Download presentation
Presentation is loading. Please wait.

1
Clare Alexander RSCH March 2015
Asthma Update Clare Alexander RSCH March 2015

2
Asthma update What is asthma (spirometry) BTS guidelines
National review of Asthma deaths Diagnostic pitfalls

4
What is Asthma Est. 3.4 million people have Asthma in the UK
Variable, reversible airways obstruction Est. 3.4 million people have Asthma in the UK Bronchoconstriction Inflammatory cellular infiltrate Mucus

5
Spirometry Method of assessing lung function - patterns
How much “puff”/ “breath” you have = FVC (Forced vital capacity How quickly you can force your breath out – i.e. how much resistance? = FEV1 (Volume (litres) of air expelled in first second of forced expiration Ratio between resistance or obstruction and the amount of available “breath” – disease patterns = FEV1/ FVC or FEV1 ratio
 of air expelled in first second of forced expiration. Ratio between resistance or obstruction and the amount of available breath – disease patterns. = FEV1/ FVC or FEV1 ratio.")
6
British Thoracic Society (BTS)
Scottish Intercollegiate Guidelines Network (SIGN) Revised guideline October 2014
 Revised guideline October")
9
Aim of Asthma Management
Complete control - defined as: No daytime symptoms No night time wakening due to asthma No need for rescue medication No asthma attacks No exacerbations No limitations on activity including exercise Normal lung function (FEV1 +/ or PEF> 80% predicted or best) Minimal side effects from medication
 Minimal side effects from medication.")
10
Treatment strategies Supported Self Management
Non- pharmacological Management Pharmacological Management Adherence and Concordance Difficult Asthma Work related Asthma

11
Supported Self Management
Incorporating written personalised asthma action plans (PAAPs) (traffic lights) Based on symptoms +/or PEFRs Supported by regular professional review Education – linked to patient goals E.g. Trigger avoidance such as animals, smoking Trained professionals Culturally appropriate In patients should all receive/ had reviewed PAAPs
 (traffic lights) Based on symptoms +/or PEFRs. Supported by regular professional review. Education – linked to patient goals. E.g. Trigger avoidance such as animals, smoking. Trained professionals. Culturally appropriate. In patients should all receive/ had reviewed PAAPs.")
13
Asthma Control Test™ (ACT)
In the past 4 weeks, how much of the time did your asthma keep you from getting as much done at work, school or at home? Score During the past 4 weeks, how often have you had shortness of breath? During the past 4 weeks, how often did your asthma symptoms (wheezing, coughing, shortness of breath, chest tightness or pain) wake you up at night, or earlier than usual in the morning? During the past 4 weeks, how often have you used your rescue inhaler or nebulizer medication (such as salbutamol)? How would you rate your asthma control during the past 4 weeks? EDUCATION! Copyright 2002, QualityMetric Incorporated. Asthma Control Test Is a Trademark of QualityMetric Incorporated. Patient Total Score
 wake you up at night, or earlier than usual in the morning During the past 4 weeks, how often have you used your rescue inhaler or nebulizer medication (such as salbutamol) How would you rate your asthma control during the past 4 weeks EDUCATION! Copyright 2002, QualityMetric Incorporated. Asthma Control Test Is a Trademark of QualityMetric Incorporated. Patient Total Score.")
14
Non- pharmacological Management
Smoking advice and support Weight loss in overweight patients Breathing exercise programs (often Physiotherapy lead, RSCH) – “dysfunctional breathing patterns” or hyperventilation. NIJEMEN questionnaire Exercise Do not recommend Physical and chemical methods to reduce house dust mite – ineffective (& expensive). Diets of exclusion (e.g. milk, unless (rarely) clinically identified – immunologist)
 – dysfunctional breathing patterns or hyperventilation. NIJEMEN questionnaire. Exercise. Do not recommend. Physical and chemical methods to reduce house dust mite – ineffective (& expensive). Diets of exclusion (e.g. milk, unless (rarely) clinically identified – immunologist)")
15
Pharmacological Management
The Stepwise Approach Start treatment at the step most appropriate to initial severity Achieve early control Maintain control by: Stepping up as necessary Stepping down when control good Before initiating new drug therapy, check – adherence with existing therapies; inhaler technique & eliminate trigger factors

