Download presentation
Presentation is loading. Please wait.

1
Shoulder, Elbow, and Wrist
For the Lecture Final Exam

2
The Pectoral Girdle Provides attachment for many muscles that move the upper limb Girdle is very light and upper limbs are mobile Only clavicle articulates with the axial skeleton Socket of the shoulder joint (glenoid cavity) is shallow Good for flexibility, bad for stability
 is shallow. Good for flexibility, bad for stability.")
3
Articulated Pectoral Girdle
Clavicle Acromio- clavicular joint Scapula PLAY Shoulder (a) Articulated pectoral girdle Figure 8.1a
 Articulated pectoral girdle. Figure 8.1a.")
4
Clavicles Extend horizontally across the superior thorax
Sternal end articulates with the manubrium Acromial end articulates with scapula Provide attachment for muscles Hold the scapulae and arms laterally Transmit compression forces from the upper limbs to the axial skeleton SCAPULA Lies on the dorsal surface of the rib cage Located between ribs 2–7 PLAY Shoulder

5
Arm Region of the upper limb between the shoulder and elbow Humerus
The only bone of the arm Longest and strongest bone of the upper limb Articulates with the scapula at the shoulder Articulates with the radius and ulna at the elbow Many structures of the humerus provide sites for muscle attachment Other structures of the humerus provide articulation sites for other bones

6
Forearm Formed from the radius and ulna
Proximal ends articulate with the humerus Distal ends articulate with carpals Radius and ulna articulate with each other At the proximal and distal radioulnar joints The interosseous membrane Interconnects radius and ulna In anatomical position; the radius is lateral and the ulna is medial PLAY Elbow

7
Proximal Part of the Ulna
Olecranon process Radial notch of the ulna Olecranon process Head of radius Head Trochlear notch Neck Neck of radius Radial tuberosity Coronoid process Proximal radioulnar joint Interosseous membrane Interosseous membrane Ulna Ulna Radius Ulnar notch of the radius Ulnar notch of the radius Radius Head of ulna Head of ulna Styloid process of radius Styloid process of ulna Distal radioulnar joint Styloid process of ulna (a) Anterior view (b) Posterior view Styloid process of radius Figure 8.4a, b
 Anterior view. (b) Posterior view. Styloid process of radius. Figure 8.4a, b.")
8
Contributes heavily to the wrist joint
RADIUS Contributes heavily to the wrist joint Distal radius articulates with carpal bones When radius moves, the hand moves with it ULNA Main bone responsible for forming the elbow joint with the humerus Hinge joint allows forearm to bend on arm Distal end is separated from carpals by fibrocartilage Plays little to no role in hand movement

9
Proximal Ends of the Radius and Ulna
Humerus Humerus Coronoid fossa Olecranon fossa Capitulum Medial epicondyle Olecranon process Lateral epicondyle Medial epicondyle Head of radius Trochlea Coronoid process of ulna Head Radial tuberosity Neck Radial notch Radius Ulna Ulna Radius (c) Anterior view at the elbow region (d) Posterior view of extended elbow Figure 8.3c, d
 Anterior view at the elbow region. (d) Posterior view of extended elbow. Figure 8.3c, d.")
10
Location of styloid processes of radius and ulna.
Head of ulna Styloid process of ulna (a) Normal position
 Normal position.")
12
Carpal bones Forms the true wrist—the proximal region of the hand
Gliding movements occur between carpals Are arranged in two irregular rows Proximal row from lateral to medial Scaphoid, lunate, triquetrium, and pisiform Distal row from lateral to medial Trapezium, trapezoid, capitate, and hamate A mnemonic to help remember carpals: Sally left the party to take Carmen home

13
Bones of the Hand Phalanges Distal Middle Proximal Metacarpals Head
Sesamoid bones Shaft Carpals Base 4 3 2 5 1 Hamate Carpals 2 3 4 1 5 Carpals Capitate Trapezium Hamate Pisiform Trapezoid Capitate Triquetrum Scaphoid Triquetrum Lunate Lunate Ulna Radius Ulna (a) Anterior view of right hand (b) Posterior view of right hand Figure 8.6a, b
 Anterior view of right hand. (b) Posterior view of right hand. Figure 8.6a, b.")
14
Metacarpals Metacarpals form the palm
Numbered 1–5, beginning with the pollex (thumb) Phalanges form the digits Named also by whether it is proximal, intermediate (or middle), or distal. The pollex does not have a middle phalanx. The second middle phalanx refers to the second DIGIT.
 Phalanges form the digits. Named also by whether it is proximal, intermediate (or middle), or distal. The pollex does not have a middle phalanx. The second middle phalanx refers to the second DIGIT.")
15
Plane Joints Movement in the transverse or frontal plane only. These are not axial since the movement does not occur around an axis. Examples are the carpal and tarsal bones, between the articular processes of the vertebrae

