Download presentation
Presentation is loading. Please wait.

1
Utilization of Plasma and Plasma derivatives in the perioperative period. Irene Sadek Medical Director Blood Transfusion Services Capital Health

2
Utilization of Plasma and Plasma derivatives in the perioperative period. Plasma products Plasma dosage and volume National and local utilization of plasma Effect on coagulation tests Inappropriate plasma transfusions Use of Octaplex

3
Plasma transfusion Although plasma transfusion guideline exists, there is little evidence to guide the current use of Frozen Plasma. Over 200,000 units of frozen plasma are transfused in Canada annually. A large number of Frozen Plasma transfusions is considered inappropriate The pattern of practice for Frozen Plasma transfusions is highly variable.

4
Plasma transfusion These unnecessary transfusions have important effects on patients and the health care system. Patients experience adverse transfusion reactions Frozen Plasma, a valuable and scarce resource is used up. Not enough Canadian plasma to manufacture plasma derivatives products, e.g IVIg.

5
Plasma products Apheresis plasma 500 ml Aphresis plasma 250 ml Fresh frozen plasma Frozen plasma BC frozen plasma

6
FFP vs BC FP Protein Function (ABO matched, n=20) 0.50 - 1.50 U 0.1880.87 0.142 1.03 Factor IX 0.50 - 1.50 U 0.2500.91 0.315 1.26 Factor VIII 0.50 - 1.50 U 0.2070.90 0.230 1.09 Factor VII 0.50 - 1.50 U 0.1921.06 0.189 1.15 Factor V 0.50 - 1.50 U 0.1230.95 0.137 1.12 Factor II 0.50 - 1.50 U 0.1510.94 0.161 1.11 Factor XI 0.50 - 1.50 U 0.1641.07 0.164 1.24 Factor X NL RangeStd DevMeanStd DevMean FP produced from BC 20-24 hrs after collection FFP produced within 8 hours of collection 6 Note: small data sample size may not be reflective of current performance.
 U Factor IX U Factor VIII U Factor VII U Factor V U Factor II U Factor XI U Factor X NL RangeStd DevMeanStd DevMean FP produced from BC hrs after collection FFP produced within 8 hours of collection 6 Note: small data sample size may not be reflective of current performance.")
7
FFP vs BC FP Protein Function (ABO matched, n=20) ---------0.0840.960.0841.01 Alpha 2 Antiplasmin >0.50 U 0.3771.130.4051.24 Von Willebrand >0.65 U 0.1801.030.4721.15 Protein S 2.00 - 5.00 g/L 1.9453.920.4813.01 Fibrinogen >0.70 U0.1221.050.2231.19 Protein C >0.75 U 0.0531.010.0780.97 Antithrombin NL Range Std DevMeanStd DevMean Produced from BC 20- 24 hrs after collection FFP Produced within 8 hours of collection 7 Note: small data sample size may not be reflective of current performance.
 Alpha 2 Antiplasmin >0.50 U Von Willebrand >0.65 U Protein S g/L Fibrinogen >0.70 U Protein C >0.75 U Antithrombin NL Range Std DevMeanStd DevMean Produced from BC hrs after collection FFP Produced within 8 hours of collection 7 Note: small data sample size may not be reflective of current performance.")
8
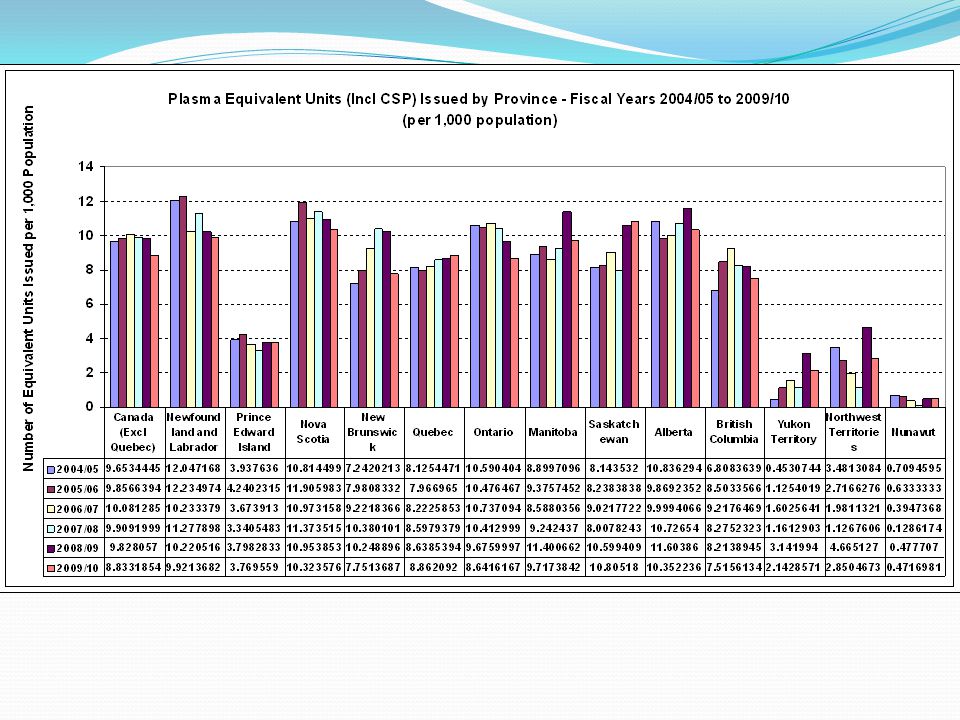
National Plasma utilization

