Download presentation
Presentation is loading. Please wait.

1
DIAGNOSTIC ET TRAITEMENT DE L’INSUFFISANCE CARDIAQUE Prof O. Gurné UCL – Cliniques Univ St Luc

2
Heart Failure (HF) Definition A complex clinical syndrome in which the heart is incapable of maintaining a cardiac output adequate to accommodate metabolic requirements and the venous return.
 Definition A complex clinical syndrome in which the heart is incapable of maintaining a cardiac output adequate to accommodate metabolic requirements and the venous return.")
3
Etiology and Pathophysiology of Heart Failure

4
Etiology of Heart Failure What causes heart failure? The loss of a critical quantity of functioning myocardial cells after injury to the heart due to: –Ischemic Heart Disease –Hypertension –Idiopathic Cardiomyopathy –Infections (e.g., viral myocarditis) –Toxins (e.g., alcohol or cytotoxic drugs) –Valvular Disease –Prolonged Arrhythmias
 –Toxins (e.g., alcohol or cytotoxic drugs) –Valvular Disease –Prolonged Arrhythmias.")
5
30% 70% Diastolic Dysfunction Systolic Dysfunction (EF < 40%) (EF > 40 %) Left Ventricular Dysfunction Systolic: Impaired contractility/ejection –Approximately two-thirds of heart failure patients have systolic dysfunction 1 Diastolic: Impaired filling/relaxation 1 Lilly, L. Pathophysiology of Heart Disease. Second Edition p 200

6
Prevention Therapy NYHAClass IIIIIIIV Ventricular dysfunction Overt heart failure Mild Moderate Severe Progress of heart failure

7
Curry CW, et al. Mechanical dyssynchrony in dilated cardiomyopathy with intraventricular conduction delay as depicted by 3D tagged magnetic resonance imaging. Circulation 2000 Jan 4;101(1):E2. Compensatory Mechanisms Ventricular Remodeling Alterations in the heart’s size, shape, structure, and function brought about by the chronic hemodynamic stresses experienced by the failing heart.
:E2. Compensatory Mechanisms Ventricular Remodeling Alterations in the heart’s size, shape, structure, and function brought about by the chronic hemodynamic stresses experienced by the failing heart..")
8
Injury to heart Sympathetic Disease progression Neurohormonal activation Renin angiotensin aldosterone Neurohormonal activation in heart failure

9
Initially Adaptive, Deleterious if Sustained Initially Adaptive, Deleterious if Sustained Response Short-Term Effects Long-Term Effects Salt and Water RetentionAugments PreloadPulmonary Congestion, Anasarca VasoconstrictionMaintains BP for perfusion of vital organs Exacerbates pump dysfunction (excessive afterload), increases cardiac energy expenditure Sympathetic StimulationIncreases HR and ejection Increases energy expenditure Neurohormonal Responses to Impaired Cardiac Performance Jaski, B, MD: Basics of Heart Failure: A Problem Solving Approach
, increases cardiac energy expenditure Sympathetic StimulationIncreases HR and ejection Increases energy expenditure Neurohormonal Responses to Impaired Cardiac Performance Jaski, B, MD: Basics of Heart Failure: A Problem Solving Approach")
10
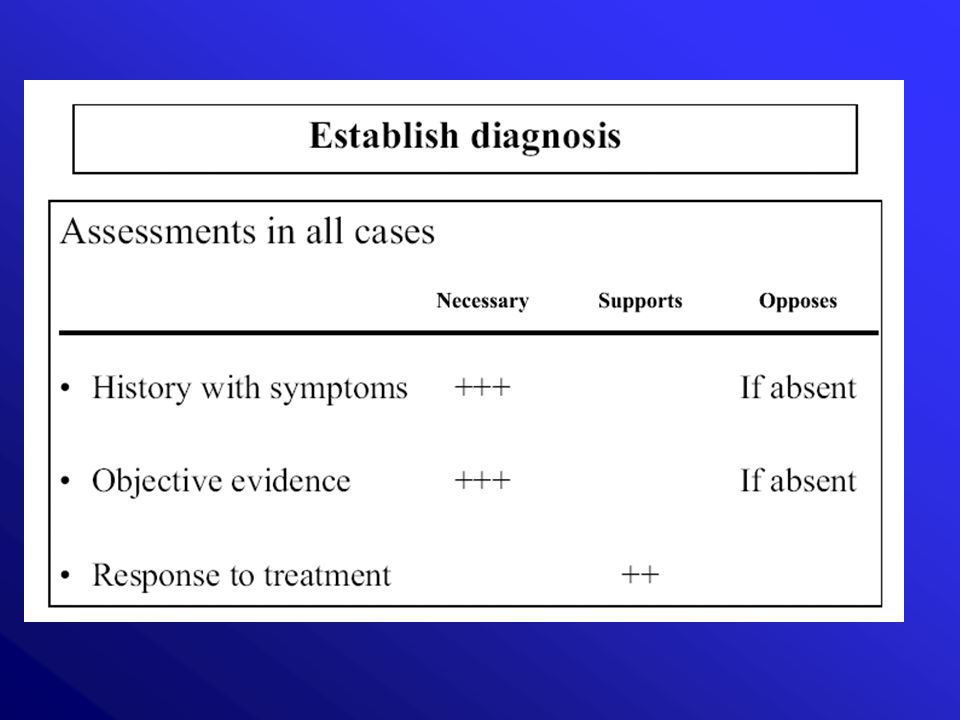
Diagnostic of Heart Failure

