Download presentation
Presentation is loading. Please wait.

1
Medicines Optimisation in IBD Can we base it on evidence?
Anja St.Clair Jones Lead Pharmacist Digestive Diseases Royal Sussex County Hospital Brighton

2
Enable medicines optimisation in IBD
Aims and Objectives Enable medicines optimisation in IBD Understand Inflammatory Bowel Disease (IBD), Describe drugs used in treatment of IBD Develop strategies for medicines optimisation
, Describe drugs used in treatment of IBD. Develop strategies for medicines optimisation.")
3
Stomach Duodenum Splenic flexure Hepatic flexure Transverse colon Descending colon (Left sided/distal) Ascending colon (Right sided/ proximal) Jejunum Ileum Caecum Sigmoid colon Terminal ileum Rectum Anus
 Jejunum. Ileum. Caecum. Sigmoid colon. Terminal ileum. Rectum. Anus.")
4
Epidemiology Disease of YOUNG people (peak 10-25y, 50+y)
Up to 260’000 people affected in UK UC: 10/100’000 per year prevalence 146/100’000 (NICE 2013, CG 166) Incidence stable Difference in ethnic groups (Ashkenazi Jews) 50% have relapse in any year 25% acute sever colitis during lifetime (NICE 2013) 90% are able to FT work 1year after diagnosis CD: 5-10/100’00 per year prevalence 157/100’000 (NICE 2012, CG152) Incidence increasing 75% able to work in year after diagnosis 15-20% disabled by disease within 5 years (NICE 2012) 50-80% require surgery for strictures (NICE 2012)
 Incidence stable. Difference in ethnic groups (Ashkenazi Jews) 50% have relapse in any year. 25% acute sever colitis during lifetime (NICE 2013) 90% are able to FT work 1year after diagnosis. CD: 5-10/100’00 per year. prevalence 157/100’000 (NICE 2012, CG152) Incidence increasing. 75% able to work in year after diagnosis % disabled by disease within 5 years (NICE 2012) 50-80% require surgery for strictures (NICE 2012)")
5
Anatomic distribution in Crohn’s

6
80% left sided only

7
Pathogenesis Theories of inflammatory bowel disease etiology
-Toxic response to luminal contents -Specific microbial pathogen -Abnormal luminal constituents -Increased absorption of luminal macromolecules -Enhanced immunologic response to normal constituents -Autoimmune response -To epithelial cell or mucus glycoproteins -Molecular mimicry (cross-reactivity of intestinal microflora and epithelia) -To immune cells Trigger – what? Genetic involvement
 -To immune cells. Trigger – what Genetic involvement.")
8
Immune dysregulation in Crohn's disease
Immune dysregulation in Crohn's disease Immune dysregulation in Crohn's disease. Just as epidemiologic evidence points to a balance of environmental and genetic factors in the pathogenesis of Crohn's disease, etiologic models suggest that a balance of external stimuli and internal host responses determine the hyperreactivity of the gut immune system that is seen in Crohn's disease

9
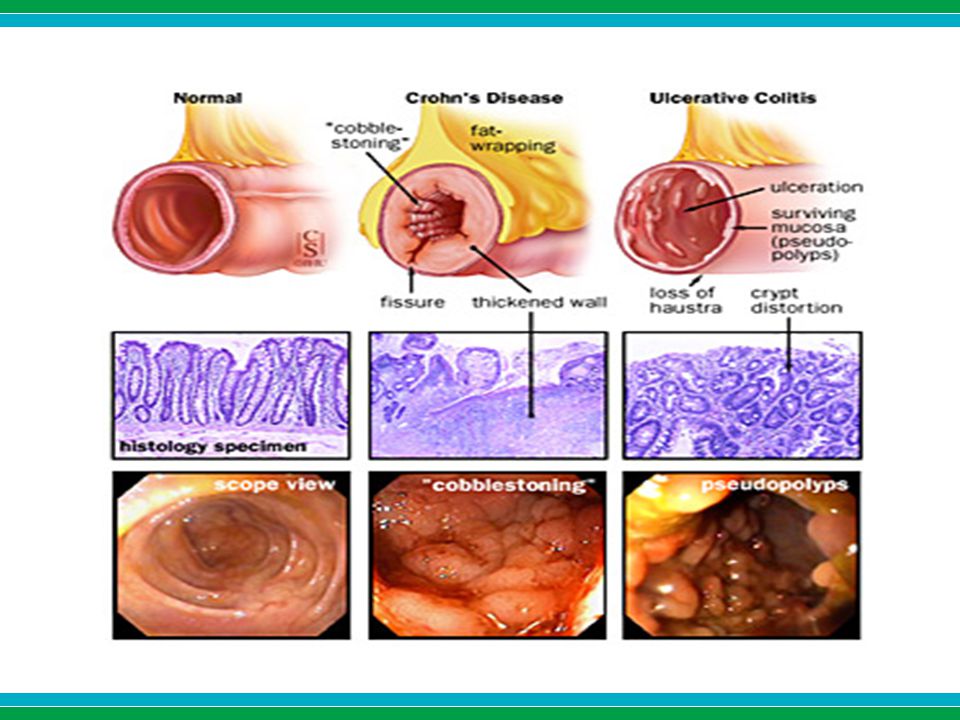
CD or UC?

