Download presentation
Presentation is loading. Please wait.

1
DIABETES INSENSATE FOOT October 27, 2005 Michael S. Brogan, PT, DPT, PhD, CWS

2
Statement of the Problem Diabetes is the 6 th leading cause of death in the U.S. (1) Diabetes is the 6 th leading cause of death in the U.S. (1) From 1990 to 1998 prevalence of diabetes increased from 4.9 to 6.5% (2) From 1990 to 1998 prevalence of diabetes increased from 4.9 to 6.5% (2) Approximately 800,000 cases of diabetes are diagnosed each year in the U.S. (3) Approximately 800,000 cases of diabetes are diagnosed each year in the U.S. (3) Approximately 17 million Americans (6.2% of pop.) have diabetes – 5.9 million of them undiagnosed (3) Approximately 17 million Americans (6.2% of pop.) have diabetes – 5.9 million of them undiagnosed (3) Another 16 million have pre-diabetes (impaired glucose tolerance) (3) Another 16 million have pre-diabetes (impaired glucose tolerance) (3)
 Diabetes is the 6 th leading cause of death in the U.S. (1) From 1990 to 1998 prevalence of diabetes increased from 4.9 to 6.5% (2) From 1990 to 1998 prevalence of diabetes increased from 4.9 to 6.5% (2) Approximately 800,000 cases of diabetes are diagnosed each year in the U.S. (3) Approximately 800,000 cases of diabetes are diagnosed each year in the U.S. (3) Approximately 17 million Americans (6.2% of pop.) have diabetes – 5.9 million of them undiagnosed (3) Approximately 17 million Americans (6.2% of pop.) have diabetes – 5.9 million of them undiagnosed (3) Another 16 million have pre-diabetes (impaired glucose tolerance) (3) Another 16 million have pre-diabetes (impaired glucose tolerance) (3).")
3
Complications of Diabetes Particularly devastating to the foot, often leading to amputation, if not treated early (4) Particularly devastating to the foot, often leading to amputation, if not treated early (4) 67% of hospital discharges for lower extremity amputations in 1997 were related to diabetes (4) 67% of hospital discharges for lower extremity amputations in 1997 were related to diabetes (4) 85% of diabetes-related amputations are preceded by the appearance of a foot ulcer (5) 85% of diabetes-related amputations are preceded by the appearance of a foot ulcer (5) Between 1989 and 1992, an average of 54,000 diabetic amputations were performed (6) Between 1989 and 1992, an average of 54,000 diabetic amputations were performed (6) In 1996, 86,000 people with diabetes underwent 1 or more lower extremity amputations (6) In 1996, 86,000 people with diabetes underwent 1 or more lower extremity amputations (6) Total cost for those amputations - > $1.1 billion dollars (7) Total cost for those amputations - > $1.1 billion dollars (7) In 1995, average individual cost of a minor amputation was $43,000, and a major amputation was $65,000 (8) In 1995, average individual cost of a minor amputation was $43,000, and a major amputation was $65,000 (8)
 Particularly devastating to the foot, often leading to amputation, if not treated early (4) 67% of hospital discharges for lower extremity amputations in 1997 were related to diabetes (4) 67% of hospital discharges for lower extremity amputations in 1997 were related to diabetes (4) 85% of diabetes-related amputations are preceded by the appearance of a foot ulcer (5) 85% of diabetes-related amputations are preceded by the appearance of a foot ulcer (5) Between 1989 and 1992, an average of 54,000 diabetic amputations were performed (6) Between 1989 and 1992, an average of 54,000 diabetic amputations were performed (6) In 1996, 86,000 people with diabetes underwent 1 or more lower extremity amputations (6) In 1996, 86,000 people with diabetes underwent 1 or more lower extremity amputations (6) Total cost for those amputations - > $1.1 billion dollars (7) Total cost for those amputations - > $1.1 billion dollars (7) In 1995, average individual cost of a minor amputation was $43,000, and a major amputation was $65,000 (8) In 1995, average individual cost of a minor amputation was $43,000, and a major amputation was $65,000 (8)")
4
Common Skin Disorders Associated With Diabetes Diabetic Dermopathy – Diabetic Dermopathy – round, reddish-brown papules (lower leg) round, reddish-brown papules (lower leg)
 round, reddish-brown papules (lower leg)")
5
Bullous Diabeticorum (upper & lower extremities)
")
6
Common Skin Disorders Associated With Diabetes Necrobiosis Lipoidica Necrobiosis Lipoidica