12
Left Ventricular Dysfunction Systolic and Diastolic Symptoms –Dyspnea on Exertion –Paroxysmal Nocturnal Dyspnea –Tachycardia –Cough –Hemoptysis Physical Signs –Basilar Rales –Pulmonary Edema –S3 Gallop –Pleural Effusion –Cheyne-Stokes Respiration

13
Right Ventricular Failure Systolic and Diastolic Symptoms –Abdominal Pain –Anorexia –Nausea –Bloating –Swelling Physical Signs –Peripheral Edema –Jugular Venous Distention –Abdominal-Jugular Reflux –Hepatomegaly

20
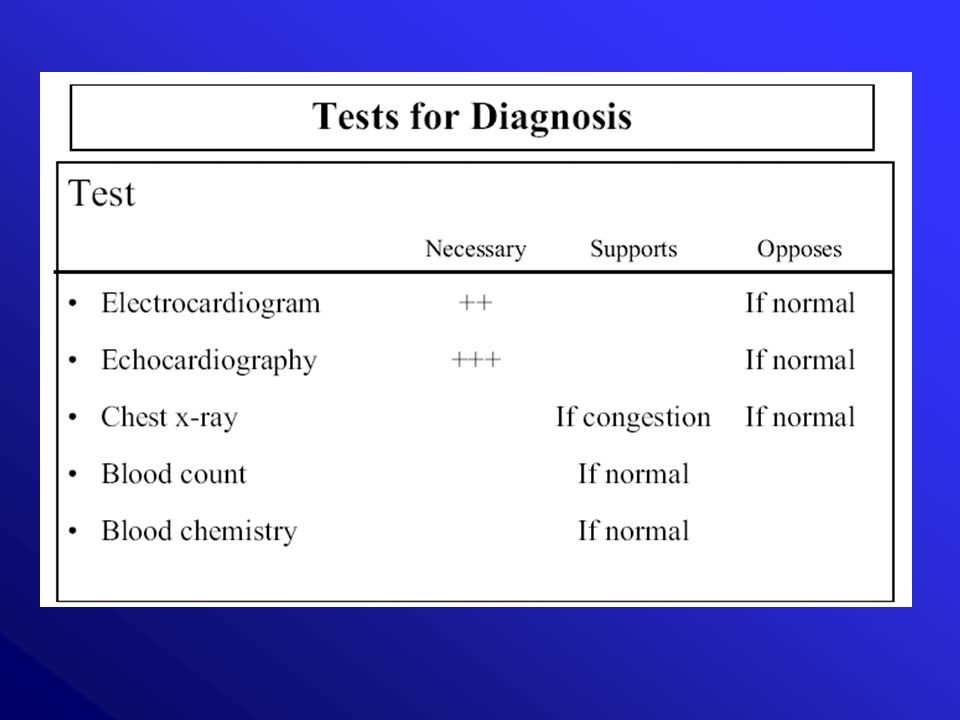
Patient suspected to have LVD Echocardiogram ECG Chest X-ray Lung function tests Full blood count Thyroid function tests Biochemistry Current diagnostic algorithm

22
Natriuretic Peptides: Origin and Stimulus of Release Adapted from Burnett JC, J Hypertens 2000;17(Suppl 1):S37-S43 ANP = Atrial Natriuretic Peptide BNP = B-type Natriuretic Peptide CNP = C-type Natriuretic Peptide PeptidePrimary OriginStimulus of Release ANPCardiac atriaAtrial distension BNPVentricular myocardiumVentricular overload CNPEndothelium Endothelial stress
:S37-S43 ANP = Atrial Natriuretic Peptide BNP = B-type Natriuretic Peptide CNP = C-type Natriuretic Peptide PeptidePrimary OriginStimulus of Release ANPCardiac atriaAtrial distension BNPVentricular myocardiumVentricular overload CNPEndothelium Endothelial stress")
23
BNP LEVELS IN PATIENTS WITN DYSPNEA Morrison et al, J Am Coll Cardiol 2002;39:202

