Download presentation
Presentation is loading. Please wait.

1
Kayvan Karamifar, M.D Occupational Medicine Specialist

2
The Most Important Disorders Shoulder: Rotator cuff tendinitis Bicipital tendinitis Elbow : – Lateral Epicondylitis – Medial Epicondylitis – Olecranon Bursitis – Cubital Tunnel Syndrome Forearm: – Pronator Teres Syndrome – Anterior interosseous syndrome – Posterior interosseous syndrome – Intersecti on syndrome Wrist: – Carpal tunnel syndrome – DeQuervain disease – Ganglion cyst – Trigger wrist Hand: – Guyon`s canal syndrome – Hypothenar hammer syndrome – Trigger finger – Trigger thumb – Occupational hand cramp

4
Occupational Physical Stressors (Job Risk Factors) Repetition Force Awkward posture Contact stress Vibration
 Repetition Force Awkward posture Contact stress Vibration")
5
High-risk Jobs Some examples: Auto assemblers Butchers VDT users Drivers Packinghouse workers Seamstresses Musicians Clerical workers Textile workers Miners Dentists

7
Diagnosis Requirements Definite clinical diagnosis History Specific physical examination Motor, sensation, reflexes, …. Ergonomic stressors Taking occupational history Job visit and ergonomic analysis Video recording Off-the-job exposure Previous trauma

8
Treatment Methods Conservative therapy Specific splint use Medical therapy Drug therapy Corticosteroid injection Physical therapy Home exercise Occupational therapy Surgery

9
Work Accommodations Engineering control Ergonomic design modification Use tools with proper ergonomic design Administrative Reduce working hours Appropriate work-rest period Job rotation Safe work practice Temporary job transfer to low-risk job Re-training

11
Lateral Epicondylitis

12
Lateral Epicondylitis ( Tennis Elbow) Inflammation, or enthesitis, at the muscular origin of the extensor carpi radialis brevis (ECRB). the most common overuse injury of the elbow up to 10 times more frequently than medial epicondylitis most often occurs between the third and fifth decades of life.

14
Ergonomic Stressors Frequent lifting Repetitive contraction of the wrist extensors (repetitive wrist dorsiflexion with force) Sustained power gripping. Repetitive forearm supination Sudden elbow extension Tool use, shaking hand, twisting movement

15
Common Jobs Involved

16
Clinical Presentations lateral elbow pain of gradual onset. pain generally increases with activity Picking up a cup of coffee or a gallon of milk Heavy lifting Gripping Pain may be present at night. Symptoms are typically unilateral.

17
Area of Pain

18
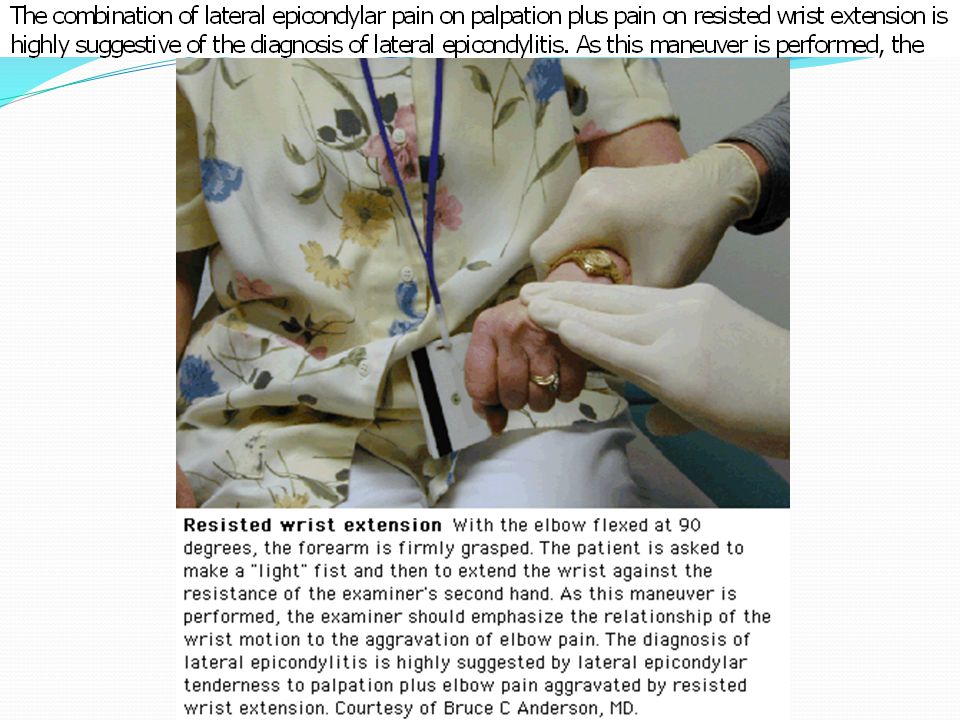
Physical Examination localized tenderness to palpation just distal and anterior to the lateral epicondyle.