10
Guideline for plasma transfusion Many guidelines published by national organizations or professional organizations over the past 20 years. The guidelines are uniformly, non-evidence-based, or lack sufficient detail to be useful to guide practice in many clinical situations. Typical recommendations such as those put forth by a Canadian Expert Working Group in 1997 include only very general recommendations. British Committee for Standards in Haematology, Blood Transfusion Task Force The British Society for Haematology, 126, 11–28, 2004

11
Canadian Recommendations regarding plasma transfusion CMAJ 1997 Underlying condition Clinical settingCoagulation parameter Level of Evidence Vit K deficiency or warfarin therapy Active bleeding Before emergency surgical or invasive procedure Significantly increased PT, INR, or PTT III Liver diseaseActive bleeding Before emergency surgical or invasive procedure (except percutaneous liver biopsy, paracenthesis and thoracocentesis) Significantly increased PT, INR, or PTT II Massive transfusionMicro vascular bleedingSignificantly increased or unknown PT, INR, or PTT II Acute DIC with treatable triggering condition Active bleedingSignificantly increased PT, INR, or PTT II TTP and HUSplasmapheresisI Acquired deficiencies of a single coagulation factor DDAVP or appropriate factor concentrate, unavailable or inneffective. Serious bleeding Before emergency surgical or invasive procedure III

12
Canadian Recommendations regarding plasma transfusion CMAJ 1997 Underlying condition Clinical settingCoagulation parameter Level of Evidence Vit K deficiency or warfarin therapy Active bleeding Before emergency surgical or invasive procedure Significantly increased PT, INR, or PTT III Liver diseaseActive bleeding Before emergency surgical or invasive procedure (except percutaneous liver biopsy, paracenthesis and thoracocentesis) Significantly increased PT, INR, or PTT II Massive transfusionMicro vascular bleedingSignificantly increased or unknown PT, INR, or PTT II Acute DIC with treatable triggering condition Active bleedingSignificantly increased PT, INR, or PTT II TTP and HUSplasmapheresisI Acquired deficiencies of a single coagulation factor DDAVP or appropriate factor concentrate, unavailable or inneffective. Serious bleeding Before emergency surgical or invasive procedure III

13
British Committee for Standards in Haematology, Blood Transfusion Task Force The British Society for Haematology, 126, 11–28, 2004 Microvascular bleeding with prolonged PT or aPTT. Continued bleeding and lab evidence of coagulopathy during massive transfusion. Urgent reversal of warfarin to stop bleeding or prior to surgery. Acquired or congenital factor deficiencies of V or XI in bleeding patients or prior to surgery or an invasive procedure. Deficiency of antithrombin III, heparin cofactor II, protein C, or protein S when specific factor concentrate is not available. Plasma exchange for TTP or HUS.

