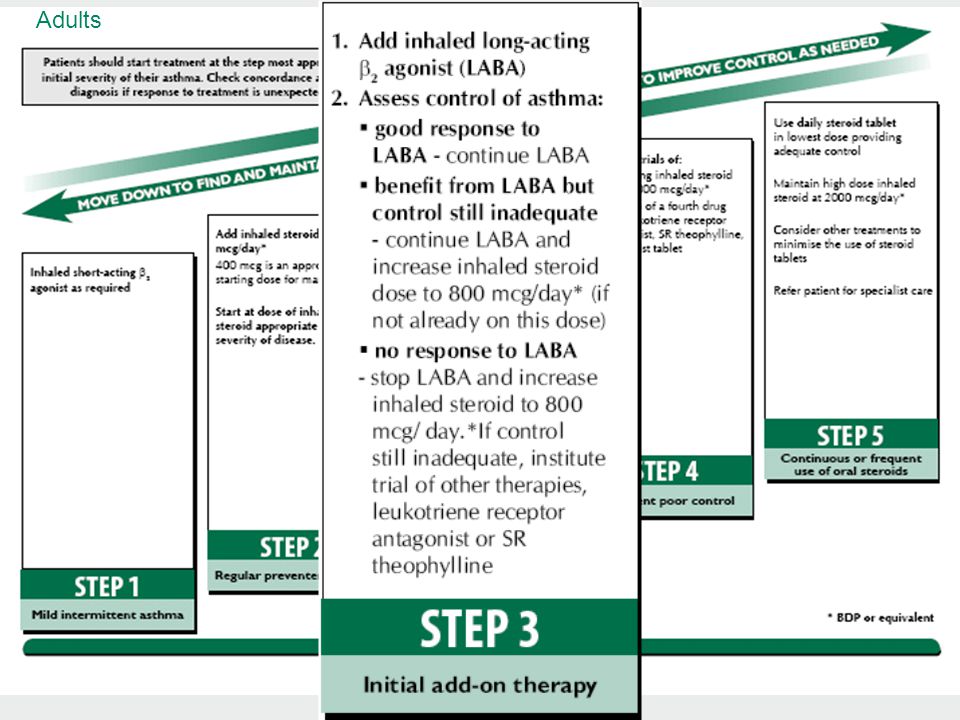
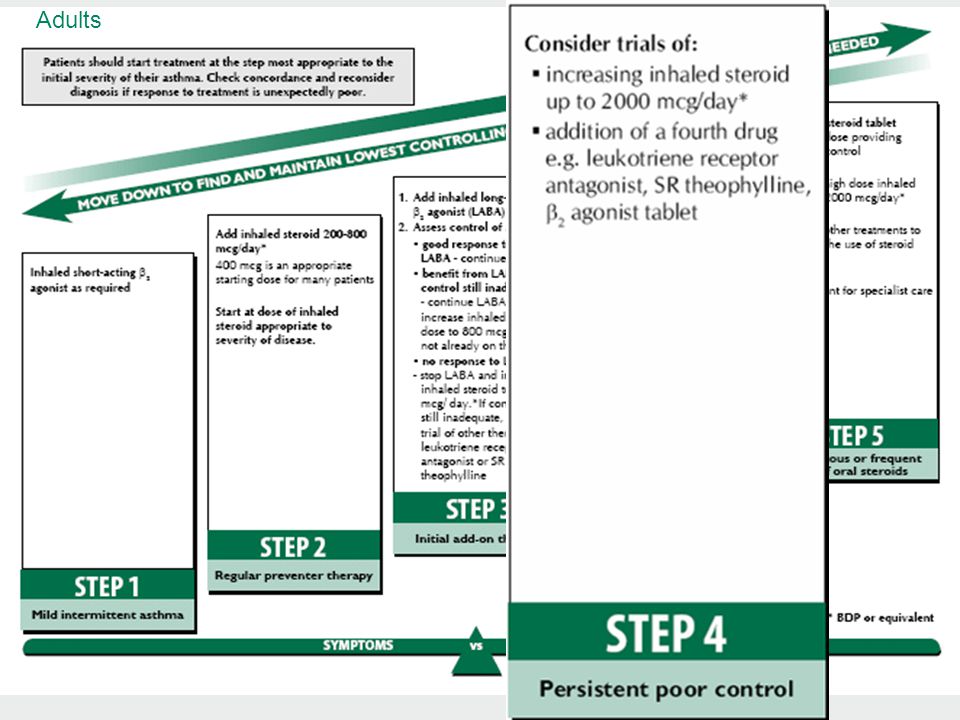
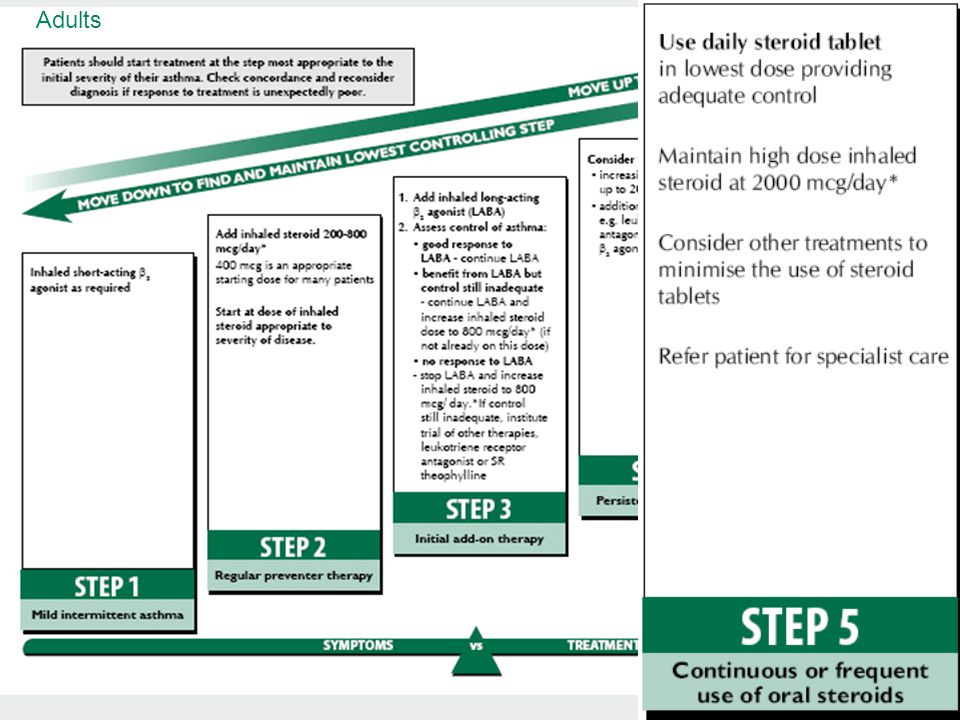
Adults

25
www.sign.ac.uk/guidelines/fulltext/102/index.html
Similar presentations




 Airway.>")






 With atria and blood vessels on for.>")
 Diagnosis and management of chronic asthma in line with current BTS guidelines (Dr Lowery) 3 x Case.>")







