Download presentation
Presentation is loading. Please wait.

1
Peptic Ulcer Disease Khalayleh Harbi

2
Definition PUD is a disease of multiple etiology that characteristic of local gastric or duodenal damage and ulceration

3
Epidemiology The annual incidence in USA 1.8% or new cases per year. There are 4 million ulcer recurrences yearly. More than operation for PUD performed yearly. About 4000 patient die from complication of their PUD yearly

4
Pathogenesis Disbalance between aggressive factors and defenisive factors cause ulcer Protective factor (defensive) – mucous bicarbonate secretion ,blood flow, grwoth factors, cell renewal, endogenous prostaglandine Damaging(aggressive ) factors-HCL secretion, ethanol, smoking, reflux of bile, NSAID, hypoxia, HP
 – mucous bicarbonate secretion ,blood flow, grwoth factors, cell renewal, endogenous prostaglandine. Damaging(aggressive ) factors-HCL secretion, ethanol, smoking, reflux of bile, NSAID, hypoxia, HP.")
5
cause 1. H.PYLORI infection (most common cause)
2.NSAID (second most common cause) 3.stress 4. incrased pepsin and acid secretion
 3.stress. 4. incrased pepsin and acid secretion.")
6
Role of HP 90% of duodenal ulcer and 70% of gastric ulcer are associated with H.Pylori infection H.Pylori is a gram-negative rod with 6 flagella.

7
HP HP is a chronic infection that found worldwide
Person is infected, usually in childhood. Developing countries have a higher rate of HP infection.

8
HP infection varies with racial and ethnic group- in USA white tend to have lowest rates of infection, African American rates of infection at each age is doubled those of white. This difference in prevalence is related to lower socioeconomic status during childhood.

9
Rout of transmission HP infection in one household member is associated with greater chance of infection in other members. This mean that infection is transmitted person- to- person route and acquired early in life

10
HP HP resides in gastric type epithelium within or beneath the mucus layer which is protect it from acid and antibiotic. It shape and flagella aid it movement within through the mucus layer HP produce variety of enzymes that help it adapt to hostile environment

11
HP HP most potent producer of urease
Urease an enzyme that split urea into ammonia and bicarbonate creating an alkaline microenvironment in the sitting of acidic gastric milieu This facilitate DS in laboratory test

12
Mechanism of gastric injury by HP
1. production of toxic product to case local tissue injury 2. induction of local mucosal immune response 3. increased gastrin levels with a resultant increase in acid secretion.

13
1.Toxic product -local injury
HP locally produce toxic product include: * breakdown product from urease activity (ammonia). * cytotoxins : - a mucinase that degrades mucus and glycoprotein's , phospholipases that damage epithelial and mucus cells * platelet-activating factor-known to cause mucusal injury and thrombosis in microcalcification
. * cytotoxins : - a mucinase that degrades mucus and glycoprotein s , phospholipases that damage epithelial and mucus cells. * platelet-activating factor-known to cause mucusal injury and thrombosis in microcalcification.")
14
2. Local Immune Injury d/t HP
HP known to case local inflammatory reaction in gastric mucusa and to produce chemotactic factors that attract neutrophils and monocytes Activated monocytes and neutrophils in turn produce a number of proinflamatory cytokines and reactive oxygen metabolites

15
3.Gastrine and HP In patient with HP infection basal and stimulated gastrine level are increased secondry to reduction in antral D cells caused by infection with HP. HP-infected patient with duodenal ulcer did have a marked increase in acid secretion

16
HP and other GI disorder
HP is present in most case of chronic gastritis HP most gastric cancer patient show evidence of past HP infection. There is strong association between mucosa-associated lymphoid tissue( MALT) lymphoma and HP infection Eradication of HP infection cause regression of these MALT lymphoma
 lymphoma and HP infection. Eradication of HP infection cause regression of these MALT lymphoma.")
17
Gastritis and PUD PUD strongly associated with antral gastritis.
All patient with PUD have histologic evidence of antral gastritis (95%) The only patient with gastric ulcer and no gastritis those ingesting aspirin or NSAID 25% of patient with NSAID- associated ulcer have evidence of antral gastritis.
 The only patient with gastric ulcer and no gastritis those ingesting aspirin or NSAID. 25% of patient with NSAID- associated ulcer have evidence of antral gastritis.")
18
PUD and NSAID