7
Common Skin Disorders Associated With Diabetes Diabetic Finger Pebbles Diabetic Finger Pebbles

8
Diabetic Foot Ulcers

9
Causes of Foot Ulcerations Peripheral neuropathy most common cause Peripheral neuropathy most common cause Sensory Loss Without Sensory Loss Ulceration Rarely Occurs Sensory Loss Without Sensory Loss Ulceration Rarely Occurs Mechanical Stress – repetitive tissue injury Mechanical Stress – repetitive tissue injury Lack of painful feedback

10
Further Causes of Ulceration Mechanical Stress Mechanical Stress Pressure Pressure Shear Shear Intrinsic Factors Intrinsic Factors Foot Deformities - bony prominences Foot Deformities - bony prominences Extrinsic Factors Extrinsic Factors Environment around the foot Environment around the foot Tight shoes Tight shoes

11
Chronic Foot Ulceration Loss of Protective Function & Sensation Loss of Protective Function & Sensation Continue to Bear Weight on Ulcerated Area Continue to Bear Weight on Ulcerated Area Uninterrupted Episodes of Repetitive Stress Uninterrupted Episodes of Repetitive Stress Autolysis Autolysis Necrosis of Tissue Necrosis of Tissue

12
Sensory Loss Patient Profile Non-Compliant Non-Compliant Ignore Treatment Recommendations Ignore Treatment Recommendations Education is necessary to combat profile Education is necessary to combat profile

13
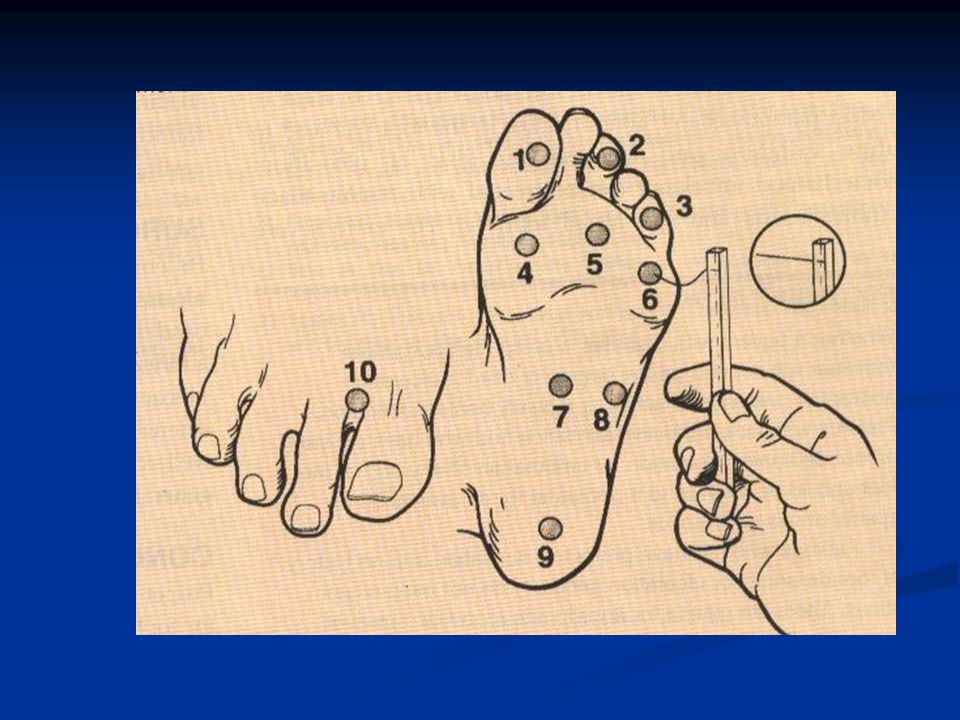
Assessment of Loss of Protective Sensation Nylon Filaments @ 10-g bending force recommended by the American Diabetes Association Nylon Filaments @ 10-g bending force recommended by the American Diabetes Association Patients unable to perceive 10-g have loss of protective sensation Patients unable to perceive 10-g have loss of protective sensation Increased risk of ulceration Increased risk of ulceration