24
100 200 300 400 500 0 600 Pulmponary Asthma COPD Pneumonia Acute Tbc Lung Pulmonary fibrosis bronchitis cancer Embolism n = 1 11 42 8 14 2 4 3 Types of Lung Disease BNP (pg/ml) Morrison et al, J Am Coll Cardiol 2002;39:202
 Morrison et al, J Am Coll Cardiol 2002;39:202")
25
ROC Curves for BNP and ED Diagnosis Using All 250 Patients Dao, Q., Maisel, A. et al. J. American College of Cardiology, Vol 37, No. 2, 2001 0102030405060708090100 0 10 20 30 40 50 60 70 80 90 100 1 - Specificity (%) Sensitivity (%) --- BNP--- ED diagnosis AUC0.8840.9790
 Sensitivity (%) --- BNP--- ED diagnosis AUC")
26
BNP in LV Dysfunction N=105 N=53 N=42 N=14 Maisel, A., De Maria, A. et al. American Heart Journal, Vol. 141, No. 3, 2001

27
Patient suspected to have LVD Echocardiogram BNP Increased Normal LVD unlikely Future diagnostic algorithm

29
Treatment of Heart Failure

30
General Measures Lifestyle Modifications: Weight reduction Discontinue smoking Avoid alcohol and other cardiotoxic substances Exercise Medical Considerations: Treat HTN, hyperlipidemia, diabetes, arrhythmias Coronary revascularization Anticoagulation Immunization Sodium restriction Daily weights Close outpatient monitoring

31
TRAITEMENT INSUFFISANCE CARDIAQUE III AIIBIIIIV DIUR ACE - INH INH A II B SPIRO DIG

32
Digitalis and Inotropic Agents Compounds Like the carrot placed in front of the donkey

33
Digoxine in heart failure Digoxine better Placebo better DIG trial –Overall death –Hospitalization 0.99 0.82 NEJM 1997; 336 : 525-533 MORTALITYDIGOXINPLACEBORRPVALUE WORSENING CHF 11.6 %13.2 %0.88 (0.77-1.01) 0.06 OTHER CARDIAC 15.0 %13.0 %1.14 (1.01-1.30) 0.04 BUTBUT
 0.06 OTHER CARDIAC 15.0 %13.0 %1.14 ( ) 0.04 BUTBUT")
34
Diuretics, ACE Inhibitors Reduce the number of sacks on the wagon