16
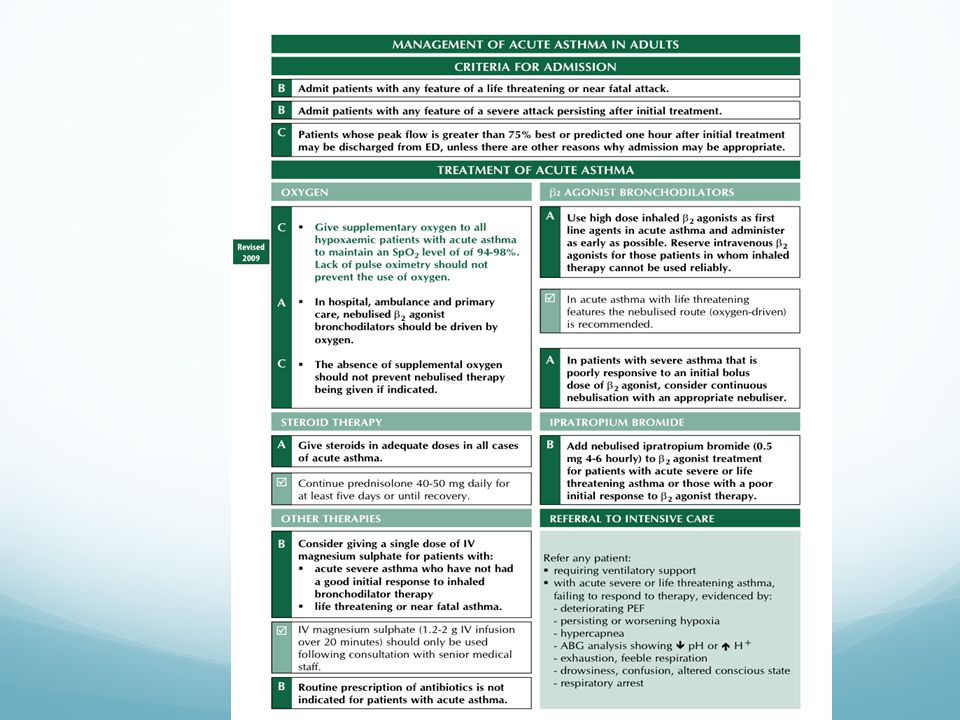
Adults Reference British Thoracic Society, Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma: A National Clinical Guideline. Revised Edition, 2008. 16

17
Adults Reference British Thoracic Society, Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma: A National Clinical Guideline. Revised Edition, 2008. 17

18
Adults Reference British Thoracic Society, Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma: A National Clinical Guideline. Revised Edition, 2008. 18

19
Adults Reference British Thoracic Society, Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma: A National Clinical Guideline. Revised Edition, 2008. 19

20
Adults Reference British Thoracic Society, Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma: A National Clinical Guideline. Revised Edition, 2008. 20

21
Pharmacological Management cont.
Combination inhalers recommended to Guarantee LABAs not taken without ICS Improve inhaler adherence Stepping down Severity of asthma, time on current dose, beneficial effects achieved & pts preference Slowly – every 3 months – % dose each time Exercise induced asthma – most patients represents poorly controlled asthma SABA immediately prior to exercise Avoid prescribing different inhaler types i.e. powder devices vs aerosols.

22
Adherence and Concordance
Routinely & regularly addressed (accessible pro-active asthma care) Computer repeat- prescribing systems (practical index) Non- judgmental discussions
 Computer repeat- prescribing systems (practical index) Non- judgmental discussions.")
23
Alternative diagnosis OR Severe/ Brittle
Difficult Asthma Alternative diagnosis OR Severe/ Brittle e.g. COPD Bronchiectasis GO reflux Cardiac failure Compliance Symptoms out of proportion Dysfunctional breathing Asthma not responding to maximum treatment Symptomatic at BTS/Sign step 4/5