16
Hinge Joints Uniaxial movement
Movement around an axis in the sagittal plane only (uniaxial). Examples are the elbow, knee, and IPJ = interphalangeal (finger and toe) joints. There are two types of IPJ’s: Distal (DIPJ) and Proximal (PIPJ). Medial/ lateral axis Flexion and extension Uniaxial movement
. Examples are the elbow, knee, and IPJ = interphalangeal (finger and toe) joints. There are two types of IPJ’s: Distal (DIPJ) and Proximal (PIPJ). Medial/ lateral. axis. Flexion and extension. Uniaxial movement.")
17
Pivot Joints Rotation movement around a vertical axis (uniaxial).
Ulna Radius Vertical axis Rotation Rotation movement around a vertical axis (uniaxial). Examples are between the first two vertebrae and proximal radioulnar joint, where the annular ligament on the ulna encircles the head of the radius
. Examples are between the first two vertebrae and proximal radioulnar joint, where the annular ligament on the ulna encircles the head of the radius.")
18
Condyloid Joints Allows for movement in two planes (biaxial) because the bones are shaped like a condyle in a cup. Examples are the Metacarpal-phalangeal joints (MPJ’s). These are called biaxial condyloid joints
. These are called. biaxial condyloid joints.")
19
Saddle Joints Both bones are concave on one side and convex on the other. Allows for movement in two planes (biaxial). Example is at the base of the thumb (between the trapezium and metacarpal I) Saddle joints are biaxial joints; in primate anatomy, allows for the opposable thumb
 Saddle joints are biaxial joints; in primate anatomy, allows for the opposable thumb.")
20
Ball and Socket Joints Allows for movement in three planes (multiaxial). Examples are the shoulder and hip joints.

21
Bursae and Tendon Sheaths
The knee joint has at least 13 bursae Figure 9.4a, b

22
The Shoulder Joint Diarthrotic (freely moveable) ball and socket joint: Humeral head in glenoid cavity
 ball and socket joint: Humeral head in glenoid cavity.")
23
Trapezoid ligament (part of coracoclavicular ligament)
Clavicle Acromioclavicular ligament Conoid ligament (part of coracoclavicular ligament) Acromion Tendon of supraspinatus muscle Superior transverse scapular ligament Coracoacromial ligament Coracoid process Tendon of long head of biceps brachii muscle Articular capsule Tendon of subscapularis muscle Humerus Scapula (in part)
 Acromion. Tendon of supraspinatus muscle. Superior transverse scapular ligament. Coracoacromial ligament. Coracoid process. Tendon of long head of biceps brachii muscle. Articular capsule. Tendon of subscapularis muscle. Humerus. Scapula (in part)")
24
Shoulder Joint (Glenohumeral Joint)
Ligaments: Glenohumeral ligaments : 3 fibrous bands From the anterior glenoid labrum to the anatomical neck of humerus Reinforce the anterior part of the articular capsule (and are inside the capsule, not visible from outside.) Coracohumeral ligament From base of coracoid process to anterior aspect of greater tubercle of humerus Transverse humeral ligament Runs from greater to lesser tubercle of humerus Creates a channel , bridging over the intertubercular groove Site for tendon of long head of biceps brachii Coracoacromial ligament From inferior aspect of acromion to coracoid process Forms a protective “arch” preventing superior displacement of the head Supraspinatus muscle passes under this arch.
 Coracohumeral ligament. From base of coracoid process to anterior aspect of greater tubercle of humerus. Transverse humeral ligament. Runs from greater to lesser tubercle of humerus. Creates a channel , bridging over the intertubercular groove. Site for tendon of long head of biceps brachii. Coracoacromial ligament. From inferior aspect of acromion to coracoid process. Forms a protective arch preventing superior displacement of the head. Supraspinatus muscle passes under this arch.")
25
Shoulder Ligaments

26
Shoulder:Glenohumeral Joint

27
Shoulder Ligaments 10 points on lecture final exam:
Label the following drawing with the names of the ligaments that attach the clavicle to the scapula and to the head of the humerus.

