Download presentation
Presentation is loading. Please wait.

1
District General Hospital
CHRONIC ULCERS Dr.D.T.Gunasena MBBS,MS,FRCS(Edin) Consultant Surgeon District General Hospital Gampaha
 Consultant Surgeon. District General Hospital. Gampaha.")
2
Affects- 3.6% of older people over 65yrs
->5% in older people over 85yrs 10% of population develops chronic ulcers in the course of lifetime with wound related mortality of 2.5% 1/3 to ½ of Hospitalizations Do You Know ? In US 5.7 Million patients 20 Billion Dollars Annual Cost Neglected Lot

3
Incidence of chronic leg ulcers is rising……
Due to, Ageing population Increased Diabetes Mellitus Obesity Increased risk factors for Atheroslcerosis-Smoking -Obesity -etc…

4
In Sri Lanka……….. Insufficient information on the extent of the problem Underestimated size and gravity “Open Minds, Close Wounds” 2nd Meeting of the Asian Wound Healing Association held in Sept. 2014

5
Understanding of factors contribute to non-healing wounds
Aim Understanding of factors contribute to non-healing wounds Appropriate management Multidisciplinary team approach

6
Overview Types of wounds Wound healing –Phases Chronic Wounds
Identification and classification of chronic wounds Management of chronic wounds New advances in management of chronic wounds

7
History Prehistory Ebers Papyrus Circa 1500BC Use of Lint
Animal grease Honey Differentiation of Acute and Chronic wounds Silver to control bodily infections Galen of Pergamum a Greek Surgeon served Roman Gladiators Modern Medicine Ancient Egypt Greece

8
19th Century…………… With the advancement of Microbiology
Cellular Pathology 1847-Ignaz Sammelweis(Obstetrician)-Hand washing & cleanliness 1860-Joseph Lister-Carbolic acid(Phenol),45% reduction of mortality 1870-Robert Wood Johnson-Production of gauze & wound dressing treated with iodine 1886-Ernst Von Bergann-Heat sterilization of instruments, aseptic surgey 1898-Paul Leopold Friedrich-Wound excision, reduces infections 2oth Century-Polymer synthetics for wounds George Winter/Howard Maibach-Moist wound dressing
-Hand washing & cleanliness Joseph Lister-Carbolic acid(Phenol),45% reduction of mortality Robert Wood Johnson-Production of gauze & wound dressing treated with iodine Ernst Von Bergann-Heat sterilization of instruments, aseptic surgey Paul Leopold Friedrich-Wound excision, reduces infections. 2oth Century-Polymer synthetics for wounds. George Winter/Howard Maibach-Moist wound dressing.")
9
Aim is Healing without complications
Wounds Acute Wounds Cuts, Abrasions, Lacerations Contusions Puncture Skin flaps and Bites Chronic Wounds Fail to pass through normal healing process They passes through the normal healing process readily Any wound > 3/12 considered a chronic wound Aim is Healing without complications

10
How do wounds heal Haemostasis Inflammation Proliferation or
Granulation Remodelling or Maturation

11
Natural wound healing process

12
Normal Healing Process…

13
Chronic Wounds

14
Chronic Wounds Working Definition – wound lasting >3 months
Normal healing process impaired Arrest at different levels Remains at same stage without progressing to wound healing Often underlying cause remains undetected

15
Neutrophil Immigration
Chronic wounds The wound healing cascade impairs and arrests at different stages Hemostasis CHRONIC WOUND Platelet Aggregation Neutrophil Immigration Monocyte Immigration Granulation Re-epithelialization Wound Closure Scar Formation Remodeling Minutes Hours Days Weeks Months Years Time

16
Affects every aspect of life………
Debilitating disease Loss of productivity at home & work place Financial burden on patient’s family & country’s health care system Reduces quality of life-Pain -Foul odour -Discharges -Sleep impaired -Deformity & Disfigurement -Reduced mobility

17
Factors that impede wound healing
Local factors Inadequate blood supply Increased skin tension Poor surgical apposition Wound dehiscence Poor venous drainage Presence of foreign body and foreign body reactions Continued presence of micro-organisms & Infection Excess local mobility, such as over a joint Systemic factors Advancing age and general immobility Obesity Smoking Malnutrition Deficiency of vitamins and trace elements Systemic malignancy and terminal illness Chemotherapy and radiotherapy Immunosuppressant drugs, corticosteroids, anticoagulants Inherited neutrophil disorders, such as leucocyte adhesion deficiency Diabetes and CRF

18
Chronic Wounds Pressure Sores(PU) Venous Ulcers(VU)
Diabetic Wounds(DU) Venous Ulcers(VU) Pressure Sores(PU) Arterial Wounds (AU)
 Venous Ulcers(VU) Pressure Sores(PU) Arterial Wounds (AU)")
19
1.Diabetic Wounds In UK ,5-7% of people with Diabetes have diabetic foot ulcers In Europe, treatment cost of DFUs is 10 billion Euros per year Globally 370 million have Diabetes In every 20 second a lower limb is amputated due to DM Development of an infection in a foot ulcer increase the risk of hospitalization 55.7 times & amputation 155 times Most of Foot & Leg Amputations are due to Diabetic Wounds Amputation Diabetes Neuropathy Foot Ulcer Infection