14
What is a prolonged PT and PTT The PT and aPTT begin to prolong out of the normal range when coagulation factor levels fall below about 30-50% of normal. Prolongation of the PT or aPTT up to about 1.5 times the midpoint of the normal range, which corresponds to coagulation factor levels of 20-30%, is not usually associated with spontaneous hemorrhage and does not increase the risk of bleeding during routine invasive procedures. However, the risk of bleeding is greater if the platelet count is decreased, platelet function is abnormal, the patient has massive trauma or is undergoing extensive surgery.

15
Indication for plasma transfusion FFP should be used to correct multiple coagulation factor deficiencies in bleeding patients or patients at risk of bleeding requiring an invasive procedure. Coagulation parameters: INR >1.5 and/or PTT > 1.5 times the midpoint or of the normal range. Specific coagulation factor assay with < 30% activity.

16
What do INR and PTT results mean in relation to factor levels

17
Effect of coagulation factor percentage on PT/INR Paradoxic effect of multiple mild coagulation factor deficiencies on the prothrombin time and activated partial thromboplastin time. Burns et al. Am J Clin Pathol. 1993 Aug;100(2):94-8 – The PT begins to lengthen when individual factor levels fall below 25%. – The APTT becomes prolonged when the levels of Factor V fall below 45%; the levels of Factors II and XI fall below 40%; and the levels of Factors I, V, VII, VIII, IX, and XII fall below 25% of normal. Coagulation assays have variable sensitivity to different factors.
:94-8 – The PT begins to lengthen when individual factor levels fall below 25%. – The APTT becomes prolonged when the levels of Factor V fall below 45%; the levels of Factors II and XI fall below 40%; and the levels of Factors I, V, VII, VIII, IX, and XII fall below 25% of normal. Coagulation assays have variable sensitivity to different factors..")
18
More than one factor deficiency Burns et al. Am J Clin Pathol. 1993 Aug;100(2):94-8 When plasma samples containing 50% activity of a single factor and 100% of all other factors were prepared by mixing the congenitally deficient plasma samples with the normal pool, the resulting mixtures had normal PT and APTT values. However, when two of these 50% factor-deficient plasmas were combined so that the mixture contained 75% activity of two coagulation factors and 100% of all other factors, the resulting PT and APTT were prolonged over the clotting times of either 50% factor-deficient plasma.
:94-8 When plasma samples containing 50% activity of a single factor and 100% of all other factors were prepared by mixing the congenitally deficient plasma samples with the normal pool, the resulting mixtures had normal PT and APTT values. However, when two of these 50% factor-deficient plasmas were combined so that the mixture contained 75% activity of two coagulation factors and 100% of all other factors, the resulting PT and APTT were prolonged over the clotting times of either 50% factor-deficient plasma..")
19
More than one factor deficiency Similar findings were obtained in patients with mild factor reductions caused by warfarin treatment. These data indicate that prolongations of the PT and APTT in disorders of coagulation affecting multiple factors represent less of a reduction in factor levels than is generally appreciated. This may explain the poor clinical correlation between abnormalities in these test results and clinical bleeding in acquired disorders of hemostasis.

20
200 consecutive liver transplants Two groups: Low INR <1.5 High INR >1.5 Coagulation parameters were not corrected in the absence of uncontrollable bleeding.

23
Plasma dosage The goal of FFP transfusion is to increase the plasma level of each coagulation factor above 30%. Usually, 10 to 15 mL of FFP per kg body weight is required to treat bleeding due to multiple factor deficiencies. This dose corresponds to 750-1200 ml in an adult. The PT and PTT should be rechecked before subsequent units are transfused. If the PT and PTT remain prolonged, more FFP is indicated.