25
Work related Asthma (& Rhinitis)
At least 1 in 10 cases of new or reappearance of childhood asthma in adult life are attributed to occupation. Nasal symptoms Prognosis of Ig-E associated occupational asthma improved by early identification and avoidance. Objective measures (PEFR at least 4x day) – specialist referrals High risk Baking, spray paint, lab animals, health & dental care, food processing, metal / wood/ plastics/rubber, farming + dust
 – specialist referrals. High risk. Baking, spray paint, lab animals, health & dental care, food processing, metal / wood/ plastics/rubber, farming + dust.")
28
National Review of Asthma Deaths NRAD (2014)
Commissioned by: Healthcare Quality Improvement Partnership (HQIP) On behalf of: NHS England, NHS Wales, Health and Social Care Division of the Scottish Government, Northern Ireland Department of Health Social Services and Public Safety Delivered by: Clinical Effectiveness and Evaluation Unit of the Clinical Standards Department of the Royal College of Physicians
 On behalf of: NHS England, NHS Wales, Health and Social Care Division of the Scottish Government, Northern Ireland Department of Health Social Services and Public Safety. Delivered by: Clinical Effectiveness and Evaluation Unit of the Clinical Standards Department of the Royal College of Physicians.")
29
Overall aim of NRAD To understand the circumstances surrounding asthma deaths in the UK, in order to identify avoidable factors and make recommendations for changes to improve asthma care as well as patient self- management (This was not a prevalence study – did not aim to determine the number of asthma deaths in the UK)
")
30
NRAD A multidisciplinary, confidential enquiry of asthma deaths in Feb Jan 2013 in the UK effectiveness of the management of asthma (acute and chronic) Identify potential avoidable factors Make recommendations for changes - to reduce the number of preventable asthma deaths The aim of the NRAD was to understand the circumstances surrounding asthma deaths in the UK, in order to identify avoidable factors and make recommendations for changes to improve asthma care as well as patient self-management. Objectives 1 Conduct a multidisciplinary, confidential enquiry to investigate the circumstances and clarify the cause of death in those people meeting the study inclusion criteria. 2 Examine the effectiveness of the management of asthma by reviewing the quality of care during the fatal attack, as well as previous treatment, against standards derived principally from the British Thoracic Society/Scottish Intercollegiate Guidelines Network (BTS/SIGN) British Guideline on the Management of Asthma (2012).1 3 Identify potentially avoidable factors related to the circumstances of those asthma deaths. 4 Make recommendations for changes in clinical management in order to reduce the number of preventable deaths from asthma in the future. 5 Understand the effect of asthma and death from asthma on families and carers of people with asthma by interviewing bereaved relatives on their experiences of the care provided to the family member who died.
 Identify potential avoidable factors. Make recommendations for changes - to reduce the number of preventable asthma deaths. The aim of the NRAD was to understand the circumstances surrounding asthma deaths in the UK, in. order to identify avoidable factors and make recommendations for changes to improve asthma care as. well as patient self-management. Objectives. 1 Conduct a multidisciplinary, confidential enquiry to investigate the circumstances and clarify the cause. of death in those people meeting the study inclusion criteria. 2 Examine the effectiveness of the management of asthma by reviewing the quality of care during the. fatal attack, as well as previous treatment, against standards derived principally from the British. Thoracic Society/Scottish Intercollegiate Guidelines Network (BTS/SIGN) British Guideline on the. Management of Asthma (2012).1. 3 Identify potentially avoidable factors related to the circumstances of those asthma deaths. 4 Make recommendations for changes in clinical management in order to reduce the number of. preventable deaths from asthma in the future. 5 Understand the effect of asthma and death from asthma on families and carers of people with asthma. by interviewing bereaved relatives on their experiences of the care provided to the family member who. died.")
31
NRAD Method Analysis of 195 people who died from asthma
374 local coordinators 297 hospitals 174 expert clinical assessors (primary and secondary care)
")
32
Location of Death

