Download presentation
Presentation is loading. Please wait.

1
Chronic Disease Management Respiratory & CKD Liz Borlase Brampton Medical Practice

2
Chronic Disease Management COPD starter question Respiratory practice nurses Role play Cases

3
Screening for COPD Should all smokers over 50 have spirometry to screen for COPD?

4
WHO screening guidelines an important health problem treatment should be available a latent stage of the disease a acceptable test or examination the natural history adequately understood an agreed policy on whom to treat economically balanced cost of finding a case case-finding should be a continuous process

5
Screening for COPD - USA During the past 4 weeks, how much of the time did you feel short of breath? Do you ever cough up any “stuff,” such as mucus or phlegm? In the last 12 months do you do less than you used to because of breathing problems?

6
BMJ Best Practice There are no data to show conclusively that screening spirometry is effective in directing management decisions or in improving COPD outcomes in patients who are identified before the development of significant symptoms. However, if COPD is diagnosed at an early stage and risk factors are eliminated, the rate of decline in lung function will dramatically decrease. Treatment is much more efficacious in the early stages of disease.

7
Do you want to speak to the man in charge, or the nurse who knows what’s going on?

8
Respiratory Practice Nurse For better or for worse….?

9
This house believes that having a respiratory practice nurse always benefits patients with asthma and/or COPD.

10
Role play with feedback

11
Possible CKD 3 Explain results Repeat eGFR, and do ACR Address CVD risk factors Lifestyle Avoid nephrotoxic meds ?contraception advice

12
CKD – NICE Guidelines July 2014 CKD new finding – repeat eGFR within 2w and again within 90d Accelerated progression eGFR: Sustained decrease 25% or more plus change in category within 12m Sustained decrease 15ml/min/1.73m² per year

13
CKD – NICE Guidelines July 2014 Refer: eGFR <30 (CKD 4) ACR >70 (unless due to DM and treated) ACR >30 plus haematuria Sustained decrease Resistant BP Suspected genetic cause or RAS
 ACR >70 (unless due to DM and treated) ACR >30 plus haematuria Sustained decrease Resistant BP Suspected genetic cause or RAS")
14
Case 1 M48y SOB and productive cough Asthma on salbutamol and Clenil Unable to complete sentences Wheezy, PEFR 350 (PrPEFR 622) Options? Immediate and long term plans?

15
SIGN guidelines Asthma – Oct 2014 Adults: Step 1 - salbutamol Step 2 - inh steroid Step 3 - LABA and/or inc dose inh steroid Step 4 - inc inh steroid or montelukast, SR theophylline etc Step 5 - oral steroid and refer

16
Case 2 M6y 3d cough at night Mother asking for another salbutamol inh Father had asthma PEFR 110 (PrPEFR 143) Chest clear Differential? Discussion with mother? Options?

17
SIGN guidelines Asthma – Oct 2014 Diagnosis in children. Increase probability: wheeze, cough etc at night or with triggers; personal or FH atopy; o/e wheeze, response to Tx Decrease probability: sx with colds only, cough only; moist cough; dizzy, lightheaded, tingling; chest repeatedly clear; normal PEFR; no response to Tx; features of alternative Dx.

18
SIGN guidelines Asthma – Oct 2014 Children 5-12y: Step 1 - salbutamol Step 2 - inh steroid Step 3 - LABA and/or inc dose inh steroid and montelukast or SR theophylline Step 4 - inc inh steroid Step 5 - oral steroid and refer

19
SIGN guidelines Asthma – Oct 2014 Children <5y: Step 1 - salbutamol Step 2 - inh steroid or montelukast Step 3 - add montelukast or inh steroid, refer <2y Step 4 - refer

20
Salbutamol inhaler 2 puffs qds prn Have you ever written this prescription? Is it a good prescription? If not, why not?