20
Presumptive Diagnosis Requires: Local tenderness directly over the lateral epicondyle Pain aggravated by resisted wrist extension and radial deviation Pain aggravated by strong gripping Normal elbow range of motion

21
Paraclinical Testing No specific test is required

22
Differential Diagnosis Cervical radiculopathy ( C6-C7) Radial tunnel syndrome Synovitis of the radiohumeral joint Posterior interosseous nerve palsy Neuralgic amyotrophy Cervical myofacial pain
 Radial tunnel syndrome Synovitis of the radiohumeral joint Posterior interosseous nerve palsy Neuralgic amyotrophy Cervical myofacial pain")
25
Lateral Epicondylitis Injection

26
Splints for Tennis Elbow

28
Carpal Tunnel Syndrome (CTS) Most common entrapment neuropathy Cause: median nerve injury in carpal tunnel RF: repetition, force, awkward postures (wrist flexion, extension, ulnar deviation) Jobs: seamstresses, packinghouse workers, electronic assemblers, furniture assemblers, clerical workers, VDT users, typists, …
 Most common entrapment neuropathy Cause: median nerve injury in carpal tunnel RF: repetition, force, awkward postures (wrist flexion, extension, ulnar deviation) Jobs: seamstresses, packinghouse workers, electronic assemblers, furniture assemblers, clerical workers, VDT users, typists, …")
29
CTS (cont.) Non-occupational risk factors: female sex, obesity, small carpal tunnel Non-occupational causes: diabetes, RA, Thyroid dysfunction, amyloidosis, wrist OA, edema, acute trauma, …
 Non-occupational risk factors: female sex, obesity, small carpal tunnel Non-occupational causes: diabetes, RA, Thyroid dysfunction, amyloidosis, wrist OA, edema, acute trauma, …")