19
after HP infection NSAID is the most common cause of PUD.
Risk of complication and bleeding in patient taking NSAID is increased with age >60 , patient having prior GI event or use of steroid and anticoagulant

20
Epidemiology of PUD and NSAID
3 million people in USA take daily NSAID 1 in 10patient taking NSAID have an acute ulcer 2%-4% of NSAID user have GI complication each year More than 3000 death and hospitalization per year are attributed to NSAID induced GI complication

21
NSAID injury NSAID can cause acute gastroduodenal injury or chronic.
Acute injury occur within 2 week of use and range from hyperemia to erosion Chronic injury occur after month of use and range from erosion to ulceration

22
Characteristic of NSAID ulcer
NSAID ulcer more frequently found in stomach whereas HP- ulcer found in duodenum Chronic active gastritis always associated with HP and not found in NSAID associated ulcer When NSAID is stopped the ulcer not recur but HP – associated ulcer recurrence is 50%-80% in 1 year unless the organism is eradicated

23
DU pathophisiology Is a disease of multiple ethiology
Absolute requirement: acid and pepsin secretion in combination of H.Pylori infection or NSAIDs ingestion Secretor abnormalities such as : bicarbonate secretion, nocturnal acid secretion, daytime acid secretion DU associated with parietal cell number

24
Pathophysiology of gastric ulcer
GU may occur anywhere in stomach GU rarely develop before age of 40, peak incidence years Predispose condition: age>40, sex f:m 2:1, ingestion of barrier breaking drug (aspirin), abnormalities in acid and pepsin secretion, gastric stasis, delayed gastric emptying, coexisting DU, duodenal gastric reflux of bile, infection with HP, smoking, alcohol intake
, abnormalities in acid and pepsin secretion, gastric stasis, delayed gastric emptying, coexisting DU, duodenal gastric reflux of bile, infection with HP, smoking, alcohol intake.")
25
TYPE I of GU Account for 60% of GU
Occur within 1.5cm of the histologic transition zone between the fundic and and antral mucosa (in the lesser curvature near the incisura) Are not associated with excessive acid secretion Not associated with DU or prepyloric ,pyloric mucosal abnormalities Malignancy are major concern
 Are not associated with excessive acid secretion. Not associated with DU or prepyloric ,pyloric mucosal abnormalities. Malignancy are major concern.")
26
TYPE II of GU About 15% Are located in the body of stomach in combination with a duodenal ulcer Associated with excess acid secretion

27
TYPE III of GU About 20% Located in the preylorus
Are associated with excess of acid secretion

28
TYPE IV of GU ABOUT 10% Occur hiegh in the lesser curvature near the gasroesophageal junction Are not associated with excessive acid secretion

29
clinical feature Abdominal midepigastric pain. Pain is well localized
Tolerable and relieve by food in DU and exagerated by food in GU Pain irradiation to back suggest pentration to pancreas Other magnifestation: perforation, bleeding, obstruction

30
Perforation About 5% of the time ulcer perforated into free peritoneal cavity and elicit chemical peritonitis. The patient recall the exact time of onset of pain. Pain accompanied by fever, tachycardia, dehydration and ileus.