28
10 pt Essay Question: Label this (½ pt each)
")
29
Essay Answer: ½ pt each

30
The sternoclavicular joint.
Anterior sternoclavicular ligament and joint capsule Articular disc Interclavicular ligament Elevation Retraction Posterior rotation Clavicle Protraction Depression Manubrium of sternum Costoclavicular ligament Costal cartilage of 1st rib (a) Sternoclavicular joint, anterior view (b) Sternoclavicular movements
 Sternoclavicular joint, anterior view. (b) Sternoclavicular movements.")
31
Glenoid labrum Synovial cavity of the glenoid cavity containing synovial fluid Hyaline cartilage Fibrous capsule Humerus (b) Cadaver photo corresponding to (a)
 Cadaver photo corresponding to (a)")
32
Elbow joint Articular capsule Synovial membrane Humerus
Synovial cavity Articular cartilage Fat pad Coronoid process Tendon of triceps muscle Tendon of brachialis muscle Ulna Bursa Trochlea Articular cartilage of the trochlear notch (a) Mid-sagittal section through right elbow (lateral view)
 Mid-sagittal section through right elbow (lateral view)")
33
Elbow joint Humerus Anular ligament Radius Lateral epicondyle
Articular capsule Radial collateral ligament Olecranon process Ulna (b) Lateral view of right elbow joint
 Lateral view of right elbow joint.")
34
Elbow joint Humerus Anular ligament Medial epicondyle Radius Ulnar
collateral ligament Articular capsule Coronoid process of ulna Ulna (c) Cadaver photo of medial view of right elbow
 Cadaver photo of medial view of right elbow.")
35
Elbow joint Articular capsule Humerus Anular ligament Coronoid process
Medial epicondyle Ulnar collateral ligament Radius Ulna (d) Medial view of right elbow
 Medial view of right elbow.")
36
Radius Ulna Radiocarpal joint Lunate Triquetrum Scaphoid Pisiform Capitate Hamate Trapezoid Trapezium Thumb (a) Right wrist, anterior (palmar) view
 Right wrist, anterior (palmar) view.")
37
Radiocarpal joint Distal radioulnar joint Articular disc Radial collateral ligament Ulnar collateral ligament Intercarpal joint (b) Wrist joints, coronal section
 Wrist joints, coronal section.")
38
Palmar radiocarpal ligament Radius Ulna Lunate Radial collateral ligament Ulnar collateral ligament Scaphoid Intercarpal ligaments Pisiform Hamate Trapezium Carpo- metacarpal ligaments Capitate (c) Ligaments of the wrist, anterior (palmar) view
 Ligaments of the wrist, anterior (palmar) view.")
39
Rheumatoid arthritis

40
Notice that these are all synovial joints.

41
Extensor pollicis longus
Flexor pollicis brevis Flexor pollicis longus Adductor pollicis Lumbricals Abductor pollicis brevis Flexor digitorum profundus Flexor digitorum superficialis Opponens digiti minimi Abductor digiti minimi Flexor digiti minimi brevis