30
CTS (cont.) Carpal tunnel: Limits: wrist bones, transverse carpal ligament Traversing elements: Digital flexor tendons Flexor policis longus Median nerve
 Carpal tunnel: Limits: wrist bones, transverse carpal ligament Traversing elements: Digital flexor tendons Flexor policis longus Median nerve")
31
CTS (cont.) Signs and symptoms Early: paresthesia, hypersthesia, hyposthesia (intermittent and in dominant hand) Then: pain, numbness, clumsiness Late: progressive pain and numbness, weakness and atrophy, loss of sweating DD: TOS, C7 radiculaopathy, general neuropathy
 Signs and symptoms Early: paresthesia, hypersthesia, hyposthesia (intermittent and in dominant hand) Then: pain, numbness, clumsiness Late: progressive pain and numbness, weakness and atrophy, loss of sweating DD: TOS, C7 radiculaopathy, general neuropathy")
32
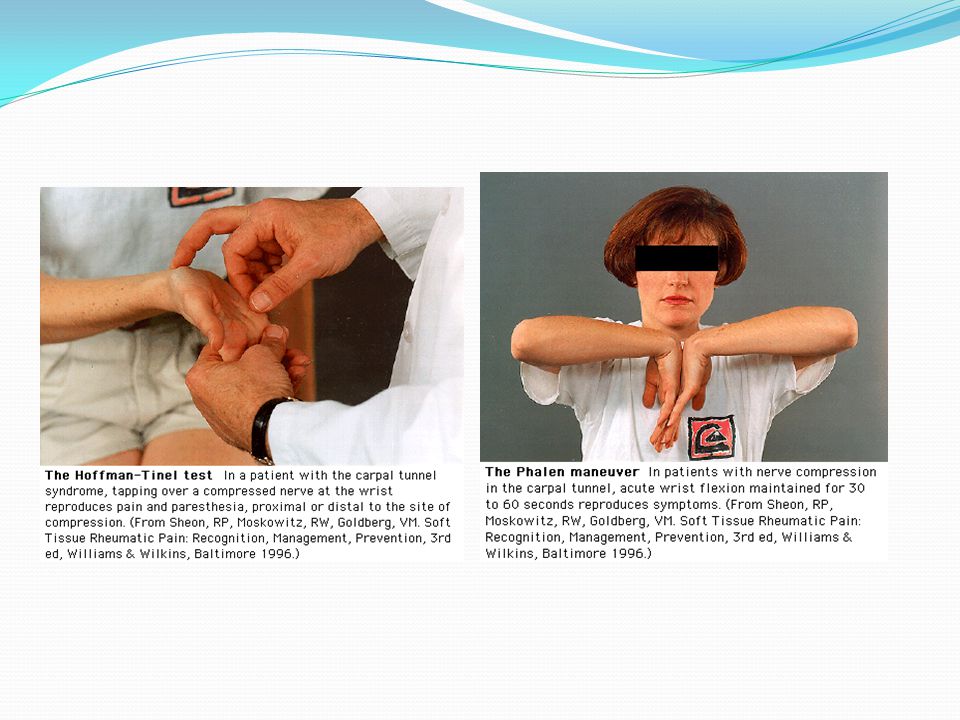
CTS (cont.) Diagnostic methods: Provocative tests Tinel Phalen Electrophysiologic tests (gold standard) Screening for diabetes, Thyroid dysfunction, and RA
 Diagnostic methods: Provocative tests Tinel Phalen Electrophysiologic tests (gold standard) Screening for diabetes, Thyroid dysfunction, and RA")
34
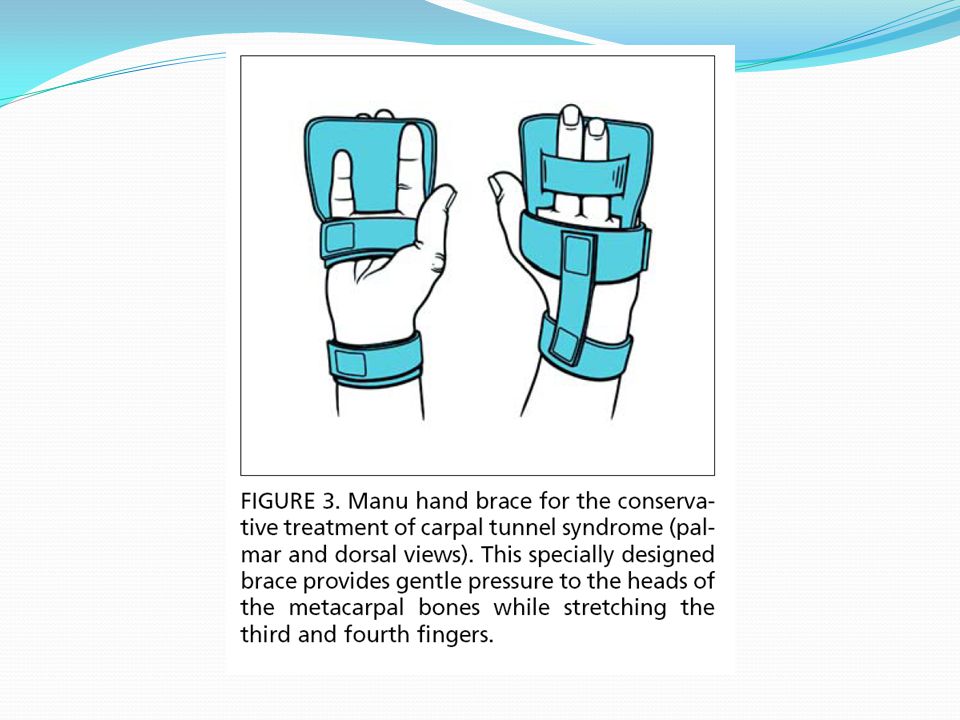
CTS (cont.) Therapy: Non-surgical: Indications: intermittent or mild symptoms, no atrophy, contraindication for surgery Methods: night splint, NSAIDs, work limitations Causes of inappropriate response: age>50, symptoms>10m., persistent paresthesia, positive phalen test in less than 30s.