33
Patient Demographics Duration of asthma (n=104) : 0-62 yrs (11 yrs)
Age at diagnosis (n=102) : mths – 90 yrs (37 yrs) Age at death (n=193) : yrs – 97 yrs (58 yrs) Severity of asthma (n=155): (classified by the Clinicians) Mild (9%) Moderate (49%) Severe 61 (39%) ‘Amount of treatment required to gain control of the asthma’ It is possible that many of those cases defined by their doctors as Mild or Moderate ….. were more severe
 : 10 mths – 90 yrs (37 yrs) Age at death (n=193) : 4 yrs – 97 yrs (58 yrs) Severity of asthma (n=155): (classified by the Clinicians) Mild 14 (9%) Moderate 76 (49%) Severe 61 (39%) ‘Amount of treatment required to gain control of the asthma’ It is possible that many of those cases defined by their doctors as Mild or Moderate ….. were more severe.")
34
Key Findings & Recommendations
Use of NHS services Medical and professional care Prescribing and medicines use

35
Key Findings - use of NHS Services
87 of the 195 (45%) died without seeking medical help or before emergency care could be provided 112 (57%) were not recorded as being under specialist supervision There was a history of previous hospital admission in 47% 19 (10%) died within 28 days of discharge from hospital
 died without seeking medical help or before emergency care could be provided. 112 (57%) were not recorded as being under specialist supervision. There was a history of previous hospital admission in 47% 19 (10%) died within 28 days of discharge from hospital.")
36
Primary care review of the 195 cases (in the 12 months before death)
64 (33%) - no details on asthma diagnosis 70/ diagnosed > age of 15 ? Late onset; ? Delayed diagnosis; ? Recurrence 84 (43%) - no record of asthma review 12 mths 37 (19%) - had assessment of asthma control 44 (23%) - had Personal Asthma Action Plans (PAAP) 112 (57%) - not under specialist supervision One-hundred (51%) of the 195 patients that died were diagnosed on the basis of recurrent symptoms, 34 (17%) on physiological measurement of lung function, and 66 (34%) on the response to asthma medication. The basis for diagnosing asthma was not detailed in 64 (33%).
 - no details on asthma diagnosis. 70/102 - diagnosed > age of 15. Late onset; Delayed diagnosis; Recurrence. 84 (43%) - no record of asthma review 12 mths. 37 (19%) - had assessment of asthma control. 44 (23%) - had Personal Asthma Action Plans (PAAP) 112 (57%) - not under specialist supervision. One-hundred (51%) of the 195 patients that died were diagnosed on the basis of recurrent symptoms, 34 (17%) on physiological measurement of lung function, and 66 (34%) on the response to asthma medication. The basis for diagnosing asthma was not detailed in 64 (33%).")
37
Key Findings - Medical and Professional Care
The majority of people (58%) who died were thought to have mild or moderate asthma Avoidable factors were identified in 89 (46%) deaths Exacerbating factors, or triggers, were documented in only half the people who died
 who died were thought to have mild or moderate asthma. Avoidable factors were identified in 89 (46%) deaths. Exacerbating factors, or triggers, were documented in only half the people who died.")
38
Recommendations - Medical and Professional Care
All patients should have written guidance in the form of a personal asthma action plans (PAAP), describing triggers, how to prevent relapse and emergency action Triggers and avoidable factors should be actively sought, and appropriate action taken Management plans should reflect that the risk of asthma death is increased where there is significant concurrent psychological and mental health issues All patients with asthma should have a regular structured review, undertaken at least annually
, describing triggers, how to prevent relapse and emergency action. Triggers and avoidable factors should be actively sought, and appropriate action taken. Management plans should reflect that the risk of asthma death is increased where there is significant concurrent psychological and mental health issues. All patients with asthma should have a regular structured review, undertaken at least annually.")
39
Recommendations - Patient factors, awareness of risk of poor control
Patient self-management should be encouraged to reflect exposure to known triggers eg before hay fever season History of smoking and/or exposure to passive smoke should be documented. Current smokers should be offered referral to a smoking cessation service Parents and children should be educated on the ‘how’, ‘why’ and ‘when’ to use their asthma medications and know how to seek emergency help