42
Dorsal interosseus Abductor digiti minimi

43
Brachial Plexus ROOTS TRUNKS DIVISIONS CORDS NERVES

44
Brachial Plexus

45
Brachial Plexus Damage to Brachial Plexus
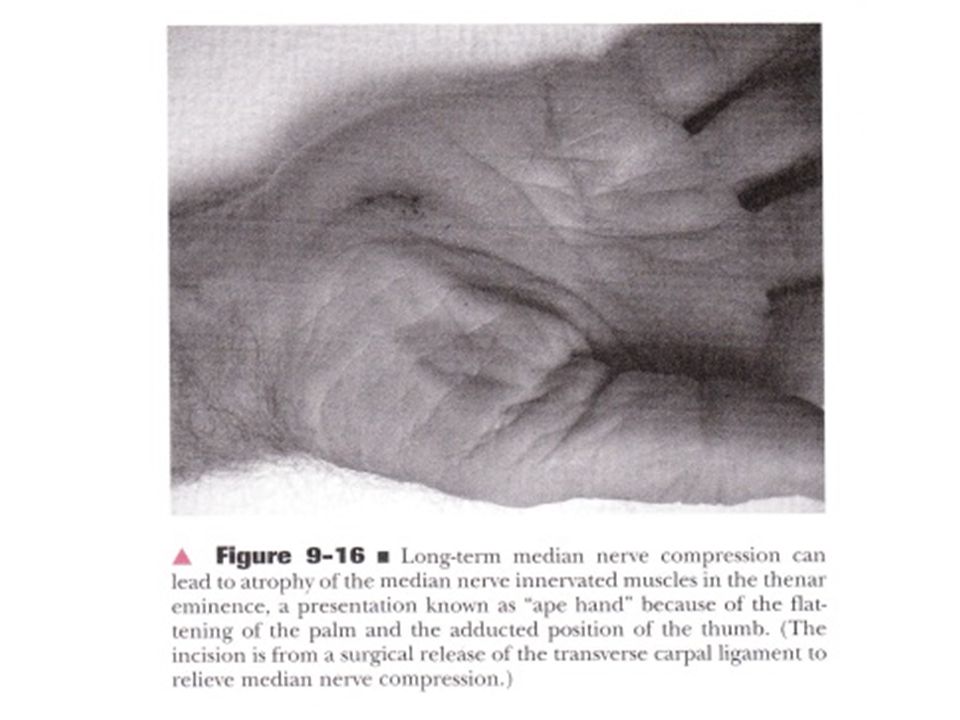
Congenital (brachial plexus damaged during birth) Klumpke’s paralysis Acquired Brachial Plexus injuries Crutch paralysis (total upper extremity paralysis) Claw Hand Carpal Tunnel Syndrome, Ape hand, Hand of benediction Wrist Drop (Waiter’s Hand)
 Klumpke’s paralysis. Acquired Brachial Plexus injuries. Crutch paralysis (total upper extremity paralysis) Claw Hand. Carpal Tunnel Syndrome, Ape hand, Hand of benediction. Wrist Drop (Waiter’s Hand)")
46
Major Nerves of the Upper Extremity
Axillary Musculocutaneus Major Nerves of the Upper Extremity

47
Axillary Nerve Deltoid Teres minor

48
Musculocutaneus Nerve Supplies anterior muscles of the arm
Axillary Musculocutaneus Musculocutaneus Nerve Supplies anterior muscles of the arm

49
Patient trying to make a fist
Median Nerve Supplies no muscles of the arm Supplies anterior forearm (except flexor carpi ulnaris) Damage can cause Carpal Tunnel Syndrome Hand of benediction Ape Hand Patient trying to make a fist
 Damage can cause. Carpal Tunnel Syndrome. Hand of benediction. Ape Hand. Patient trying to make a fist.")
50
Carpel Tunnel Syndrome

51
Carpel Tunnel Syndrome

52
Carpel Tunnel Syndrome
The median nerve travels under the transverse carpal ligament. The nerve is pinched in carpal tunnel syndrome.

53
MEDIAN NERVE This is the nerve that gets cut when people try to slit their wrists. The arteries are so small in the wrist; people rarely die from this type of suicide attempt. However, they live with a lot of tissue damage. They are not able to move the thumb towards the little finger, so it is hard to pick up small objects. This is called “ape hand”.

55
Ulnar Nerve Supplies flexor carpi ulnaris “Funny Bone”
Damage can cause claw hand; cannot adduct or abduct fingers

56
Radial Nerve Supplies muscles on the posterior arm and forearm
Triceps brachii Extensor carpi radialis Extensor digitorum communis Damage can cause wrist drop

57
Carpel Tunnel Syndrome
Ape Hand

58
Brachial plexus Radial nerve Musculocutaneous nerve Median nerve Ulnar nerve Axillary nerve Axillary nerve

59
Median nerve Radial nerve Ulnar nerve

60
Arteries of the Upper Extremity

61
Radial artery Superficial palmar arch Ulnar artery Anterior interosseous artery Brachial artery

62
Arteries of the Upper Extremity
Subclavian (becomes axillary artery in armpit) Axillary (becomes brachial artery in arm) Supplies triceps brachii Brachial (divides into radial and ulnar arteries when it reaches the elbow) Supplies arm muscles except triceps brachii Radial Ulnar
 Axillary (becomes brachial artery in arm) Supplies triceps brachii. Brachial (divides into radial and ulnar arteries when it reaches the elbow) Supplies arm muscles except triceps brachii. Radial. Ulnar.")
63
Cephalic Brachial Axillary Brachial Median cubital Radial Radial Ulnar Ulnar