36
SOLVD Investigators N Engl J Med 1991;325:293-302 0 10 20 30 40 50 0612182430364248 Placebo Enalapril Follow-up (months) Mortality (%) Risk reduction 16% p=0.0036 Studies of Left Ventricular Dysfunction – SOLVD (Treatment Study)
 Mortality (%) Risk reduction 16% p= Studies of Left Ventricular Dysfunction – SOLVD (Treatment Study)")
37
ACE INHIBITORS - IN WHOM AND WHEN? Indications: potentially all patients with heart failure 1st line treatment (along with beta-blockers) in NYHA class I-IV heart failure Contra-indications: history of angioneurotic oedema Cautions: significant renal dysfunction (creatinine > 2.5 mg/dL or 221 µmol/L ) or hyperkalaemia (K + > 5.0 mmol/L) symptomatic or severe asymptomatic hypotension (SBP < 90 mmHg) Drug interactions to look out for: K + supplements/ K + sparing diuretics (including spironolactone) NSAIDs avoid unless essential AT 1 -receptor blockers
 in NYHA class I-IV heart failure Contra-indications: history of angioneurotic oedema Cautions: significant renal dysfunction (creatinine > 2.5 mg/dL or 221 µmol/L ) or hyperkalaemia (K + > 5.0 mmol/L) symptomatic or severe asymptomatic hypotension (SBP < 90 mmHg) Drug interactions to look out for: K + supplements/ K + sparing diuretics (including spironolactone) NSAIDs avoid unless essential AT 1 -receptor blockers.")
38
ACE INHIBITORS - HOW TO USE start with a low dose Increase dose progressively aim for target dose or, failing that, the highest tolerated dose remember some ACE inhibitor is better than no ACE inhibitor monitor blood chemistry (urea, creatinine, K + ) and blood pressure
 and blood pressure")
39
ACE INHIBITORS - PROBLEM SOLVING Asymptomatic low blood pressure does not usually require any change in therapy Symptomatic hypotension: if dizziness, light-headedness and/or confusion and a low blood pressure occurs, reconsider need for nitrates, calcium channel blockers** and other vasodilators if no signs/symptoms of congestion, consider reducing diuretic dose **calcium channel blockers should be discontinued unless absolutely essential (eg. for angina or hypertension)
.")
40
ACE INHIBITORS - PROBLEM SOLVING (cont.) Cough: cough is common in patients with heart failure, many of whom have smoking-related lung disease cough is also a symptom of pulmonary oedema which should be excluded if a new or worsening cough develops ACE inhibitor-induced cough rarely requires treatment discontinuation: ± 5 – 10 % max if a very troublesome cough develops (eg. one stopping the patient sleeping) and can be proven to be due to ACE inhibition (ie. recurs after ACE inhibitor withdrawal and rechallenge) substitution with an AT 1 -receptor blocker can be considered
 and can be proven to be due to ACE inhibition (ie. recurs after ACE inhibitor withdrawal and rechallenge) substitution with an AT 1 -receptor blocker can be considered.")
41
ACE INHIBITORS - PROBLEM SOLVING (cont.) Worsening renal function: some increase in urea (blood urea nitrogen), creatinine and K + is to be expected after initiation; if the increase is “small” and asymptomatic no action is necessary an increase in creatinine of up to 50% above baseline, or 3 mg/dL (266 µmol/L), whichever is the smaller, is acceptable an increase in K + 6.0 mmol/L is acceptable if urea, creatinine or K + rise excessively consider stopping concomitant nephrotoxic drugs (eg. NSAIDs), other K + supplements/ K + retaining agents (triamterene, amiloride) and, if no signs of congestion, reducing the dose of diuretic if greater rises in creatinine or K + than those outlined above persist despite adjustment of concomitant medications, halve the dose of ACE inhibitor and recheck blood chemistry; if there is still an unsatisfactory response, check for renal artery stenosis
, other K + supplements/ K + retaining agents (triamterene, amiloride) and, if no signs of congestion, reducing the dose of diuretic if greater rises in creatinine or K + than those outlined above persist despite adjustment of concomitant medications, halve the dose of ACE inhibitor and recheck blood chemistry; if there is still an unsatisfactory response, check for renal artery stenosis.")
42
ACE INHIBITORS - PROBLEM SOLVING (cont.) Worsening renal function (cont.): If K + rises to > 6.0 mmol/L or creatinine increases by >100% or to above 4 mg/dL (354 µmol/L), the dose of ACE inhibitor should be stopped Blood chemistry should be monitored serially until K + and creatinine have plateaued NB: it is very rarely necessary to stop an ACE inhibitor and clinical deterioration is likely if treatment is withdrawn
 Worsening renal function (cont.): If K + rises to > 6.0 mmol/L or creatinine increases by >100% or to above 4 mg/dL (354 µmol/L), the dose of ACE inhibitor should be stopped Blood chemistry should be monitored serially until K + and creatinine have plateaued NB: it is very rarely necessary to stop an ACE inhibitor and clinical deterioration is likely if treatment is withdrawn")
43
B lockade of RAS ANGIOTENSIN I ANGIOTENSINOGEN (LIVER) AT 1 AT 2 ANGIOTENSIN II ACE INHIBITOR AT 1 RECEPTOR BLOCKER RENIN INHIBITOR BRADYKININ PEPTIDES CHYMASE LOCAL ANG II SYNTHESIS IS INDEPENDENT OF ACE
 AT 1 AT 2 ANGIOTENSIN II ACE INHIBITOR AT 1 RECEPTOR BLOCKER RENIN INHIBITOR BRADYKININ PEPTIDES CHYMASE LOCAL ANG II SYNTHESIS IS INDEPENDENT OF ACE")
44
A Biollaz et al. J Cardiovasc Pharmacol 1982;4:966 NG II levels increase over time despite ACEI HOSPITAL 0 4 8 12 16 20 24 PLACEBO 4H24H123456 MONTHS 80 100 120 140 160 180 BLOOD PRESSURE mm Hg PLASMA ANG II pg/mL

45
NYHA III* or IV heart failure LVEF 35% ACE-I + loop diuretic ± digoxin NYHA III* or IV heart failure LVEF 35% ACE-I + loop diuretic ± digoxin Spironolactone 25 mg/day (n = 822) Spironolactone 25 mg/day (n = 822) Primary Endpoint Total mortality Secondary Endpoint Cardiac mortality Cardiac hospitalization Cardiac mortality or cardiac hosptitalization Changes from baseline in NYHA classification Primary Endpoint Total mortality Secondary Endpoint Cardiac mortality Cardiac hospitalization Cardiac mortality or cardiac hosptitalization Changes from baseline in NYHA classification Placebo (n = 841) Placebo Pitt et al, N Engl J Med, 1999. *History of NYHA IV within 6 months before first dose 3 years RALES: Study Design