31
Perforation Examination reveal: tenderness, rigidity and rebound
Diagnosis is established by free air in upright chest X-Ray underneath the diaphragm. Treatment is operative after fluid resuscitation

32
Bleeding The most common cause of death with PUD is bleeding in those who have medical problems or are older than 60 years In DU bleeding usually from GDA Most case of massive GI bleeding are DU following penetration of ulcer in GDA Bleeding can manifests as melena or bloody vomiting

33
Obstruction Active inflamation of duodenum can cause mechanical obstruction and functional gastric outlet obstruction Delayed gastric emptying lead to nausea and vomiting Can lead to hypochloremic hypokalemic metabolic alkalosis secondry to loss of gastric juice and H+, CL-, K

34
Zollinger –Ellison Syndrome
ZES clinical triade: 1 .Gastric acid hyper secretion 2. Severe PUD 3. Non-b islet cell tumors ZES are known to produce gastrin and called gastrinomas

35
ZES ZES usually localized to the head of pancreas, duodenal wall or regional LN. ½ of ZES are multiple 2/3 of ZES are malignant ¼ of ZES are associated with MEN1

36
ZES Clinically- abdominal pain and PUD in 80% of case.
½ of patient have diarrhea secondary to increase gastric acid secretion (Gastrin stimulation secretion of acid) Weight loss and steatorrhea occur secondary to decreased duodenal and jeujenal PH and inactivation of lipase Esophagitis is common
 Weight loss and steatorrhea occur secondary to decreased duodenal and jeujenal PH and inactivation of lipase. Esophagitis is common.")
37
When consider ZES In a ptient with recurrent or intractable PUD despite eradication of H.Pylori. In patient with multiple or atypically located ulcer. PUD associated with significant diarrhea PUD associated with symptom of MEN1: hyperparthyroidism Patient with other pancreatic endocrine tumors Large gastric rugae in endoscopy

38
How to diagnose ZES Elevated serum gastrin > 200 pg/ml, value >1000 is diagnostic Secretin test: give secretine 2u/kg and measure serum gastrin before and after gastrin administration evrey 5 minute for 30 minute: an increase of serum gastrin of greater than 200pg/ml above basal level is specific for gastrinoma.

39
Diagnosis of PUD

40
History and physical examination.
Laboratory to R/O other condition: CBC, Liver chimistry, cre, elecgtrolytes, amylase Serum Gastrin in refractory ulcer Chest- X-ray- to rule out perforation Endoscopy or contrast radiography H.pylori testing

41
H.Pylori testing Serology- HP ilicites a local as a systemic immunoglonulin G mediated immune response that can measured by ELISA Serology is test of choice when endoscopy is not indicated Sensitivity 90% Limitation: the test remain high for year or more thus cannot used to assess eradication

42
Urease breath test Carbon- labeled urea breath test
Based in ability of HP to hydrolyze urea to ammonia and bicarbonate Patient ingest 14C or 13C Isotope after carbone ingestion urea metabolized to ammonia and bicarbonate if HP present

43
Urease breath test The bicarbonate is excreted in the breath as labeled carbon dioxide Negative result occur if the test done early after treatment , , 4 weak. Is the method of choice to documment erradication, Test not expensive

44
Rapid urease assay The urease catalize urea to ammonia and bicarbonate creating an alkaline environment This environment can measured by PH indicator Endoscopy is performed and gastric mucosal biopsied to perform the test Sensitivity 90%, specificity 98%.

45
Diagnosis of HP by histology
Endoscopy performed and biopsy obtained Diagnosis is by visualization of HP by hematoxyline and eosin stain Sensitivity is 90%, specificity is 99% HP can cultured – diagnosis required 3-5 days and expensive, sensitivity 80%, specificity is 99%

46
Upper GI radiography The barium is demonstrated within the ulcer crater which is round or oval and may or may not surrounded by edema With single contrast 50% of ulcer may be missed With double contrast 80-90% of ulcer carter can be detected Can asses the depth and penetration Limitation- cannot r/o malignancy

48
Endoscopy The most reliable method of diagnosis
Ability to diagnose malignancy Benign ulcer have smooth ulcer base Malignant ulcer associated with mass and protrude into the lumen or have fold surrounding the ulcer carter Biopsy can performed with endoscopy .