20
A Growing Epidemic… The worldwide diabetic population is expected to grow from 171 million to 366 million by 2025 Foot complications are one of the most common complications in diabetic patients The lifetime risk of a diabetic foot ulcer (DFU) is 15% to 25% Approximately 15% of DFUs result in amputation
 is 15% to 25% Approximately 15% of DFUs result in amputation.")
21
Cost of Diabetes and Wound Care
$174 billion: Total costs of diagnosed diabetes in the United States in 20071 $20 billion: Chronic wounds cost health care systems annually2

22
Amputations are a serious predictor of death…

23
Diabetic Wounds Most of Foot & Leg Amputations are due to Diabetic Wounds Chronic ulcer in a diabetic patient, not primarily due to other causes Extrinsic causes: smoking, friction, burn Intrinsic causes: neuropathy, macrovascular and microvascular disease, immune dysfunction, deformity, reopened previous ulcer

24
Peripheral vascular disease occurs in 11% of diabetic patients
Co-Morbidity in DU Peripheral vascular disease occurs in 11% of diabetic patients Peripheral neuropathy occurs in 42% of diabetic patients PVD is associated with delayed ulcer healing and increased rates of amputation

25
2.Venous Ulcers An area of discontinuity of the epidermis, persisting for 4 weeks or more, occurring as a result of venous hypertension and calf muscle pump insufficiency

26
Reflux in deep veins in 50 t0 71%
Venous Ulcers Recurrence in 57% Reflux in deep veins in 50 t0 71% Prior DVT causes 95% of deep vein reflux

27
Diagnosis of Venous Ulcers
Location on the calf Bronzing (lipodermatosclerosis) Exclusion of arterial insufficiency by bounding DP pulses, or ABI > 0.8 Tend to be slow-healing (~90% heal by one year), irregular, and associated with edema and sloughing
 Exclusion of arterial insufficiency by bounding DP pulses, or ABI > 0.8. Tend to be slow-healing (~90% heal by one year), irregular, and associated with edema and sloughing.")
28
3.Pressure Sores Visible evidence of pathological interruption of blood flow to dermal tissues Chief cause: sustained pressure Most commonly over sacrum, hip

29
3.Pressure Sores

30
Pressure Ulcers: What Works
Must relieve pressure or it won’t heal. Must use moist dressing or it won’t heal.

31
4.Arterial Ulcers Tend to occur on distal areas
Diminished/absent pulses Punched-out appearance, or gangrene Requires either salvage revascularization, or amputation—usually the latter

32
Diagnosis: ABI ABI= LE systolic BP/Brachial art syst BP
ABI < 0.7 abnormal; < 0.4 unlikely to heal Can perform in FMC Values: normal; mild; moderate; < 0.4 severe

33
Differential Diagnosis
LOCATION CAUSE APPEARANCE PAIN PU DU Bony Prom Callus Pressure Neuropathy/trauma Crater Borders distinct Intermittent pain No or diminished pain, sensation VU AU Calf/ankle Distal points Venous Stasis Inadequate arterial flow Irregular Gangrene Little pain, intact sensation Constant pain

34
Management of Chronic Wounds

35
Patient Centered – dealing with person with a chronic wound
Holistic –Total care -Not only wound itself- need to address patient’s other needs, diseases, and psychosocial wellbeing Wound Care Plan (WCP) Inter-disciplinary Needs Participation of multitude of disciplines Overall strategy and scope of the treatment plan depends on patient’s condition, prognosis, and reversibility of the wound.
 Inter-disciplinary. Needs Participation of multitude of disciplines. Overall strategy and scope of the treatment plan depends on patient’s condition, prognosis, and reversibility of the wound.")
36
Basic elements in wound care plan
Different types of wounds need different management Cleanse Debris from the Wound Manage Exudate Promote Granulation and Epithelialization Treat Infections Minimize Discomfort