15
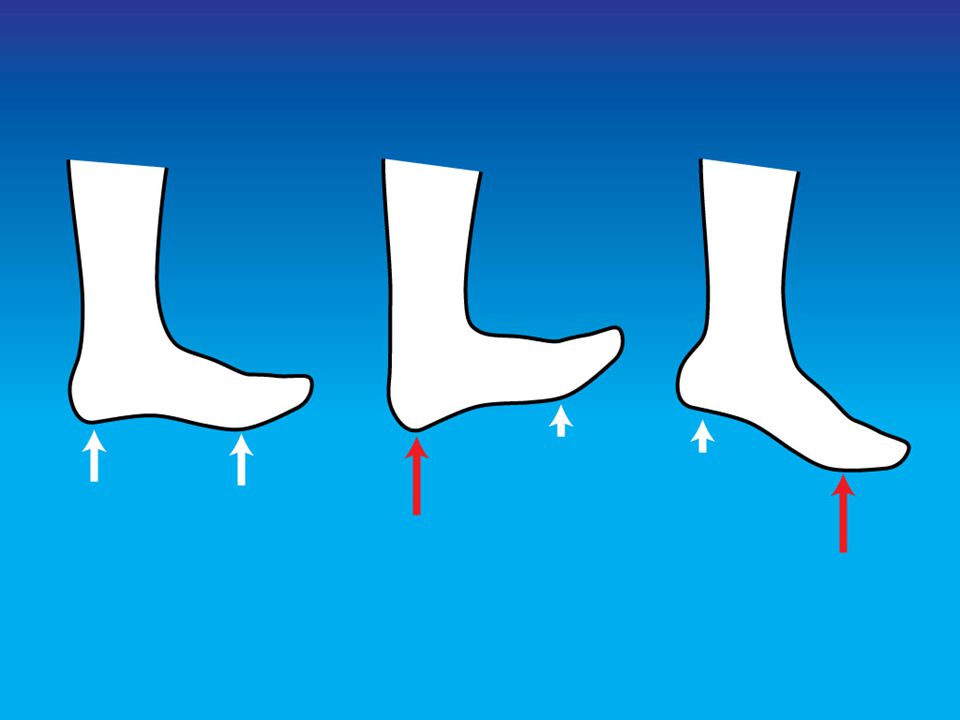
Research High pressure caused by excessive weight bearing causes plantar ulcerations High pressure caused by excessive weight bearing causes plantar ulcerations Pressure is higher in diabetic neuropathy Pressure is higher in diabetic neuropathy Higher pressure associated with foot deformity, joint limitation, muscle weakness and atrophy Higher pressure associated with foot deformity, joint limitation, muscle weakness and atrophy Muscle Weakness (toe deformities) Muscle Weakness (toe deformities) Peroneal nerve-foot drop-equinovarus-increased foot pressure-forefoot ulceration Peroneal nerve-foot drop-equinovarus-increased foot pressure-forefoot ulceration Tibial Nerve-calcaneovalgus deformity-increased heel pressure-heel ulceration Tibial Nerve-calcaneovalgus deformity-increased heel pressure-heel ulceration
 Muscle Weakness (toe deformities) Peroneal nerve-foot drop-equinovarus-increased foot pressure-forefoot ulceration Peroneal nerve-foot drop-equinovarus-increased foot pressure-forefoot ulceration Tibial Nerve-calcaneovalgus deformity-increased heel pressure-heel ulceration Tibial Nerve-calcaneovalgus deformity-increased heel pressure-heel ulceration")
16
Most Common Sites of Ulceration in Diabetics 1st Metatarsal Head 1st Metatarsal Head Great Toe Great Toe

17
Talking Points Obesity, Poor Vision, Joint Limitation (decreased flexibility) limit people from inspecting their feet Obesity, Poor Vision, Joint Limitation (decreased flexibility) limit people from inspecting their feet Mirror Mirror Properly Fitted Shoes Properly Fitted Shoes Hx of Callus, Ingrown Toenails, Blisters or Open Sores all increase risk of injury. Hx of Callus, Ingrown Toenails, Blisters or Open Sores all increase risk of injury.