24
Effect of plasma transfusions on factor levels. Plasma – Dosage – Volume of 1 Unit Plasma: 200-250 mL – 1 mL plasma contains 1 u coagulation factors – 1 Unit contains 220 u coagulation factors – Factor recovery with transfusion = 40% – 1 Unit provides ~80 u coagulation factors – 70 kg X.05 = plasma volume of 35 dL (3.5 L) 80 u = 2.3 u/dL = 2.3% (of normal 100 u/dL) 35 dL In a 70 kg Patient: 1 Unit Plasma increases most factors ~2.5% 4 Units Plasma increase most factors ~10%
 80 u = 2.3 u/dL = 2.3% (of normal 100 u/dL) 35 dL In a 70 kg Patient: 1 Unit Plasma increases most factors ~2.5% 4 Units Plasma increase most factors ~10%.")
25
Appropriate utilization Requests for FFP are the most frequent inappropriate orders received by the blood bank. Reported percentages of inappropriate FFP orders vary from institution to institution and range from 10% to 83%. The most frequent reason for these inappropriate order accounting for at least a third of them, is for correction of a prolonged INR in the absence of bleeding. This prophylactic correction of minor laboratory coagulation abnormalities continues in the absence of evidence of its benefit.

26
Inappropriate use of plasma Crit Care Med. 2007 Jul;35(7):1655-9. Fresh frozen plasma transfusion in critically ill patients. Lauzier F et al 73 (32.4%) were consistent with guidelines, 45 (20.0%) were inconsistent but appropriate, 107 (47.6%) were inappropriate
 were consistent with guidelines, 45 (20.0%) were inconsistent but appropriate, 107 (47.6%) were inappropriate.")
27
Inappropriate use of plasma Crit Care Med. 2007 Jul;35(7):1655-9. Fresh frozen plasma transfusion in critically ill patients. Lauzier F et al 73 (32.4%) were consistent with guidelines, 45 (20.0%) were inconsistent but appropriate, 107 (47.6%) were inappropriate
 were consistent with guidelines, 45 (20.0%) were inconsistent but appropriate, 107 (47.6%) were inappropriate.")
28
Inappropriate use of plasma Crit Care Med. 2007 Jul;35(7):1655-9. Fresh frozen plasma transfusion in critically ill patients. Lauzier F et al 73 (32.4%) were consistent with guidelines, 45 (20.0%) were inconsistent but appropriate, 107 (47.6%) were inappropriate
 were consistent with guidelines, 45 (20.0%) were inconsistent but appropriate, 107 (47.6%) were inappropriate.")
29
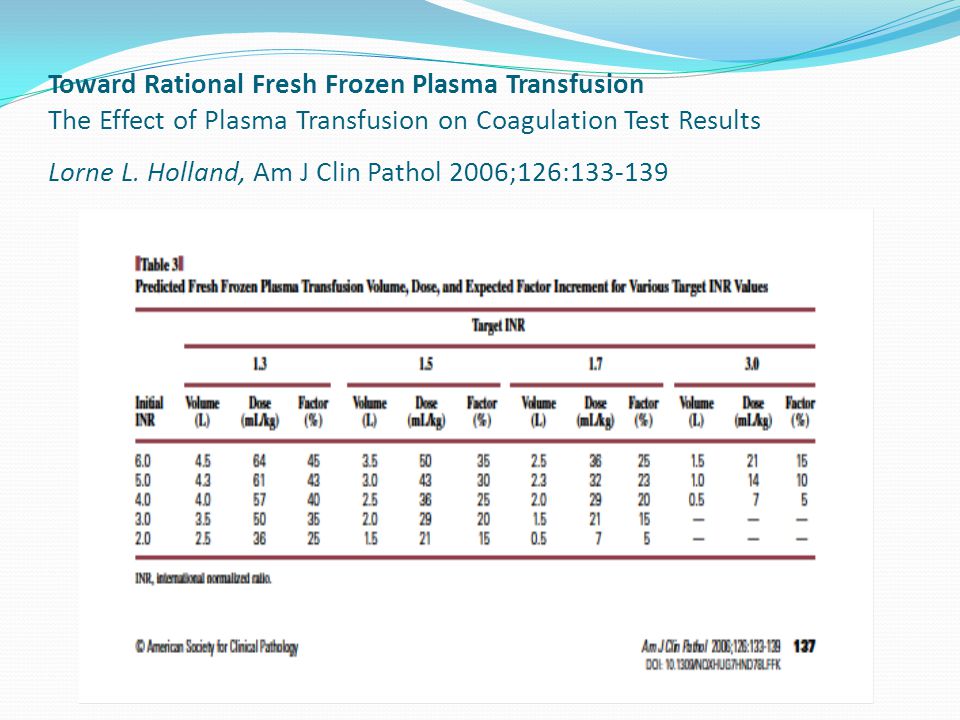
Toward Rational Fresh Frozen Plasma Transfusion The Effect of Plasma Transfusion on Coagulation Test Results Lorne L. Holland, Am J Clin Pathol 2006;126:133-139