64
Patient Case Susan reports shoulder pain located at the proximal lateral humerus. The pain is worse when sleeping on the right shoulder, and also when she elevates her arm. This location is consistent with pain originating from the shoulder cuff tendons, the long head of biceps brachii, or subacromial bursa. Her pain may be from the rotator cuff, bursitis, or biceps tendonitis. Pain from laying on the shoulder is consistent with pain originating from the subacromial space. The humerus compresses the bursa there when laying on the affected side.

65
Patient Case When the arm is elevated and especially when carrying a load in that position, the subacromial bursa is compressed. As the supraspinatus muscle contracts in this position, the blood supply to its tendon is impinged. Repeating these motions during the day may cause a supraspinatus tendon tear, since its nutrient vessels are pinched.

66
Supraspinatus The supraspinatus muscle participates in humeral elevation throughout its range of motion, especially the first 5-10 degrees, so it is under tension most of a person’s waking hours and is vulnerable to tensile overload. The trapezius then takes over most of the rest of the range of motion. Supraspinatus is the most vulnerable of the cuff muscles. Rotator cuff tendinitis produces pain between degrees of humeral elevation in relation to the trunk. This range is called the painful arc. Beyond 120 degrees, the tendons have cleared the coracoacromial arch. If the pain occurs beyond 120 degrees, it is more likely to be from degeneration of the acromial-clavicular joint.

67
Rotator Cuff Injury Symptoms
Pain and tenderness in the shoulder, especially when reaching overhead, reaching behind the back, lifting, pulling or sleeping on the affected side. Diagnosis X-rays MRI Ultrasound

68
Causes of Rotator Cuff Injuries
Normal wear and tear. Poor posture. When you slouch your neck and shoulders forward, the space where the rotator cuff muscles reside can become smaller. This can allow a muscle or tendon to become pinched under your shoulder bones (including your collarbone), especially during overhead activities, such as throwing. Falling. Using your arm to break a fall or falling on your arm Lifting or pulling. Lifting an object overhead Likewise, pulling something, such as a high-poundage archery bow, may cause an injury. Repetitive overhead movement. This occurs often in athletes, especially baseball pitchers, swimmers and tennis players. It's also common among people in the building trades, such as painters and carpenters.
, especially during overhead activities, such as throwing. Falling. Using your arm to break a fall or falling on your arm. Lifting or pulling. Lifting an object overhead Likewise, pulling something, such as a high-poundage archery bow, may cause an injury. Repetitive overhead movement. This occurs often in athletes, especially baseball pitchers, swimmers and tennis players. It s also common among people in the building trades, such as painters and carpenters.")
69
Trapezius Serratus anterior and trapezius both abduct the arm. Trapezius can abduct the arm through its full range of motion, although it is weaker without serratus anterior. Overuse and damage to trapezius can result in a shoulder shrug motion when trying to elevate the arm, and fatigue and pain in that muscle. This also might be a cause of Susan’s pain.

70
Upper Trapezius Strain
An upper-trapezius strain can be triggered quite easily by consistently overusing the muscle group, even at a low intensity. Because repetitive motions do not allow the affected tissue to rest between movements, they can cause stress and irritation. The members of today’s work force don’t often get up to sharpen a pencil, fax documents or walk to the post office to deliver a package. The easy and convenient access of working tools promotes inactivity and therefore a rise in repetitive stress injuries associated with desk and computer work. Simple, everyday movements—like habitually holding a telephone between the ear and shoulder—can trigger upper trapezius pain.