18
Talking Points (cont.) Painful foot problems are often a sign of early neuropathy Painful foot problems are often a sign of early neuropathy Pain with walking or elevation indicative of PVD Pain with walking or elevation indicative of PVD Callus should be trimmed to reduce pressure & to expose an underlying problem Callus should be trimmed to reduce pressure & to expose an underlying problem
 Painful foot problems are often a sign of early neuropathy Painful foot problems are often a sign of early neuropathy Pain with walking or elevation indicative of PVD Pain with walking or elevation indicative of PVD Callus should be trimmed to reduce pressure & to expose an underlying problem Callus should be trimmed to reduce pressure & to expose an underlying problem")
19
Pre-Ulceration Local areas of non-blanchable erythema Local areas of non-blanchable erythema Ecchymosis Ecchymosis Subcutaneous hematoma Subcutaneous hematoma Neuropathic fracture Neuropathic fracture Rapidly progress to unstable foot deformity & lead to chronic ulceration Rapidly progress to unstable foot deformity & lead to chronic ulceration

20
Wagner Ulcer Classification Diabetic Ulcers Grade Grade 0Intact Skin 0Intact Skin 1Superficial Ulcer 1Superficial Ulcer 2Deep Ulcer 2Deep Ulcer 3Deep Infected Ulcer 3Deep Infected Ulcer 4Partial Foot Gangrene 4Partial Foot Gangrene 5Full Foot Gangrene 5Full Foot Gangrene

22
Management Based on Ulcer Grading Pre-ulcer: Modified Footwear & activity, PWB Pre-ulcer: Modified Footwear & activity, PWB Superficial: PWB, Relief Pads, Cast or Splint Superficial: PWB, Relief Pads, Cast or Splint Deep: PWB, Cast or Splint, Probe, X-Ray, Culture Deep: PWB, Cast or Splint, Probe, X-Ray, Culture Deep, Infected: PWB, Splint, Probe, X-ray, culture, antibiotics, surgical consult Deep, Infected: PWB, Splint, Probe, X-ray, culture, antibiotics, surgical consult Dysvascular:PWB, Splint, Vascular Studies, Vascular Consult Dysvascular:PWB, Splint, Vascular Studies, Vascular Consult * probing to bone, suspect osteomyelitis * probing to bone, suspect osteomyelitis

23
Notes on Debridement Non-Ischemic Foot Ulcers: cleaned, Debrided & Dressed Non-Ischemic Foot Ulcers: cleaned, Debrided & Dressed Wound debridement has been shown to improve healing time of non-ischemic foot ulcers Wound debridement has been shown to improve healing time of non-ischemic foot ulcers Callus should be trimmed to reduce pressure, expose underlying problems & promote epithelialization Callus should be trimmed to reduce pressure, expose underlying problems & promote epithelialization

24
Reducing Weight Bearing Stresses Objective: To reduce weight bearing stresses on the foot (plantar ulcers) Objective: To reduce weight bearing stresses on the foot (plantar ulcers) Methods Methods Crutches or Walker (PWB) Crutches or Walker (PWB) Gait Training (decrease step length to reduce forefoot pressure) Gait Training (decrease step length to reduce forefoot pressure) Walking Casts Walking Casts Decrease pressure, decrease edema, protect from re- injury Decrease pressure, decrease edema, protect from re- injury Contraindicated for infected ulcers Contraindicated for infected ulcers Caution: moderate or severe edema, fragile atrophic skin, deep ulceration Caution: moderate or severe edema, fragile atrophic skin, deep ulceration
 Objective: To reduce weight bearing stresses on the foot (plantar ulcers) Methods Methods Crutches or Walker (PWB) Crutches or Walker (PWB) Gait Training (decrease step length to reduce forefoot pressure) Gait Training (decrease step length to reduce forefoot pressure) Walking Casts Walking Casts Decrease pressure, decrease edema, protect from re- injury Decrease pressure, decrease edema, protect from re- injury Contraindicated for infected ulcers Contraindicated for infected ulcers Caution: moderate or severe edema, fragile atrophic skin, deep ulceration Caution: moderate or severe edema, fragile atrophic skin, deep ulceration")
25
Walking Casts Decrease pressure, decrease edema, protect from re-injury Decrease pressure, decrease edema, protect from re-injury Contraindicated for infected ulcers Contraindicated for infected ulcers Caution: moderate or severe edema, fragile atrophic skin, deep ulceration Caution: moderate or severe edema, fragile atrophic skin, deep ulceration

26
Total Contact Casts Minimize risk of secondary infection Minimize risk of secondary infection Bony prominences are padded Bony prominences are padded (tibial crest, malleoli, navicular, posterior heel, toes) (tibial crest, malleoli, navicular, posterior heel, toes) Inner layer of plaster, carefully molded for optimal total-contact fit Inner layer of plaster, carefully molded for optimal total-contact fit Combination of minimal padding & molding for better distribution of pressure Combination of minimal padding & molding for better distribution of pressure
 (tibial crest, malleoli, navicular, posterior heel, toes) Inner layer of plaster, carefully molded for optimal total-contact fit Inner layer of plaster, carefully molded for optimal total-contact fit Combination of minimal padding & molding for better distribution of pressure Combination of minimal padding & molding for better distribution of pressure")
27
The Use of Electrical Stimulation and an Off-Loading Technique For the Treatment of Diabetic Foot Ulcers Michael S. Brogan, PT, MS, DPT, CWS Laura E. Edsberg, Ph.D.