 Therapy: Non-surgical: Indications: intermittent or mild symptoms, no atrophy, contraindication for surgery Methods: night splint, NSAIDs, work limitations Causes of inappropriate response: age>50, symptoms>10m., persistent paresthesia, positive phalen test in less than 30s.")
38
CTS (cont.) Surgical therapy: Indications: inappropriate response to non-surgical therapy, severe and prolonged symptoms, muscular weakness or atrophy, positive electrophysilogic tests Post-surgery problems: persistent symptoms, recurrence, median nerve injury, neuroma formation, adhesions, …
 Surgical therapy: Indications: inappropriate response to non-surgical therapy, severe and prolonged symptoms, muscular weakness or atrophy, positive electrophysilogic tests Post-surgery problems: persistent symptoms, recurrence, median nerve injury, neuroma formation, adhesions, …")
39
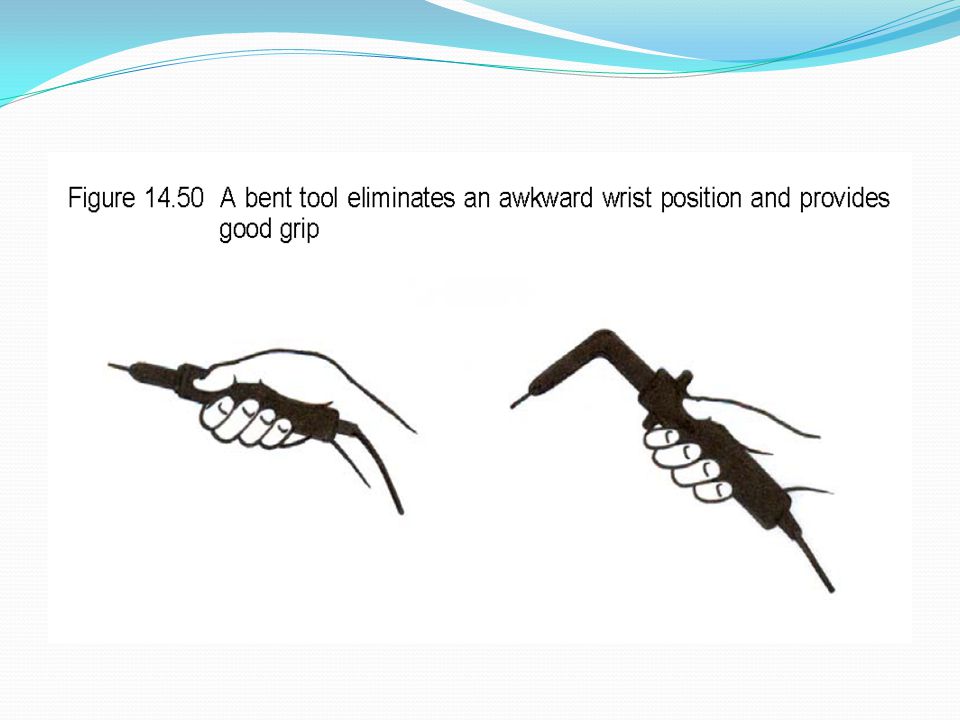
Ergonomic Modifications Depends on ergonomic stressor: VDT User: adjust workstation, ergonomic mouse, wrist pad, modify contact stress, work-rest period, ergonomic keyboard, work exercises Hand tool user: electrical hand tools, work-rest period, work exercises, ergonomic hand tools

46
Electrical Screwdriver

49
Wrist Awkward Posture

50
Ergonomic Mouse pad

52
Compression = soft tissue is compressed between the bone and a hard or sharp object Before: Worker rests his wrists on the sharp tray edges. His wrist is extended into a non-neutral posture. Ergonomic Improvement: Worker rests her wrists and forearms on a padded surface. Wrist and forearms are in a neutral position.

Similar presentations























>")


(1) of the OSH Act.>")





 Pathology Pathology 30 – 50 years old Repetitive micro-trauma Chronic tear in the origin of the extensor.>")