40
Key Findings - Prescribing and medicines use
There was evidence of excessive prescribing of relievers, 6 patients being prescribed more than 50 short acting reliever inhalers in the year before death There was strong evidence of under prescribing of preventer medications (ICS) There appeared to be inappropriate prescribing of long- acting beta agonist, either as a single agent without inhaled corticosteroid
 There appeared to be inappropriate prescribing of long- acting beta agonist, either as a single agent without inhaled corticosteroid.")
41
Excessive prescribing of Short Acting Beta-Agonist Bronchodilators (SABAs) (n= 189/194 ; 97%)
Excess need for reliever medication (SIGN/BTS) = Poor asthma control Numbers of devices prescribed during final year (n=165) Range: 1 to 112; median of 10 inhaler devices > 6 SABA : 92/165 (56%) inhaler devices > 12 SABA : 65/165 (39%) inhaler devices >50 SABA : 6 patients From available information on 194 of the 195 cases who died, 189 (97%) were recorded as having SABAs prescribed at the time of death. Of these 189, there were 165 for whom the number of prescriptions authorised for SABA was recorded within the last year, and of these 3 were recorded as zero. For the 162 with one or more within the last year the number of prescribed devices ranged from 1 to 112, with a median of 10 (IQR 3,21) inhalers per year. Ninety two (57%) of the 162 were prescribed more than six SABA inhalers and 65 (40%) more
 = Poor asthma control. Numbers of devices prescribed during final year (n=165) Range: 1 to 112; median of 10 inhaler devices. > 6 SABA : 92/165 (56%) inhaler devices. > 12 SABA : 65/165 (39%) inhaler devices. >50 SABA : 6 patients. From available information on 194 of the 195 cases who died, 189 (97%) were recorded as having SABAs prescribed at the time of death. Of these 189, there were 165 for whom the number of prescriptions authorised for SABA was recorded within the last year, and of these 3 were recorded as zero. For the 162 with one or more within the last year the number of prescribed devices ranged from 1 to 112, with a median of 10 (IQR 3,21) inhalers per year. Ninety two (57%) of the 162 were prescribed more than six SABA inhalers and 65 (40%) more.")
42
Inadequate prescribing of Inhaled Corticosteroids (ICS) ICS +/- Long Acting Beta-agonist Bronchodilator (ICS/LABA) (n= 168/195 ; 86%) Number of prescribed devices final year (n=128): Range: 1 to 54, median of 5 inhaler devices < 4 ICS devices in 12 mths : 49/128 (38%) < 12 ICS devices in 12 mths : 103/128 (80%) From available information, 168 (86%) of the 195 that died from asthma had repeat prescriptions authorised for inhalers containing inhaled corticosteroids, either as ‘stand alone’ ICS and / or as combination ICS/LABA inhalers at the time of death. Conversely, 26 (13%) of the 195 cases were not prescribed any preventer medication at all in their final year, with insufficient information for the remaining 1 case. Depending on the dose of medication and device prescribed patients would normally need about 12 ICS or ICS / LABA combination inhaler devices a year, in order to adhere to advice on daily medication use. For 128 of the 168 cases the number prescribed ICS alone and the number prescribed combination ICS / LABA inhalers in the 12 months before they died were both known. These 128 cases were prescribed a median of five inhalers IQR (2,10), and the numbers of inhalers prescribed for cases ranged from one to 54 inhalers in the twelve months. Forty nine (38%) of these 128 cases had been issued (and presumably collected) less than four prescriptions for these inhaler devices in the 12 months before death, and 103 (80%) were prescribed less than 12 inhalers, and as most ICS or ICS / LABA combination inhalers last for 1 month at standard doses, the majority of cases were therefore undertreated and had only partially adhered to medical advice.
: Range: 1 to 54, median of 5 inhaler devices. < 4 ICS devices in 12 mths : 49/128 (38%) < 12 ICS devices in 12 mths : 103/128 (80%) From available information, 168 (86%) of the 195 that died from asthma had repeat prescriptions authorised for inhalers containing inhaled corticosteroids, either as ‘stand alone’ ICS and / or as combination ICS/LABA inhalers at the time of death. Conversely, 26 (13%) of the 195 cases were not prescribed any preventer medication at all in their final year, with insufficient information for the remaining 1 case. Depending on the dose of medication and device prescribed patients would normally need about 12 ICS or ICS / LABA combination inhaler devices a year, in order to adhere to advice on daily medication use. For 128 of the 168 cases the number prescribed ICS alone and the number prescribed combination ICS / LABA inhalers in the 12 months before they died were both known. These 128 cases were prescribed a median of five inhalers IQR (2,10), and the numbers of inhalers prescribed for cases ranged from one to 54 inhalers in the twelve months. Forty nine (38%) of these 128 cases had been issued (and presumably collected) less than four prescriptions for these inhaler devices in the 12 months before death, and 103 (80%) were prescribed less than 12 inhalers, and as most ICS or ICS / LABA combination inhalers last for 1 month at standard doses, the majority of cases were therefore undertreated and had only partially adhered to medical advice.")
43
Recommendations - Prescribing and medicines use
People with asthma who have been prescribed more than 12 short-acting reliever inhalers in the past 12 months should be invited for urgent review Non-adherence with preventer inhaled corticosteroid should be monitored Use of combination inhalers should be encouraged Assessment of inhaler technique should be made at annual review and by the pharmacist whenever new inhaled devices are prescribed