46
0.00 0.45 0.50 0.55 0.60 0.65 0.70 0.75 0.80 0.85 0.90 0.95 1.00 0369121518212427303336 Spironolactone Placebo Probability of survival Months Randomized Aldactone Evaluation Study (RALES) All causes mortality Pitt B et al. N Engl J Med 1999;10:709-717 Risk reduction 30% 95% CI : 18-40 % p<0.001

49
SPIRONOLACTONE - IN WHOM AND WHEN? Indications: potentially all patients with symptomatically moderately severe or severe heart failure 2nd line therapy (after ACE inhibitors and beta-blockers) in patients with NYHA class III-IV heart failure Cautions: significant renal dysfunction (creatinine > 221 µ mol/L or 2.5 mg/dL) significant hyperkalaemia (K + > 5.0 mmol/L)
 in patients with NYHA class III-IV heart failure Cautions: significant renal dysfunction (creatinine > 221 µ mol/L or 2.5 mg/dL) significant hyperkalaemia (K + > 5.0 mmol/L).")
50
SPIRONOLACTONE - HOW TO USE start at 25 mg once daily(12.5) check blood chemistry at 1, 4, 8 and 12 weeks; 6, 9 and 12 months; 6 monthly thereafter if K + rises to between 5.5 and 6.0 mmol/L or creatinine rises to 2.5 mg/dL (221 µmol/L) reduce dose to 25 mg on alternate days and monitor blood chemistry closely if K + rises to > 6.0 mmol/L or creatinine to > 4.0 mg/dL (354 µmol/L), stop spironolactone
 check blood chemistry at 1, 4, 8 and 12 weeks; 6, 9 and 12 months; 6 monthly thereafter if K + rises to between 5.5 and 6.0 mmol/L or creatinine rises to 2.5 mg/dL (221 µmol/L) reduce dose to 25 mg on alternate days and monitor blood chemistry closely if K + rises to > 6.0 mmol/L or creatinine to > 4.0 mg/dL (354 µmol/L), stop spironolactone")
51
Vasoconstriction Hypertrophy Inotrope + Chronotrope + Hypertrophy (HVG) Fibrosis sodium and water retention Vasoconstriction of afferent and efferent arterioles Aldosterone secretion Catecholamines secretion Stimulation thirst center Vasopressin release sympathetic activation AT 1 ANGIOTENSINE II Goodfriend et al. N Engl J Med 1996;334:1649-1654 Jackson and Garrisson. In: Hardman et al. eds. Goodman & Gilman ’s The Pharmacological Basis of Therapeutics 9th ed. New York: McGraw Hill: 1996;733-758 Bauer and Reams Arch Intern Med 1995;155:1361-1368 E ffects of Angiotensin II via AT 1 receptors

52
Study Design Losartan Heart Failure Survival Study ELITE II 60 yrs; NYHA II-IV; EF 40% ACE-I/AIIA naive or <7 days in 3 months prior to entry Standard Rx (± Dig/Diuretics), ß-blocker stratification Captopril 50 mg 3 times daily (N=1574) Primary Endpoint: All-Cause Mortality Secondary Endpoint: Sudden Cardiac Death and/or Resuscitated Arrest Other Endpoin: All-cause Mortality/Hospitalizations Safety and Tolerability Event Driven (Target 510 Deaths) ~ 2 years Losartan 50 mg Daily (N=1578)
, ß-blocker stratification Captopril 50 mg 3 times daily (N=1574) Primary Endpoint: All-Cause Mortality Secondary Endpoint: Sudden Cardiac Death and/or Resuscitated Arrest Other Endpoin: All-cause Mortality/Hospitalizations Safety and Tolerability Event Driven (Target 510 Deaths) ~ 2 years Losartan 50 mg Daily (N=1578)")
53
Losartan Heart Failure Survival Study - ELITE II Primary Endpoint: All-Cause Mortality 0100200300400500600700 Days of Follow-up 0.0 0.2 0.4 0.6 0.8 1.0 Probability of Survival Losartan (N=1578)280 Events Captopril(N=1574) 250 Events Captopril/Losartan Hazard Ratio (95% C.I.): 0.88 (0.75, 1.05) P=0.16
280 Events Captopril(N=1574) 250 Events Captopril/Losartan Hazard Ratio (95% C.I.): 0.88 (0.75, 1.05) P=0.16")
54
CHARM Added CHARM Preserved CHARM Programme 3 component trials comparing candesartan to placebo in patients with symptomatic heart failure CHARM Alternative n=2028 LVEF 40% ACE inhibitor intolerant n=2548 LVEF 40% ACE inhibitor treated n=3025 LVEF >40% ACE inhibitor treated/not treated Primary outcome for Overall Programme: All-cause death Primary outcome for each trial: CV death or CHF hospitalisation