32
Effect of fresh-frozen plasma transfusion on prothrombin time and bleeding in patients with mild coagulation abnormalities. Dzik et al Transfusion. 46(8):1279-1285, August 2006 All patients transfused with FFP for – a pretransfusion prothrombin time (PT) between 13.1 and 17 seconds (international normalized ratio [INR], 1.1-1.85) – and with a follow-up PT-INR within 8 hours of transfusion were included. – Of 1091 units of FFP transfused, follow-up coagulation values within 8 hours were available for 121 patients (324 units).
: , August 2006 All patients transfused with FFP for – a pretransfusion prothrombin time (PT) between 13.1 and 17 seconds (international normalized ratio [INR], ) – and with a follow-up PT-INR within 8 hours of transfusion were included. – Of 1091 units of FFP transfused, follow-up coagulation values within 8 hours were available for 121 patients (324 units)..")
33
Effect of fresh-frozen plasma transfusion on prothrombin time and bleeding in patients with mild coagulation abnormalities. Dzik et al RESULTS: – Transfusion of FFP resulted in normalization of PT-INR values in 0.8 percent of patients decreased the PT-INR value halfway to normalization in 15.0 percent of patients Median decrease in PT was 0.20 seconds (median decrease in INR, 0.07). Pretransfusion PT-INR, partial thromboplastin time, platelet count, and creatinine values had no correlation with red blood cell loss. CONCLUSION: – It is concluded that transfusion of FFP for mild abnormalities of coagulation values results in partial normalization of PT in a minority of patients and fails to correct the PT in 99 percent of patients.
. Pretransfusion PT-INR, partial thromboplastin time, platelet count, and creatinine values had no correlation with red blood cell loss. CONCLUSION: – It is concluded that transfusion of FFP for mild abnormalities of coagulation values results in partial normalization of PT in a minority of patients and fails to correct the PT in 99 percent of patients..")
34
Fresh-frozen plasma transfusion in patients with mild coagulation abnormalities at a large Canadian transfusion center. Cheng et al Transfusion vol 47, 2006 722 plasma transfusion episodes mean number of units transfused per episode was 1.07(range, 1-6). The mean pretransfusion international normalized ratio (INR) was 2.04, A significant number (452/722 [62.6%]) were being transfused for an INR between 0.9 and 1.8 (Fig. 1).
. The mean pretransfusion international normalized ratio (INR) was 2.04, A significant number (452/722 [62.6%]) were being transfused for an INR between 0.9 and 1.8 (Fig. 1)..")
35
Fresh-frozen plasma transfusion in patients with mild coagulation abnormalities at a large Canadian transfusion center. Cheng et al