49
Treatment Medical management

50
The goals of treatment 1.symptom need to be relieved
2.The ulcer need to be healed 3. Recurrence must be prevented The antisecretory agent achieve the first 2 goals With NSAIDs related ulcer discontinuation of NSAIDs achieve the 3 goal Eradication of HP achieve the 3 goal

51
Antacids Antacids reduce the gastric acidity by reacting with HCL forming a salt and water If taking on an empty stomach the antacids are emptied rapidly and have only transient effect ( for this take just after meal) Can result in 80% healing at 1 month Magnesium antacids – the best buffers but can cause significant diarrhea Aluminum antacis can bind phosporus and result in hypophospatemia and constipation
 Can result in 80% healing at 1 month. Magnesium antacids – the best buffers but can cause significant diarrhea. Aluminum antacis can bind phosporus and result in hypophospatemia and constipation.")
52
H2-receptor antagonist
Structurally similar to histamine Undergo hepatic metabolism and excreted by kidney Half-life hours The most potent is famotidine Less potent is cimetidine. Result in DU healing 70-80% after 4 weak and 80-90% after 8 weak Continuous IV infusion can produce more effect than intermittent administration

53
Proton Pump Inhibitor Are the most potent antisecretory agent
Bond to the catalytic alfa subunit of the proton pump and negate all types of acid secretion Inhibition is more potent than H2 antagonist and more prolonged and irreversible Produce more rapid healing of ulcer, healing rate 85% at 4 weeks , and 95% at 8 weeks PPI require an acidic environment within gastric lumen to become activated

54
Sucralafate Structurally related to heparin but not have anticoagulant effect Aluminum salt of sulfated sucrose disassociates under acidic condition to sucrose polymerizes and bind protein in ulcer crater to produce a kind of protective coating that can last for 6 hours DU healing after 4-6 weeks of treatment : 1g *4/day Effect is compared to cimetidine

55
Treatment of HP Very important, recurrence without eradication is 72%, after eradication is 2%. Use antibiotic: Moxypen 1gr*2 + clarythromycin 0.5 gr*2 for 14 days Or Moxypen 1gr*2 for 10 days followed by clarythromycin 0.5*2 or metronidasole 0.5*3 for 5 days

56
Surgical Procedure for PUD

57
Indication for operation
1.intractability (failure of ulcer healing after 8-12 weeks of therapy) 2.hemorrhage 3.perforation 4.obstruction
 2.hemorrhage. 3.perforation. 4.obstruction.")
58
The goals of operation Prevent of gastric acid secretion Achieved by:
1.anterctomy- removal of the gastrin-secretion portion of stomach 2.vagotomy alone decrease the acid secretion by 50% 3.Combination of vagotomy and anterectomy decrease acid secretion by 85%

59
Truncal vagotomy Division of RT and LT vagus nervus above the hepatic and celiac branches just above the GEJ Most commonly used for DU . Performe drainage procedure mandatory drainage operation: heineke-mikulicz, Finney, jaboulay pyloroplasty Side effects- bile reflux after gastroduodenostomy, diarrhea after pyloroplasty

61
heineke-mikulicz

62
Finney, jaboulay pyloroplasty

63
Highly Selective Vagotomy (Parietal Cell Vagotyomy)
Divide only the vagus nerve supplying the acid-producing portion of stomach within the corpus and fundus Preserve the vagal innervation of antrum , thus no need for drainage procedure The nerve of latarjet devided and crows feet innervation of fundus and body devided until point 7 cm proximal to pylorus and to point 5 cm proximal to GEJ. Tow or three branchs to antrum and pylorus preserved

64
The criminal nerve of Grassi represent a very proximal branch of the posterior trunk of vagus and great attention is take to avoid missing of them, because is cited predisposition for ulcer recurrence Recurrence rate 10-15% and usually patient responsive to medical therapy This not procedure of choice for pylorus ulcer but for duodenal ulcer Postvagotomy syndrome is rare