28
Purpose To Evaluate the efficacy of electrical stimulation and off- loading for the treatment of diabetic foot ulcers To Evaluate the efficacy of electrical stimulation and off- loading for the treatment of diabetic foot ulcers

29
Case History 52 year old male with Diabetes 52 year old male with Diabetes Insulin dependent Insulin dependent Comorbidities Comorbidities Renal failure (daily dialysis) Renal failure (daily dialysis) Severe diabetic neuropathy Severe diabetic neuropathy Left B/K amputation Left B/K amputation Left hand 3 rd & 4 th distal digit amputations Left hand 3 rd & 4 th distal digit amputations Referred for 2 chronic open wounds, Right Foot (Chronicity > 3 years) Referred for 2 chronic open wounds, Right Foot (Chronicity > 3 years) Previous Care Previous Care Various topical applications Various topical applications Various dressings Various dressings Antibiotics Antibiotics Debridement Debridement
 Renal failure (daily dialysis) Severe diabetic neuropathy Severe diabetic neuropathy Left B/K amputation Left B/K amputation Left hand 3 rd & 4 th distal digit amputations Left hand 3 rd & 4 th distal digit amputations Referred for 2 chronic open wounds, Right Foot (Chronicity > 3 years) Referred for 2 chronic open wounds, Right Foot (Chronicity > 3 years) Previous Care Previous Care Various topical applications Various topical applications Various dressings Various dressings Antibiotics Antibiotics Debridement Debridement")
30
1-6-03

32
Interventions Electrical Stimulation Electrical Stimulation High Volt Pulsed Current High Volt Pulsed Current 150v, 120pps, 255ppi 150v, 120pps, 255ppi Stainless Steel Electrodes (4x4) Stainless Steel Electrodes (4x4) 30 minutes, 5 X week 30 minutes, 5 X week Immersion Techniques Immersion Techniques Object: Object: improve blood flow improve blood flow Reduce edema Reduce edema Inhibit bacterial growth Inhibit bacterial growth Enhance closure Enhance closure
 Stainless Steel Electrodes (4x4) 30 minutes, 5 X week 30 minutes, 5 X week Immersion Techniques Immersion Techniques Object: Object: improve blood flow improve blood flow Reduce edema Reduce edema Inhibit bacterial growth Inhibit bacterial growth Enhance closure Enhance closure")
34
Off-Loading Reducing weight bearing forces on the foot is critical for healing plantar ulcers (9) Reducing weight bearing forces on the foot is critical for healing plantar ulcers (9) Total contact casts used commonly for grade 1 & 2 neuropathic foot ulcers Total contact casts used commonly for grade 1 & 2 neuropathic foot ulcers Allows weight bearing forces to be dispersed over a larger area, reducing plantar pressures Allows weight bearing forces to be dispersed over a larger area, reducing plantar pressures Rigidity of cast assists with edema control, improving circulation Rigidity of cast assists with edema control, improving circulation Cast immobilizes the foot and ankle, reducing shearing forces Cast immobilizes the foot and ankle, reducing shearing forces Completely encloses the patient’s insensate foot, protecting it from further trauma & microorganisms Completely encloses the patient’s insensate foot, protecting it from further trauma & microorganisms Allows patient to be relatively active Allows patient to be relatively active
 Reducing weight bearing forces on the foot is critical for healing plantar ulcers (9) Total contact casts used commonly for grade 1 & 2 neuropathic foot ulcers Total contact casts used commonly for grade 1 & 2 neuropathic foot ulcers Allows weight bearing forces to be dispersed over a larger area, reducing plantar pressures Allows weight bearing forces to be dispersed over a larger area, reducing plantar pressures Rigidity of cast assists with edema control, improving circulation Rigidity of cast assists with edema control, improving circulation Cast immobilizes the foot and ankle, reducing shearing forces Cast immobilizes the foot and ankle, reducing shearing forces Completely encloses the patient’s insensate foot, protecting it from further trauma & microorganisms Completely encloses the patient’s insensate foot, protecting it from further trauma & microorganisms Allows patient to be relatively active Allows patient to be relatively active")
36
TOTAL CONTACT CASTS Contraindicated Contraindicated In grades 3, 4, and 5 ulcers In grades 3, 4, and 5 ulcers Fluctuating edema Fluctuating edema Active infection Active infection ABI of less than 0.45 ABI of less than 0.45 Requires skill to apply Requires skill to apply Plaster vs. Fiberglass Plaster vs. Fiberglass Heel vs. Cast Shoe Heel vs. Cast Shoe