71
Upper Trapezius Strain
It is easy to understand how the upper trapezius could be in a state of active insufficiency in certain situations; for example, when the shoulder is elevated and the neck is extended, side-bent and rotated, as when you are cradling a phone between your ear and shoulder. Shrugging the shoulders and overhead movements also fatigue trapezius. Throughout the day, the upper trapezius might be actively insufficient, while, alternatively, the rhomboids might be passively insufficient (when the shoulders are rounded). Developing better posture and moving out of these positions intermittently throughout the workday will place the muscles back at their optimal length.
. Developing better posture and moving out of these positions intermittently throughout the workday will place the muscles back at their optimal length.")
72
Trapezius Exercises at the Office
Sitting with upright posture, perform 15–20 reps an hour of the following upper trapezius exercises. 1. Scapular Pinches. Roll the shoulders back, and pinch the shoulder blades together. 2. Shoulder Shrugs. Raise the shoulders up toward the ears, then lower them back down. 3. Neck Side-Bending. Tilt one ear toward the shoulder, and hold briefly. 4. Neck Rotation. Look over one shoulder, and pause briefly. 5. Neck Stretch. In a standing or seated position, place the right hand on top of the head and let the left arm rest at the side. Gently pull the head toward the right shoulder with the right hand. Rotate the head down and look at the right hip. (The stretch should be felt on the left side of the neck/shoulder area.) Repeat on the opposite side.
 Repeat on the opposite side.")
73
Elbow Pain When the elbow joint capsule is inflamed, the patient holds the elbow flexed at about 80 degrees. That is the position at which the least amount of tension is present in the joint capsule and surrounding structures.

74
Elbow Pain Most elbow pain results from overuse injuries; many sports, hobbies and jobs require repetitive hand, wrist or arm movements. Elbow pain may occasionally be due to arthritis, but in general, your elbow joint is much less prone to wear-and-tear damage than are many other joints.

75
Common Causes of Elbow Pain
Fractures, ligament sprains and muscle and tendon tears Dislocation; usually caused by a fall. Children may dislocate the head of the radius from being pulled by the arm (nursemaid’s elbow). Tennis elbow (lateral epicondylitis) from forceful extension of wrist; wrist extension is painful. Diagnose by resisting extension of third finger, creating pain in lateral epicondyle. Golfer's elbow (medial epicondylitis) from repeatedly flexing wrists or clenching fingers Cubital tunnel syndrome, ulnar nerve on the inside of the elbow is irritated or injured Little league elbow syndrome (pitcher's elbow) — an injury mainly affecting children and rapidly growing adolescents involved in throwing sports such as baseball Olecranon bursitis — inflammation of a small sac of fluid (olecranon bursa) on the tip of your elbow Osteochondritis dissecans - Caused by reduced blood flow to the end of a bone, occurs most often in young men, particularly after an injury to a joint. Radial tunnel syndrome, which occurs when the radial nerve becomes compressed just beyond the elbow (sometimes called resistant tennis elbow) Nursemaid’s Elbow
. Tennis elbow (lateral epicondylitis) from forceful extension of wrist; wrist extension is painful. Diagnose by resisting extension of third finger, creating pain in lateral epicondyle. Golfer s elbow (medial epicondylitis) from repeatedly flexing wrists or clenching fingers. Cubital tunnel syndrome, ulnar nerve on the inside of the elbow is irritated or injured. Little league elbow syndrome (pitcher s elbow) — an injury mainly affecting children and rapidly growing adolescents involved in throwing sports such as baseball. Olecranon bursitis — inflammation of a small sac of fluid (olecranon bursa) on the tip of your elbow. Osteochondritis dissecans - Caused by reduced blood flow to the end of a bone, occurs most often in young men, particularly after an injury to a joint. Radial tunnel syndrome, which occurs when the radial nerve becomes compressed just beyond the elbow (sometimes called resistant tennis elbow) Nursemaid’s Elbow.")
76
Treatment of Elbow and Wrist Pain
Splinting Forearm support bands Taping Ultrasound Manipulation Exercise Oral anti-inflammatory medicines Cortisone injections

77
Extensor Retinaculum

78
Patient Case George has been a computer programmer for 20 years. He has numbness in his right hand on the thumb, index finger, and middle finger. Tapping on the carpal tunnel causes parathesias (tingling) in the median nerve distribution (positive Tinel’s sign). Placing his wrist in sustained flexion for one minute also causes the parathesias (positive Phalen’s test).
 in the median nerve distribution (positive Tinel’s sign). Placing his wrist in sustained flexion for one minute also causes the parathesias (positive Phalen’s test).")
79
Patient Case Treatment began with splinting the wrist in neutral position and patient education for proper ergonomics (use a wrist pad while typing).
.")
80
Anti-Deformity Positioning
After trauma to the hand, a custom-fabricated splint is provided for support and protection during healing. Because the collateral ligaments of the MP joints are slack with extension, immobilization in MP extension would place the collateral ligaments at risk for adaptive shortening, limiting joint flexion, which impairs grasp. A splint should place the MP joints in flexion. The IP joints should be held in extension to reduce the risk of flexion contractures. The thumb should be placed in slight abduction to prevent contracture.