37
CDHA study about plasma transfusions Cheng et al 199 plasma transfusion episodes involving 62 patients, some being transfused on multiple occasions. 16/199(8%) were for plasmapheresis, the majority 183/199(92%) were transfused for other indications. Of these 183 transfusion instances, The average dose of plasma was 567ml, or 1.2 units. Pre-transfusion coagulation studies were ordered 4.6 hours pre- transfusion, with mean INR, PT, and PTT being 2.0, 28 seconds and 40 seconds respectively. Post-transfusion studies were ordered 3.9 hours after transfusion, in 168/183(92%) of cases, with a mean change in INR, PT, and PTT of -0.4, -7.7s, and -3.7s respectively. There was a significant number of plasma transfusions, 91/183(50%) occurring in the population with INR<1.7.
 were for plasmapheresis, the majority 183/199(92%) were transfused for other indications. Of these 183 transfusion instances, The average dose of plasma was 567ml, or 1.2 units. Pre-transfusion coagulation studies were ordered 4.6 hours pre- transfusion, with mean INR, PT, and PTT being 2.0, 28 seconds and 40 seconds respectively. Post-transfusion studies were ordered 3.9 hours after transfusion, in 168/183(92%) of cases, with a mean change in INR, PT, and PTT of -0.4, -7.7s, and -3.7s respectively. There was a significant number of plasma transfusions, 91/183(50%) occurring in the population with INR<1.7..")
38
CDHA study about plasma transfusions Cheng et al Those transfused with 1 unit of plasma (500 ml) experienced a mean change of INR= - 0.44, PT= -8.4 sec, PTT = -4.15sec. Those receiving 2 units had changes of INR =-0.168, PT= -2.96sec, PTT= 0.14sec In the subgroup 91/183(50%) with INR<1.7; their INR = 1.4, PT = 17.3 sec, and PTT 33 sec a mean change of these coagulation values post-transfusion were INR= 0.000, PT= -0.02seconds, and PTT =-3.35sec.
 with INR<1.7; their INR = 1.4, PT = 17.3 sec, and PTT 33 sec a mean change of these coagulation values post-transfusion were INR= 0.000, PT= -0.02seconds, and PTT =-3.35sec..")
39
Appropriateness of Frozen plasma Appropriateness of Frozen Plasma Use in Canada Principal Investigator: Alan T. Tinmouth et al Start Jan 24 Review all transfusions for 2 months.

40
PLASMA DERIVATIVES

41
octaplex ® : A product in good haemostatic balance, i.e. balanced potencies of prothrombin complex factors FII, FVII, FIX and FX – ideal ratio 1:1:1:1 (low target level, but short half-life for FVII) Therapeutic levels of PC, PS (and PZ) (Traces of) ATIII in combination with heparin Low proteolytic activity (e.g. FSAP) and FVIIa Potent product with no thrombogenic tendency
 Therapeutic levels of PC, PS (and PZ) (Traces of) ATIII in combination with heparin Low proteolytic activity (e.g. FSAP) and FVIIa Potent product with no thrombogenic tendency.")
42
octaplex ® : Manufacturing process Cryoprecipitate-poor plasma Heparin and pH adjustment Ion Exchange Chromatography S/D Virus inactivation Ion exchange chromatography Virus removal: Nanofiltration Diafiltration Ultrafiltration Heparin and pH adjustment Sterile filtration, filling Lyophilisation OCTAPLEX

43
octaplex ® use and indication In Canada, octaplex ® is licensed for: Treatment of bleeding and perioperative prophylaxis of bleeding in acquired deficiency of the prothrombin complex coagulation factors (such as deficiency caused by treatment with vitamin K antagonists, or in case of overdose of vitamin K antagonists, when rapid correction of the deficiency is required)
")
44
Dosing recommendations Initial INR2.0 - 2.52.5 - 3.03.0 - 3.5>3.5 Approximate dose* (mL octaplex ® / kg body weight) 0.9 - 1.31.3 - 1.61.6 - 1.9>1.9 The dose will depend on the INR before treatment and the targeted INR. In the following table approximate doses (mL / kg body weight of the reconstituted product) required for normalisation of INR (≤1.2 within 1 hour) at different initial INR levels are given. For example: Recommended dose of octaplex for a 70 kg patient with starting INR of 2.5: 1.3 mL x 70 kg = 91 mL octaplex 91 mL octaplex / 20 mL per vial = 4.55 vials octaplex (2275 IU octaplex) One vial of octaplex is 20 mL and contains 500 IU FIX
 required for normalisation of INR (≤1.2 within 1 hour) at different initial INR levels are given. For example: Recommended dose of octaplex for a 70 kg patient with starting INR of 2.5: 1.3 mL x 70 kg = 91 mL octaplex 91 mL octaplex / 20 mL per vial = 4.55 vials octaplex (2275 IU octaplex) One vial of octaplex is 20 mL and contains 500 IU FIX.")
45
Dosing recommendations Administration: octaplex ® should administered IV. The infusion should start at a speed of 1ml/min, followed by 2-3ml/min, using an aseptic technique. Precaution: pulse should taken before and during injection. If increase occurs, reduce the injection speed or stop administration. For example: Recommended dose of octaplex for a 70 kg patient with starting INR of 2.5: 1.3 mL x 70 kg = 91 mL octaplex 91 mL octaplex / 20 mL per vial = 4.55 vials octaplex (2275 IU octaplex)
.")
46
Dosage: less than the manufacturer’s recommended dose Adult patients: 40 mL octaplex (1000 IU Factor IX activity*) and 10 mg Vitamin K IV *[Others have - Double the dose if INR>3 or weight>90 kg, adopted weight based dosing or adopted weight based/ INR based dosing. Administration:Run over 15 min/1,000 IU