37
Off Loading DonJoy Walking Boot (Cam Walker) DonJoy Walking Boot (Cam Walker) provides foot and ankle immobilization at 0º, 10º, and 20º plantarflexion provides foot and ankle immobilization at 0º, 10º, and 20º plantarflexion protected range of motion in 10º increments from 40º plantarflexion to 40º dorsiflexion protected range of motion in 10º increments from 40º plantarflexion to 40º dorsiflexion easily to don and doff easily to don and doff easy to distribute weight bearing pressures via ankle motion easy to distribute weight bearing pressures via ankle motion provides protection from trauma provides protection from trauma allows for daily dressings and external treatments allows for daily dressings and external treatments can be removed when not ambulating can be removed when not ambulating
 DonJoy Walking Boot (Cam Walker) provides foot and ankle immobilization at 0º, 10º, and 20º plantarflexion provides foot and ankle immobilization at 0º, 10º, and 20º plantarflexion protected range of motion in 10º increments from 40º plantarflexion to 40º dorsiflexion protected range of motion in 10º increments from 40º plantarflexion to 40º dorsiflexion easily to don and doff easily to don and doff easy to distribute weight bearing pressures via ankle motion easy to distribute weight bearing pressures via ankle motion provides protection from trauma provides protection from trauma allows for daily dressings and external treatments allows for daily dressings and external treatments can be removed when not ambulating can be removed when not ambulating")
39
Overview of Intervention Wounds were treated 5 X week with electrical stimulation in an aqueous solution for 30 min per session Wounds were treated 5 X week with electrical stimulation in an aqueous solution for 30 min per session Wounds were first dressed with hydrogels and eventually hydrocolloids Wounds were first dressed with hydrogels and eventually hydrocolloids Walking Boot worn whenever weight bearing was anticipated (transfer & gait) Walking Boot worn whenever weight bearing was anticipated (transfer & gait)
 Walking Boot worn whenever weight bearing was anticipated (transfer & gait)")
40
Outcomes Heel 1-6-03 7-29-03

41
Outcomes Plantar Surface 1-6-03 7-29-03

42
Clinical Relevance Case study does suggest that electrical stimulation and off-Loading for diabetic neuropathic wounds is a viable treatment option Case study does suggest that electrical stimulation and off-Loading for diabetic neuropathic wounds is a viable treatment option Walking Boots that allow for ankle motion control offer an additional option for off- loading Walking Boots that allow for ankle motion control offer an additional option for off- loading Chronic diabetic foot ulcers can be treated effectively by physical therapists in conjunction with referring physicians Chronic diabetic foot ulcers can be treated effectively by physical therapists in conjunction with referring physicians Chronic wounds in patients with severe comorbidities can be healed using electrical stimulation and off-Loading Chronic wounds in patients with severe comorbidities can be healed using electrical stimulation and off-Loading

43
Tid Bits Half Casts Half Casts Ambulatory Aids, Ambulatory Aids, Molded Plastazote Sandals Molded Plastazote Sandals Post-Operative Shoes Post-Operative Shoes Pressure Relief, sculpting with Adhesive Felt Padding, Foot Orthoses, Rocker Soles Pressure Relief, sculpting with Adhesive Felt Padding, Foot Orthoses, Rocker Soles Modalities Modalities

44
Shapero, C. Stanoch, J. Barrese, D. (2002). Acute Care Perspectives: 3 (11). APTA, pp1-6.
. Acute Care Perspectives: 3 (11). APTA, pp1-6.")
45
Following Closure Proper Footwear Proper Footwear Progress into Normal Weight Bearing Gait Progress into Normal Weight Bearing Gait

Similar presentations