Download presentation
Presentation is loading. Please wait.

2
CONCUSSION “From Pitch to Podium” Dr Pierre Viviers Dr Jo-Anne Kirby Warren Adams

3
IMPORTANT PRINCIPLES Concussion must be taken extremely seriously Players suspected of having concussion: – Must be removed – Must not resume play (same match) – Must be medically assessed – Must go through a graduated RTP protocol (GRTP)
 – Must be medically assessed – Must go through a graduated RTP protocol (GRTP)")
4
AIM Refresh knowledge Share a evidence-based multi-professional approach Zurich Consensus (2008)
")
5
CONCUSSION Complex process (traumatic biochemical forces) Cause: direct/ indirect trauma to the brain Result: functional impairment (temporary) Recovery: spontaneous & often rapid (minutes > days) (challenge – window period)
 Cause: direct/ indirect trauma to the brain Result: functional impairment (temporary) Recovery: spontaneous & often rapid (minutes > days) (challenge – window period)")
6
PATHOPHYSIOLOGY Metabolic stress – “Fuel need/ fuel delivery mismatch” Need for glucose ↑ Oxidative metabolism ↓ Activation Na-K pump Intracellular Ca ↑ CBF ↓ Injury-induced vulnerability Irreversible damage

7
COMPLICATIONS Second Impact Syndrome Long Term: – 5x: mild cognitive impairment – 3x: significant memory lost – 3x: diagnosis of depression

8
Identify an injured athlete Suspect because of Mechanism – Hard hit to head – Hit to body that causes whiplash of head Behaviour of player – Stays on ground – Holds neck – Looks dazed and confused – Runs in wrong direction – Loss of consciousness ON THE PITCH

9
Stabilise the c-spine until neck pain has been excluded Remove from the field of play Remember symptoms may be subtle

10
PITCH SIDE Maddocks questions – Who is winning? – Which half of the game are we in? – Which side scored last? – Who won the previous game your team played? “When in doubt sit them out” May not return to play

11
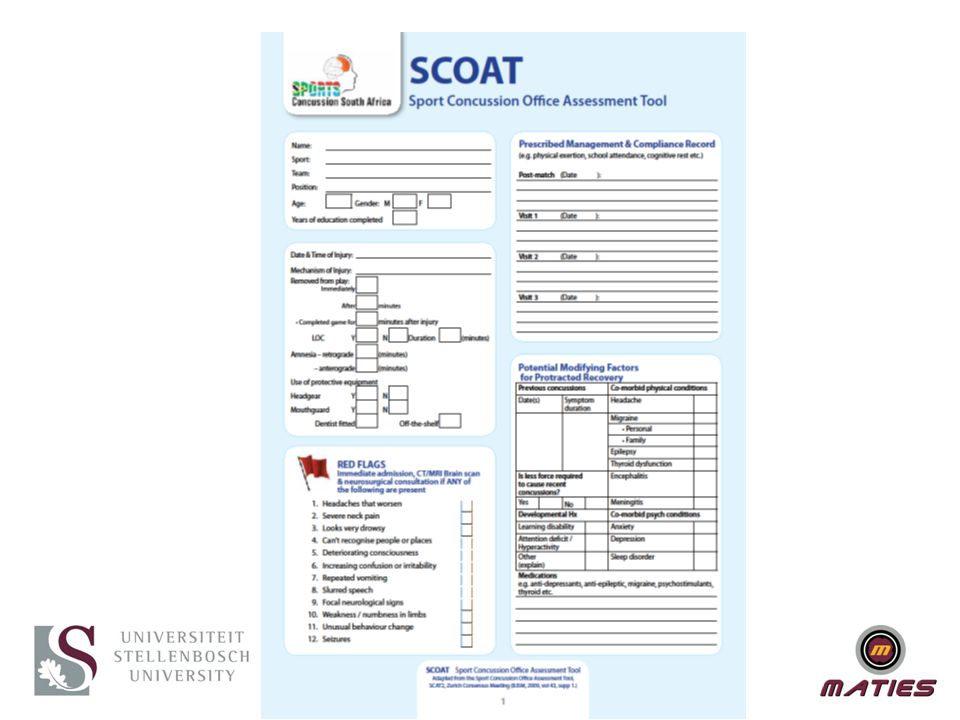
MEDICAL ASSESSMENT SCOAT Demographics of injury Red flags Identify modifying factors Symptom evaluation Cognitive assessment (Orientation) (Standardized Assessment of concussion SAC) Memory and Concentration Balance Delayed recall Upper limb coordination Physical Examination Scoring
 (Standardized Assessment of concussion SAC) Memory and Concentration Balance Delayed recall Upper limb coordination Physical Examination Scoring")
13
MANAGEMENT Cognitive Rest Physical rest Medical certificates / team notification Take home patient info Care of responsible adult Follow-up

14
FINAL CHECKLIST BEFORE RTP CAN START SCOAT score 0 (asymptomatic, normal exam) Computerized neurocognitive test returned to baseline or age-norms Exercise stress test completed asymptomatically Modifying factors considered
 Computerized neurocognitive test returned to baseline or age-norms Exercise stress test completed asymptomatically Modifying factors considered")
15
ROLE OF NEUROCOGNITIVE TESTS Example Cogsport or Impact Not a stand alone test, adjunct Assists in identifying the window period Ideal setting is pre-season baseline tests Followed by post injury monitoring until return to normal Alternate, post injury test compared to norms

17
RETURN TO PLAY FOR CONCUSSION Following a concussion or suspected concussion the management of a Graduated Return to Play(GRTP) should be undertaken on a case by case basis and with the full cooperation of the player.
 should be undertaken on a case by case basis and with the full cooperation of the player.")
18
Rehabilitation StageFunctional Exercise at Stage of rehabilitation Objective of each stage 1. No Activity, minimum 24hours following the injury where managed by a medical practitioner, otherwise minimum 14days following the injury Complete physical and cognitive rest without symptoms Recovery 2. Light aerobic exercise during 24hour period Walking, swimming or stationary cycling keeping intensity, <70% max predicted heart rate. No resistance training. Symptom free during full 24hour period. Increase heart rate 3. Sport specific exercise during 24hour period Running drills. No head impact activities. Symptom free during full 24hour period. Add Movement 4. Non Contact training drills during 24hour period Progression to more complex training drills, eg. Passing drills. May start progressive resistance training. Symptom free during full 24hour period. Exercise, coordination, and cognitive load. 5. Full contact PracticeFollowing medical clearance participate in normal training activities. Restore confidence and assess functional skills by coaching staff. 6.After 24hours return to playPlayer rehabilitatedRecovered

19
GRTP BY A MEDICAL PRACTITIONER

20
EYE HAND COORDINATION AND PERIPHERAL AWARENESS TEST – BATAK PRO

21
EYE HAND COORDINATION AND PERIPHERAL AWARENESS TEST – SVT

22
REMINDER Concussion must be taken extremely seriously Players suspected of having concussion: – Must be removed – Must not resume play (same match) – Must be medically assessed – Must go through a graduated RTP protocol (GRTP) – Assessment must be individualized – Sequential follow-up is a cornerstone
 – Must be medically assessed – Must go through a graduated RTP protocol (GRTP) – Assessment must be individualized – Sequential follow-up is a cornerstone")
23
Questions?

Similar presentations








>")