55
n=3025 LVEF >40% ACE inhibitor treated/not treated CHARM Added CHARM Preserved CHARM Alternative n=2028 LVEF 40% ACE inhibitor intolerant n=2548 LVEF 40% ACE inhibitor treated Primary outcome: CV death or CHF hosp CHARM Programme 3 component trials comparing candesartan to placebo in patients with symptomatic heart failure

56
CHARM-Alternative: Primary outcome CV death or CHF hospitalisation 0123years 0 10 20 30 40 50 Placebo Candesartan % HR 0.77 (95% CI 0.67-0.89), p=0.0004 Adjusted HR 0.70, p<0.0001 Number at risk Candesartan 1013929831434122 Placebo 1015887798427126 3.5 406 (40.0%) 334 (33.0%)
, p= Adjusted HR 0.70, p< Number at risk Candesartan Placebo (40.0%) 334 (33.0%)")
57
n=3025 LVEF >40% ACE inhibitor treated/not treated CHARM Added CHARM Preserved CHARM Alternative n=2028 LVEF 40% ACE inhibitor intolerant n=2548 LVEF 40% ACE inhibitor treated Primary outcome: CV death or CHF hosp CHARM Programme 3 component trials comparing candesartan to placebo in patients with symptomatic heart failure

58
CHARM-Added: Primary outcome CV death or CHF hospitalisation 0123years 0 10 20 30 40 50 Placebo Candesartan Number at risk Candesartan127611761063948457 Placebo127211361013906422 3.5 HR 0.85 (95% CI 0.75-0.96), p=0.011 Adjusted HR 0.85, p=0.010 483 (37.9%) 538 (42.3%) %
, p=0.011 Adjusted HR 0.85, p= (37.9%) 538 (42.3%) %")
59
n=3025 LVEF >40% ACE inhibitor treated/not treated CHARM Added CHARM Preserved CHARM Alternative n=2028 LVEF 40% ACE inhibitor intolerant n=2548 LVEF 40% ACE inhibitor treated Primary outcome: CV death or CHF hosp CHARM Programme 3 component trials comparing candesartan to placebo in patients with symptomatic heart failure

60
CHARM-Preserved: Primary outcome CV death or CHF hospitalisation 0123years Number at risk Candesartan 151414581377833182 Placebo 150914411359824195 3.5 0 10 20 30 Placebo Candesartan 5 15 25 HR 0.89 (95% CI 0.77-1.03), p=0.118 Adjusted HR 0.86, p=0.051 % 366 (24.3%) 333 (22.0%)
, p=0.118 Adjusted HR 0.86, p=0.051 % 366 (24.3%) 333 (22.0%)")
61
ß-Blockers Limit the donkey’s speed, thus saving energy

62
Carvedilol (n=696) Placebo (n=398) Survival Days 050100150200250300350400 1.0 0.9 0.8 0.7 0.6 0.5 Risk reduction = 65% p<0.001 Packer et al (1996) Lancet (1999) 0 200 400 600 800 1.0 0.8 0.6 0 Bisoprolol Placebo Time after inclusion (days) p<0.0001 Survival Risk reduction = 34% The MERIT-HF Study Group (1999) Months of follow-up Mortality % 036912151821 20 15 10 5 0 Placebo Metoprolol CR/XL p=0.0062 Risk reduction = 34% US Carvedilol Study blockers in heart failure - all-cause mortality CIBIS-II MERIT-HF
 Placebo (n=398) Survival Days Risk reduction = 65% p<0.001 Packer et al (1996) Lancet (1999) Bisoprolol Placebo Time after inclusion (days) p< Survival Risk reduction = 34% The MERIT-HF Study Group (1999) Months of follow-up Mortality % Placebo Metoprolol CR/XL p= Risk reduction = 34% US Carvedilol Study blockers in heart failure - all-cause mortality CIBIS-II MERIT-HF")
63
COPERNICUS Patient Characteristics Symptoms of heart failure at rest or minimal exertion for at least 2 months LV ejection fraction <25% Receiving diuretics and an ACE inhibitor (+ digitalis) 2 months. Diuretics optimised to achieve euvolaemia No need for intensive care and no treatment with IV inotropic or IV vasodilator therapy within 4 days of screening