66
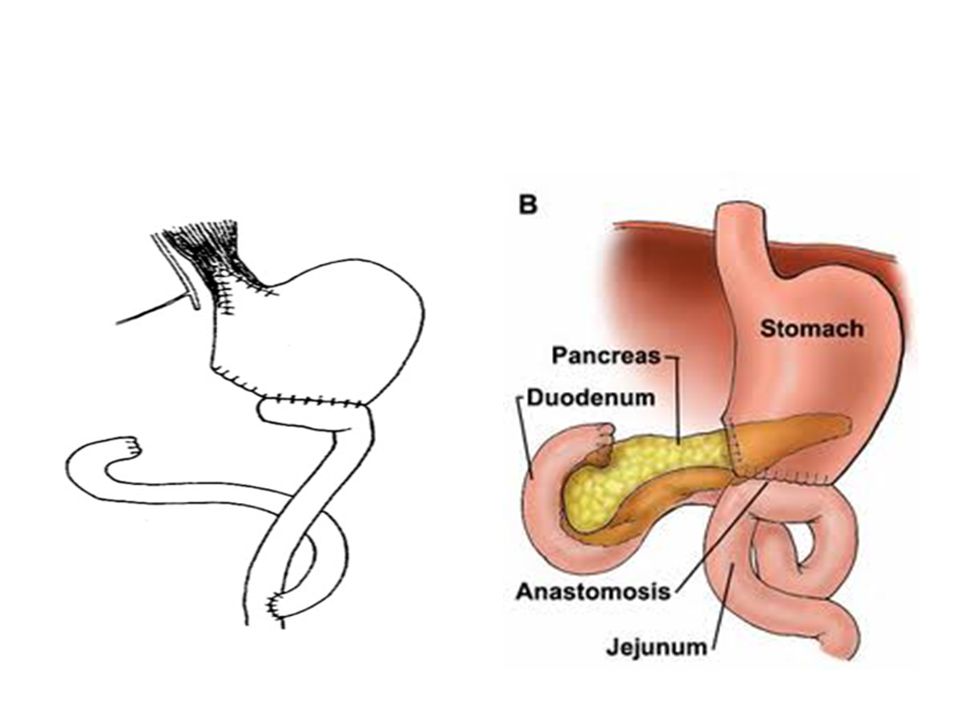
Truncal Vagotomy and Antrectomy
Indication- gastric ulcer and benign gastric tumours Contraindication- cirrhosis, previous operation on duodenum Recurrence rate 0-2% Postagstrectomy and postvagotomy syndrome occur in 20% . Reconstruction of GI tract done by biloroth 1 or 2 or Roux-En-Y

69
Subtotal Gastrectomy Rarely used today for treatment of PUD
Are preserved for malignancy

70
Laparoscopy All previous procedure can performed laparoscopicaly
Also omentopexy for perforation can performed laparoscopicaly. Taylor procedure- parietal cell vagotomy+posterior truncal vagotomy+seromyotomy

71
Surgical Treatment Recommendations for Complications Related to Peptic Ulcer Disease

72
Duodenal Ulcer Intractable: parietal cell vagotomy
Bleeding: truncal vagotomy with pyloroplasty and oversewing of bleeding vessel Perforation: patch closure with treatment of H. pylori with or without parietal cell vagotomy Obstruction: rule out malignancy and parietal cell vagotomy with gastrojejunostomy

73
Gastric Ulcer Intractable Type I: distal gastrectomy with Billroth I
Type II or III: distal gastrectomy with truncal vagotomy Bleeding Type II or III: distal gastrectomy with truncal vagotomy Perforated Type I, stable: distal gastrectomy with Billroth I Type I, unstable: biopsy, patch, and treatment for H. pylori Type II or III: patch closure with treatment of H. pylori Obstruction: rule out malignancy and antrectomy with vagotomy Type IV: depends on ulcer size, distance from the gastroesophageal junction, and degree of surrounding inflammation. Giant gastric ulcers: distal gastrectomy, with vagotomy reserved for type II and III gastric ulcers

74
Thank you

Similar presentations








>")
![Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.](/13/3809458/big_thumb.jpg "Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.>")


, FRCS (Ireland), FRCS(Edinburgh), FRCS(Glasgow), MS, DNB, FAMS, FACS, FICS, Professor of Surgery.>")

>")
 Dr. Gehan Mohamed Dr. Abdelaty Shawky.>")