44
Recommendations - use of NHS Services
Every NHS hospital and general practice should have a designated lead for asthma service Follow up must be undertaken after every attendance at the emergency department or out-of-hours service A standard national template should be developed to facilitate a structured review Electronic systems should be developed urgently to alert clinicians to over use of short acting relievers or underuse of preventers

45
Major factors identified by panels (i. e
Major factors identified by panels (i.e. contributed significantly to the deaths, where different management would reasonably be expected to have affected the outcome ) n Did not recognise high-risk status 21 Lack of specific asthma expertise 17 Did not perform adequate asthma review 16 Did not refer to another appropriate team member Failure to take appropriate medication in month before death 15 Failure to take appropriate medication in year before death 13 Over prescribed short acting beta agonist bronchodilator 13 Poor or inadequate implementation of policy/pathway/protocol Lack of knowledge of guidelines 12 Did not adhere to medical advice 10
 n. Did not recognise high-risk status. 21. Lack of specific asthma expertise. 17. Did not perform adequate asthma review. 16. Did not refer to another appropriate team member. Failure to take appropriate medication in month before death. 15. Failure to take appropriate medication in year before death. 13 Over prescribed short acting beta agonist bronchodilator. 13. Poor or inadequate implementation of policy/pathway/protocol. Lack of knowledge of guidelines. 12. Did not adhere to medical advice. 10.")
47
Differential Diagnosis & Diagnostic pitfalls
Bronchiectasis (normal, obstructive or restrictive spirometry) Vocal cord dysfunction (+/- normal spirometry at rest) COPD – smoking > 20years (fixed obstructive spirometry) Pulmonary fibrosis – progressive SOB and cough – HRCT scan (restrictive spirometry) Cardiac failure (restrictive spirometry)
 Vocal cord dysfunction (+/- normal spirometry at rest) COPD – smoking > 20years (fixed obstructive spirometry) Pulmonary fibrosis – progressive SOB and cough – HRCT scan (restrictive spirometry) Cardiac failure (restrictive spirometry)")
48
Bronchiectasis “Wet cough” , hard “casts” sputum production
Recurrent infections Poorly controlled asthma High resolution CT Scan Aspergillus Precipitins (IgG) and Aspergillus specific IgE and total IgE – ABPA (Allergic bronchopulmonary aspergilosis) treatment with prolonged steroid (upto a year) plus itraconazole. Treatment – Physiotherapy and airways clearance. Bronchodilators Prophylactic Antibiotic (> 3-4 infections in a year)
 and Aspergillus specific IgE and total IgE – ABPA (Allergic bronchopulmonary aspergilosis) treatment with prolonged steroid (upto a year) plus itraconazole. Treatment – Physiotherapy and airways clearance. Bronchodilators. Prophylactic Antibiotic (> 3-4 infections in a year)")
Similar presentations







>")
 Airway.>")
 Asthma GP monitoring Guideline 2) Asthma Diagnosis Guideline 3) Acute asthma.>")
>")
 -based on the recognition of a characteristic pattern of symptoms and signs and the absence of an alternative.>")


 By Chris Callan 23 April 2008.>")





 Diagnosis and management of chronic asthma in line with current BTS guidelines (Dr Lowery) 3 x Case.>")