81
Ulnar Nerve Damage: Cubital Tunnel Syndrome
When the medial epicondyle is struck while the elbow is flexed, the ulnar nerve can be damaged. The extensor digitorum muscle alone can extend the IP joints of the two small fingers if full MPJ extension is prevented. The splint is shaped so the flexor digitorum longus can still flex.

82
Wartenberg’s Sign Ulnar nerve damage can cause claw hand because the flexors become weak, giving the extensors a mechanical advantage, pulling the two little fingers into a claw. The little finger may also assume an MPJ abduction position, called Wartenberg’s sign.

83
Trigger Finger Trigger finger is one example of the disability that can be created when repetitive trauma to a flexor tendon results in the formation of nodules on the tendon. Finger flexion may be prevented completely, or the finger may be unable to re-extend.

84
Pistol Grip Tapered shape Cylindrical Grip Lateral prehension Power Grip Precision Handling Spherical Grip Hook Grip

85
Carpal Fractures Upper extremity fractures are among the most common of the extremity injuries with carpal fractures accounting for 18% of hand fractures and 6 percent of all fractures. Of these, fractures to bones of the proximal row are most frequent. Fractures of the pisiform bone occur less often than fractures of the scaphoid, lunate, or triquetrum (triangular). Pisiform fractures account for 1-3% of all carpal bone osseous injuries
. Pisiform fractures account for 1-3% of all carpal bone osseous injuries.")
86
Pisiform Fracture Most commonly the pisiform is injured in a fall on the outstretched hand with the wrist in extension or if the heel of the hand is used like a hammer. When the wrist is in this position, the flexor carpi ulnaris tendon compresses the pisiform to the triquetrum. These mechanisms can create an avulsion fracture of the distal aspect of the pisiform, a linear fracture, or a chondral injury to its dorsal surface. The bone may need to be removed surgically. Being an anchor for several ligamentous attachments, and the origin of the abductor digiti minimi, there is a 50% chance of an associated injury to the distal radius or to another carpal bone when a fracture of the pisiform is identified.

87
Scaphoid Fracture Scaphoid fractures are among the most common injuries. They frequently occur following a fall onto an outstretched hand. X-rays taken soon after the injury may not reveal a fracture, but the clinician should assume one is present until definitive proof otherwise is obtained. Of all carpal fractures, scaphoid fractures are by far the most common, accounting for 10% of all hand fractures and 60-70% of all carpal fractures.

88
Anatomical Snuffbox The anatomical snuffbox is a triangular deepening on the radial, dorsal aspect of the hand—at the level of the carpal bones, specifically, the scaphoid and trapezium bones forming the floor. The name originates from the use of this surface for placing and then sniffing powdered tobacco, or “snuff.”

89
Anatomical Snuffbox The radius and scaphoid articulate deep to the snuffbox to form the basis of the wrist joint. In the event of a fall onto an outstretched hand, this is the area through which the brunt of the force will focus. This results in these two bones being the most often fractured of the wrist. In a case where there is localized tenderness within the snuffbox, the fracture is likely to be of the scaphoid. The scaphoid is a small, oddly shaped bone whose purpose is to facilitate mobility rather than confer stability to the wrist joint. In the event of inordinate application of force over the wrist, this small scaphoid is clearly likely to be the weak link. Interestingly, scaphoid fracture is one of the most frequent causes of medico-legal issues.

90
Anatomical Snuffbox An interesting anatomical anomaly in the vascular supply to the scaphoid is the area to which the blood supply is first delivered. Blood enters the scaphoid distally. Consequently, in the event of a fracture the proximal segment of the scaphoid will be devoid of a vascular supply, and will—if action is not taken—avascularly necrose within a sufferer's snuffbox. Due to the small size of the scaphoid and its shape, it is difficult to determine, early on, whether or not the scaphoid is indeed fractured with an x-ray.

Similar presentations
















>")


 Joint and Hand>")