47
Treatment, time and INR

48
Contains a small amount of heparin therefore should not be given to patients with HIT or with known allergies to heparin Should not be given to patients with a hypersensitivity to any ingredient in the product Relative contraindications, due to high risk of thrombotic complications, include acute coronary syndrome, DIC, severe liver disease, and liver transplant octaplex® should not be used in massive transfusion cases. octaplex® should not be used in coagulopathy associated with liver dysfunction. octaplex® should not be used in patients with recent history of thrombosis, myocardial infarction, recent ischemic stroke or Disseminated Intravascular Coagulation (DIC). What are the contraindications?
. What are the contraindications .")
49
Efficacy (n=7) (n=20) octaplex ® : Clinical trials – LEX-202
 (n=20) octaplex ® : Clinical trials – LEX-202")
50
Clinical studies: LEX-202 Lubetsky, A, Thromb Res 2004;113:371-378 n= 20 (10 bleeding, 10 surgery) Median dose: 26,1 IU/kg
 Median dose: 26,1 IU/kg")
51
Efficacy (n=20)(n=4) (n=9) (n=2) octaplex ® : Clinical trials – LEX-202
(n=4) (n=9) (n=2) octaplex ® : Clinical trials – LEX-202")
52
OCTAPLEX, CDHA experience. Al-Mohamadi et al.. Retrospective data on 50 patients received OCTAPLEX between Feb and December 2009. - - 38 met NAC criteria 22 presented with bleeding 16 prophylactic (taken to surgery) - 12 did not meet NAC criteria 8 with bleeding 4 prophylactic (taken to surgery)
 - 12 did not meet NAC criteria 8 with bleeding 4 prophylactic (taken to surgery).")
53
OCTAPLEX, CDHA experience. INR Post- octaplex INR Pre- octaplex Patients N=38 1.63.9Bleeding N=22 1.63.3Pre-op N=16 INR Post-octaplex INR Pre-octaplex Patients N=38 1.63.9Bleeding N=22 1.63.3Pre-op N=16

54
OCTAPLEX, CDHA experience. One dose of 40ml reasonably corrected INR in the vast majority of patients. Moreover, this single dose was enough to stop the bleeding in all patients except one patient who was on non steroidal anti-inflammatory drugs presenting with massive upper GI bleeding.

55
OCTAPLEX, CDHA experience. INR Pre-octaplex INR Post- octaplex <2 N=6 <1.5 2-4 N=21 1.67 4-6 N=7 1.61 >6 N=4 2.2

56
Patients divided by two post-octaplex targets INR of 1.6 and INR of 1.7 INR: 4-6 42% post INR 1.6 or less 85% post INR 1.7 or less INR: 2-4 52% post INR 1.6 or less 68% post INR 1.7 or less INR: 2-4 52% post INR 1.6 or less 68% post INR 1.7 or less INR: 2-4 52% post INR 1.6 or less 68% post INR 1.7 or less INR: 2-4 52% post INR 1.6 or less 68% post INR 1.7 or less INR: 2-4 52% post INR 1.6 or less 68% post INR 1.7 or less

57
Octaplex Octaplex utilization is monitored closely Provincial guidelines are in place Approval process Acceptable use of octaplex at CDHA Dose per capita comparison.

59
Plasma Plasma utilization is high. 50-60 % of plasma transfusions are for INR<1.7. Need for plasma transfusion guidelines??? Physician education?? Approriate utilization Adverse events to plasma transfusion...

60
Questions or advice?

Similar presentations






>")

