64
0 0 % Survival 36912151821 Months 100 90 80 60 70 p=0.00013 35% risk reduction Carvedilol Placebo COPERNICUS All-cause mortality

65
Randomised3029 Carvedilol1511Metoprolol1518 Assigned to drug and received at least one tablet Withdrew consent 10 Lost to follow-up 3 Withdrew consent 18 Lost to follow-up 2 Flow chart of patients

66
Time (years) Mortality (%) 0 10 20 30 40 012345 Metoprolol Carvedilol hazard ratio 0.83, 95% CI 0.74-0.93, P = 0.0017 Number at risk Carvedilol151113671259 11551002383 Metoprolol151813591234 1105933352 Primary endpoint of mortality
 Mortality (%) Metoprolol Carvedilol hazard ratio 0.83, 95% CI , P = Number at risk Carvedilol Metoprolol Primary endpoint of mortality")
67
BETA-BLOCKERS - IN WHOM AND WHEN? Indications: potentially all patients with stable mild and moderate heart failure; patients with severe heart failure should be referred for specialist advice 1st line treatment (along with ACE inhibitors) in patients with stable NYHA class I-III heart failure; start as early as possible Contra-indications: asthma Cautions: severe (NYHA Class IV) heart failure ( ! COPERNICUS) current or recent (< 4 weeks) exacerbation of heart failure eg. hospital admission with worsening heart failure heart block or heart rate < 60 beats/min persisting signs of congestion – raised jugular venous pressure, ascites, marked peripheral oedema
 in patients with stable NYHA class I-III heart failure; start as early as possible Contra-indications: asthma Cautions: severe (NYHA Class IV) heart failure ( . COPERNICUS) current or recent (< 4 weeks) exacerbation of heart failure eg. hospital admission with worsening heart failure heart block or heart rate < 60 beats/min persisting signs of congestion – raised jugular venous pressure, ascites, marked peripheral oedema.")
68
BETA-BLOCKERS - IN WHOM AND WHEN? (cont.) Drug interactions to look out for: verapamil/diltiazem (should be discontinued) amiodarone BETA-BLOCKERS - WHERE? in the community in stable patients (NYHA class IV/severe heart failure patients should be referred for specialist advice) not in unstable patients hospitalised with worsening heart failure other exceptions – see CAUTIONS
 Drug interactions to look out for: verapamil/diltiazem (should be discontinued) amiodarone BETA-BLOCKERS - WHERE. in the community in stable patients (NYHA class IV/severe heart failure patients should be referred for specialist advice) not in unstable patients hospitalised with worsening heart failure other exceptions – see CAUTIONS.")
69
BETA-BLOCKERS - HOW TO USE start with a low dose double dose at not less than 2 weekly intervals aim for target dose or, failing that, the highest tolerated dose remember some beta-blocker is better than no beta-blocker monitor HR, BP, clinical status (symptoms, signs – especially signs of congestion) and body weight) check blood chemistry 1-2 weeks after initiation and 1-2 weeks after final dose titration a specialist heart failure nurse may assist with patient education, follow-up (in person/by telephone) and dose up- titration when to down-titrate/stop up-titration – see PROBLEM SOLVING
 and body weight) check blood chemistry 1-2 weeks after initiation and 1-2 weeks after final dose titration a specialist heart failure nurse may assist with patient education, follow-up (in person/by telephone) and dose up- titration when to down-titrate/stop up-titration – see PROBLEM SOLVING")
70
BETA-BLOCKERS - ADVICE TO PATIENT explain expected benefits (see WHY?) emphasise that treatment given as much to prevent worsening of heart failure as to improve symptoms; beta-blockers also increase survival if symptomatic improvement occurs, this may develop slowly, 3 - 6 months or longer temporary symptomatic deterioration may occur (estimated 20 - 30% of cases) during initiation/up- titration phase
 emphasise that treatment given as much to prevent worsening of heart failure as to improve symptoms; beta-blockers also increase survival if symptomatic improvement occurs, this may develop slowly, months or longer temporary symptomatic deterioration may occur (estimated % of cases) during initiation/up- titration phase")
71
BETA-BLOCKERS - ADVICE TO PATIENT (cont.) advise patient to report deterioration (see PROBLEM SOLVING) and that deterioration (tiredness, fatigue, breathlessness) can usually be easily managed by adjustment of other medication; patients should be advised not to stop beta-blocker therapy without consulting their physician patients should be encouraged to weigh themselves daily (after waking, before dressing, after voiding, before eating) and to increase their diuretic dose should their weight increase, persistently (> 2 days), by >1.5 – 2.0 kg
 advise patient to report deterioration (see PROBLEM SOLVING) and that deterioration (tiredness, fatigue, breathlessness) can usually be easily managed by adjustment of other medication; patients should be advised not to stop beta-blocker therapy without consulting their physician patients should be encouraged to weigh themselves daily (after waking, before dressing, after voiding, before eating) and to increase their diuretic dose should their weight increase, persistently (> 2 days), by >1.5 – 2.0 kg")
72
BETA-BLOCKERS - PROBLEM SOLVING Worsening symptoms/signs (eg. increasing dyspnoea, fatigue, oedema, weight gain): if increasing congestion, double dose of diuretic and/or halve dose of beta-blocker (if increasing diuretic does not work) if marked fatigue (and/or bradycardia – see below) halve dose of beta-blocker (rarely necessary) review patient in 1-2 weeks; if not improved seek specialist advice if serious deterioration halve dose of beta-blocker or stop this treatment (rarely necessary); seek specialist advice
: if increasing congestion, double dose of diuretic and/or halve dose of beta-blocker (if increasing diuretic does not work) if marked fatigue (and/or bradycardia – see below) halve dose of beta-blocker (rarely necessary) review patient in 1-2 weeks; if not improved seek specialist advice if serious deterioration halve dose of beta-blocker or stop this treatment (rarely necessary); seek specialist advice.")
73
BETA-BLOCKERS - PROBLEM SOLVING (cont.) Low heart rate: if < 50 beats/min and worsening symptoms – halve dose beta-blocker or, if severe deterioration, stop beta-blocker (rarely necessary) review need for other heart rate slowing drugs eg. digoxin, amiodarone, diltiazem arrange ECG to exclude heart block