37
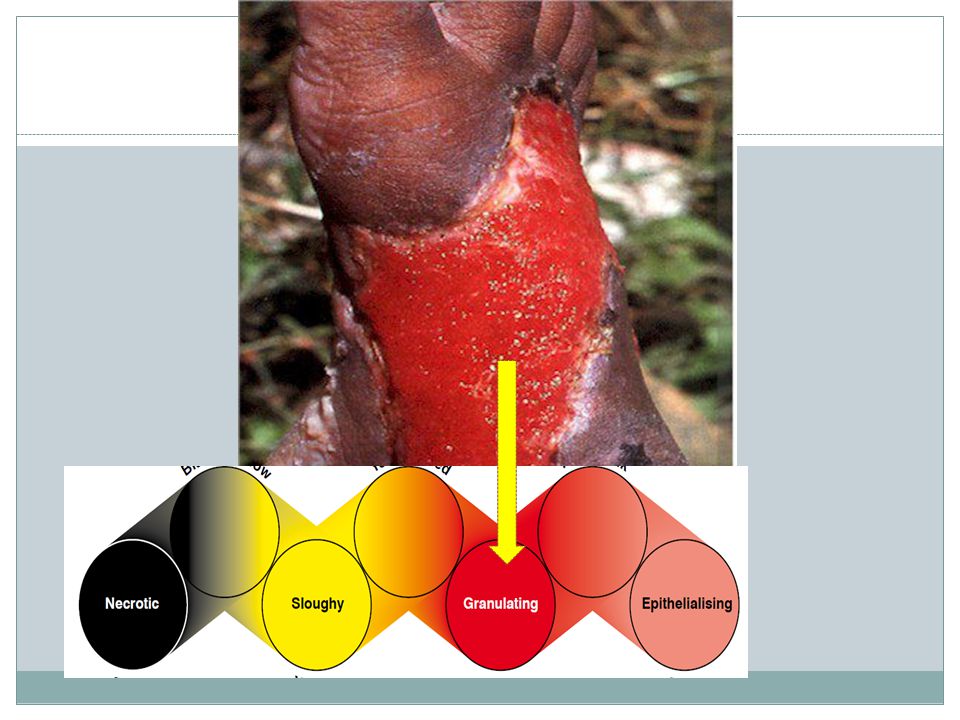
Chronic Wounds Appearance
approach has been criticised for being too simplistic as wound healing is a continuum and wounds often contain a mixture of tissue types.

38
Wound healing continuum
Wound Healing Continuum (Gray et al. 2005) have been developed. This tool incorporates intermediate colour combinations between the four key colours
 have. been developed. This tool incorporates intermediate colour combinations. between the four key colours.")
43
Cleanse Debris from the Wound
Cleansing agents Flowing Water –Requesting pt to bath before dressing change Normal Saline Commercial Cleansers Hydrogen Peroxide Povidone iodine Hypochlorite solution Sterile vinegar solution Mechanical Cleansers –Whirl pools Salt dips Aims Reduce bio burden Reduce dead and dying debris Clean the wound

44
Care of necrotic wound As areas of necrosis interfere with healing process, need to remove it through any of the following means Mechanical Debridement –Wet to dry dressings Autolytic Debridement- Occlusive dressing and wound exudate will debride by its enzymatic relations Enzymatic Debridement –By softening slough by using enzymes –Iruxol and Papaya Bio logical Debridement –Maggots therapy Surgical Debridement –Surgeons blades

45
Manage Exudates Identify the level of moisture
Manage exudates by dressings Nature of Exudate Type of wound Aim of exudate management Method /Agent No exudate Dry Keep the base moist Hydrocolloid agent Intrasite Need occlusive and non occlusive dressing Mild exudate Moist Keep the wound moist Absorb moisture Moderate Wet Keep the wound in moist state by reducing exudate Absorb moisture Form dressing Heavy Wet +++ Absorb

46
Care of granulating wounds
Care of granulation tissue – avoid dry or wet to dry dressings Prevent over granulation Prevent infection Minimal Dressing changes Exudate management and care of peri-wound area Skin grafting or skin substitutes

47
Care of infected wounds
Reduce bio burden –Cleansing, reduction of necrotic and sloughy tissue Local antiseptics – rotational Local antiseptics- cadexomer iodine, crystalline silver, PHMB Exudate management Care of peri-wound area

48
For spreading infection and or evidence of systemic infection
Antibiotics For spreading infection and or evidence of systemic infection Take blood cultures Treated with Broad Spectrum antibiotics intravenously. Topical antimicrobials - used to reduce wound bio burden (EWMA 2006).
.")
49
Minimize discomfort Pain relief Psychological support
Family education and create conducive environment Social support

50
Dressings

51
Advanced Treatment Modalities
Ultra Sound Debridement Negative Pressure Wound Therapy Growth Factor Therapy Pulsed Electromagnetic Wound Stimulation Live Skin Equivalent Grafting Hyperbaric Oxygen Maggots Therapy

52
Ultra Sound Debridement

53
Negative Pressure Wound Therapy

54
Growth Factor Therapy PDGF- based dressing

55
Pulsed Electromagnetic Wound Stimulation

56
Live Skin Equivalent Grafting

57
Hyperbaric Oxygen

58
Maggots therapy

59
Goals………….. Promote wound healing and achieve cure
Minimize amputations Prevention of recurrence Effective education reduces incidence of foot ulceration & amputation by over 50% Appropriate care planning goals for hospice patients may include: Preventing complications of the wound, such as infection or odor Of course, you will work to prevent additional breakdown of the skin We want to do our best to minimize harmful effects of the wound on the patient’s overall condition. This would be things like depression, social isolation or general discomfort. In many of our hospice patients, we know that promoting wound healing may be unrealistic. Therefore, let’s take a look at some specific interventions for wound care that might be more feasible.

60
Thank You Thank You

Similar presentations








 Closed wound: Skin is intact (not opened) include crushing injury and contusions. Wounds A) Skin involvement: 1) Open wound: when the whole thickness.>")


, However it is often misdiagnosed and mistreated.>")