21
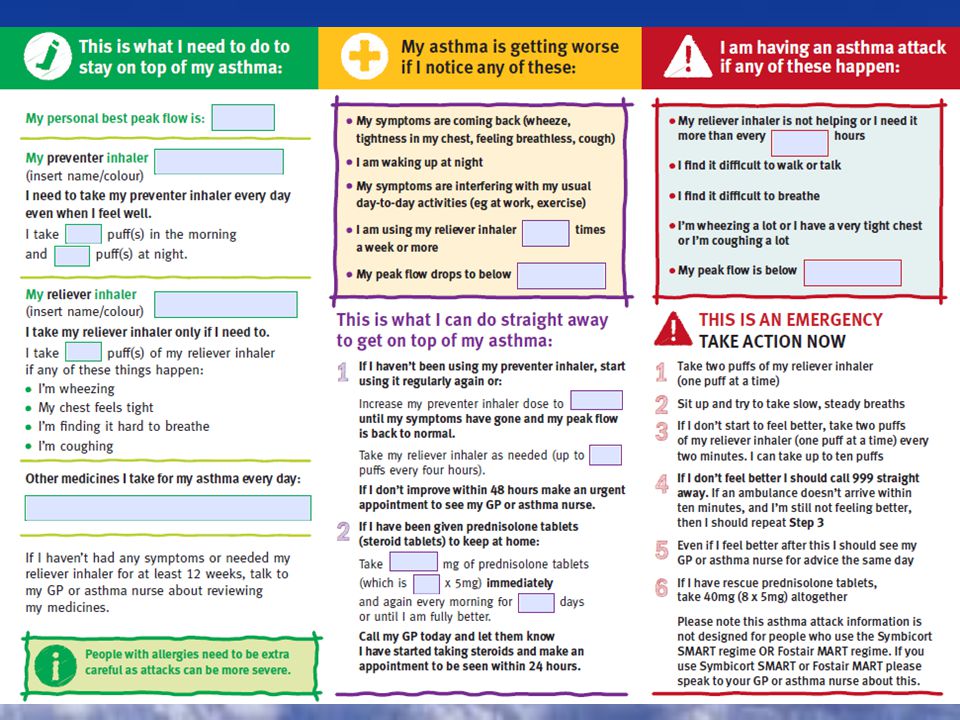
Asthma action plans What information do you give to your patients with asthma? http://www.asthma.org.uk/

24
Inhalers

25
Case 3 F67y 4d SOB and productive cough, tired and ankle swelling COPD, IHD, BP, hysterectomy, Colles, IBS, & OA salbutamol, tiotropium, aspirin, bisoprolol, ramipril, simvastatin, paracetamol, doublebase, citalopram P92, BP108/74, RR28, O2 91%, Wt 92kg, wheeze and creps throughout

26
Case 3 cont. Admission? Immediate plan? One week later, much better….. Discussion? Options?

27
NICE guidelines COPD – July 2014 Exacerbations Admit if: not coping, severe dyspnoea, confined to bed, cyanosis, worsening oedema, impaired consciousness, LTOT, acute confusion, co-morbidity, O2 < 90%, etc.

28
NICE guidelines COPD – July 2014 Diagnose: >35y, smoker and sx; then do spirometry Stop smoking Salbutamol; FEV1 > 50% then LABA or LAMA; FEV1 < 50% then LABA & ICS or LAMA. Pulmonary rehab

29
NICE guidelines COPD – July 2014 Consider LTOT if: FEV1 < 30% Cyanosis Polycythaemia Oedema Raised JVP O2 sats < 92%

30
HOOF forms Ask someone who knows! Part A only Consent form for new patients Capitals black ink, don’t miss anything marked ‘*’ Fax copy to ‘Air Liquide’, and respiratory nurses Add READ code to patient record New form for change in flow rate, hours or equipment Patient contacts ‘Air Liquide’ re holidays Letter on headed paper to remove equipment/supplies

31
Community COPD team Office hours, not rapid response Prevention of admission Supported discharge Pulmonary rehabilitation Ambulatory oxygen Patients not coming to surgery Education Inhalers, nebulisers, spirometry Oxygen concordance

Similar presentations

>")


 Airway.>")

>")


 -based on the recognition of a characteristic pattern of symptoms and signs and the absence of an alternative.>")



 By Chris Callan 23 April 2008.>")




 Professor Bill MacNee>")
 Diagnosis and management of chronic asthma in line with current BTS guidelines (Dr Lowery) 3 x Case.>")