74
BETA-BLOCKERS - PROBLEM SOLVING (cont.) Asymptomatic low blood pressure: does not usually require any change in therapy Symptomatic hypotension: if dizziness, light-headedness and/or confusion and a low blood pressure occur, reconsider need for nitrates, calcium channel blockers and other vasodilators if no signs/symptoms of congestion, consider reducing diuretic dose NOTE: Beta-blockers should not be stopped suddenly unless absolutely necessary (there is a risk of a “rebound” increase in myocardial ischaemia/infarction and arrhythmias) – ideally specialist advice should be sought before treatment discontinuation
 Asymptomatic low blood pressure: does not usually require any change in therapy Symptomatic hypotension: if dizziness, light-headedness and/or confusion and a low blood pressure occur, reconsider need for nitrates, calcium channel blockers and other vasodilators if no signs/symptoms of congestion, consider reducing diuretic dose NOTE: Beta-blockers should not be stopped suddenly unless absolutely necessary (there is a risk of a rebound increase in myocardial ischaemia/infarction and arrhythmias) – ideally specialist advice should be sought before treatment discontinuation")
75
How could we do better than better … perhaps one day ? Treatment of Heart Failure

76
HEART FAILURE - TREATMENT MEDICAL THERAPY TECHNICAL DEVICE –Biventricular pacing –Défibillateur implantable –Assist devices –Artificial heart Bridge to transplant Permanent GENE / CELLULAR THERAPY

77
Cardiac Resynchronization Therapy Increase the donkey’s (heart) efficiency
 efficiency")
78
BIVENTRICULAR PACING in CHF “Conventional” target population High functional class (NYHA III or IV) Prolonged QRS ( > 150 ms) Dilated LV with EF <0.35 PR interval > 150 ms Relative clinical stability... % of CHF patients reflect these findings !

79
(4) Lancet 1998; 352 : SI15-SI18 Structure of heart failure clinic Effect of Multidisciplinary Intervention in Treatment of Heart Failure In-hospital patient Cardiologist Nursing Dietician Physiotherapist Out- patient GP Home nursing Social services
 Lancet 1998; 352 : SI15-SI18 Structure of heart failure clinic Effect of Multidisciplinary Intervention in Treatment of Heart Failure In-hospital patient Cardiologist Nursing Dietician Physiotherapist Out- patient GP Home nursing Social services")
80
EXEMPLE : EDUCATION DU PATIENT DEBUTE A L’HOPITAL POURSUIVI A LA MAISON Connaissance de sa pathologie Relation avec sa médication Relation avec son hygiène de vie, son régime Connaissance des signes précoces de décompensation Ex: prise du poids

Similar presentations













 Class IV: symptoms at rest Class III: symptoms on less-than-ordinary exertion Class.>")







 Garrett J. Gross, Ph.D. Drugs Used In the Treatment of Congestive Heart Failure(Cont) Garrett.>")


 failure is the state in which the heart is unable to pump blood.>")