10
Ulcerative colitis Crohn's disease Site of disease Colon only Any part of gastrointestinal tract Symptoms Bleeding +++ + Diarrhea ++ Abdominal pain Growth failure Tenesmus Perianal disease — Endoscopic findings Rectal involvement Inflammation Continuous Discontinuous Diffuse erythema Patchy lesions Ulceration in inflamed mucosa Discrete ulcers in normal mucosa Complications Fistulas Exceedingly uncommon Frequent (? Crohn's) Strictures Uncommon (? malignancy) Common Cancer risk (>10 years) Increased
 Strictures. Uncommon ( malignancy) Common. Cancer risk (>10 years) Increased.")
11
Fistulae in IBD

13
Diagnosis and investigations
History and examination FBC, LFT, ESR or CRP Microbiological testing (C. Diff., CMV) Abdo imaging Endoscopies +/- biopsies Barium enema, small bowel studies Colonoscopy Assessment of disease extent
 Abdo imaging. Endoscopies +/- biopsies. Barium enema, small bowel studies. Colonoscopy. Assessment of disease extent.")
15
Figure 1a and 1b: endoscopic views of Crohn’s disease showing mucosal oedema, ulceration and exudates.

17
Crohn's Disease Activity Index
CDAI = 2x1 + 5x2 + 7x3 + 20x4 + 30x5 + 10x6 + 6x7 + (weight factor)8 1. Number of liquid or very soft stools in one week 2. Sum of seven daily abdominal pain ratings: (0=none, 1=mild, 2=moderate, 3=severe) 3. Sum of seven daily ratings of general well-being: (0=well, 1=slightly below par, 2=poor, 3=very poor, 4=terrible) 4. Symptoms or findings presumed related to Crohn's disease arthritis or arthralgia iritis or uveitis erythema nodosum, pyoderma gangrenosum, apththous stomatitis anal fissure, fistula or perirectal abscess other bowel-related fistula febrile (fever) episode over 100 degrees during past week 5. Taking Lomotil or opiates for diarrhea 6. Abnormal mass 0=none; 0.4=questionable; 1=present 7. Hematocrit [ (Typical - Current) x 6 ] x [(standard weight-actual body weight) / standard weight]
8. 1. Number of liquid or very soft stools in one week. 2. Sum of seven daily abdominal pain ratings: (0=none, 1=mild, 2=moderate, 3=severe) 3. Sum of seven daily ratings of general well-being: (0=well, 1=slightly below par, 2=poor, 3=very poor, 4=terrible) 4. Symptoms or findings presumed related to Crohn s disease arthritis or arthralgia iritis or uveitis erythema nodosum, pyoderma gangrenosum, apththous stomatitis anal fissure, fistula or perirectal abscess other bowel-related fistula febrile (fever) episode over 100 degrees during past week. 5. Taking Lomotil or opiates for diarrhea. 6. Abnormal mass 0=none; 0.4=questionable; 1=present 7. Hematocrit [ (Typical - Current) x 6 ] x [(standard weight-actual body weight) / standard weight]")
18
Harvey–Bradshaw Index for Crohn's disease
Number of liquid stools per day Abdominal pain, sum of seven daily ratings: (0-none, 1-mild, 2-moderate, 3-severe) Abdominal mass (0-none, 1-questionable, 2-definite, 3-definite & tender) General well being (0-very well, 1-slightly below par, 2-poor, 3-very poor, 4-terrible) Complications (score 1 point per item) Arthritis/arthalgia Skin/mouth lesions Iritis/uveitis Anal fissure, fistula/perianal abscess
 Abdominal mass (0-none, 1-questionable, 2-definite, 3-definite & tender) General well being (0-very well, 1-slightly below par, 2-poor, 3-very poor, 4-terrible) Complications (score 1 point per item) Arthritis/arthalgia Skin/mouth lesions Iritis/uveitis Anal fissure, fistula/perianal abscess.")
20
UC activity scores

24
Therapeutic aim Remission Avoid surgery CRC (5x) Also:
Smoking cessation VTE prophylaxis (always!!) Pain control (no NSAIDs) Osteoporosis prophylaxis Opportunistic infections
 Pain control (no NSAIDs) Osteoporosis prophylaxis. Opportunistic infections.")
25
Treatments

26
How to optimise treatment?
Correct dose Co-prescribing TDM Exit strategies Rescue strategies

27
Steroids Indication: CD and UC
Moderate to severe relapse Maximise local effect and limit systemic effect No role in maintenance 40mg OD Prednisolone reduced slowly by 5mg/week ≤ 15mg ineffective in active disease Budesonide not as effective as Pred but alternative in ileo-ascending colonic disease Less systemic effect Osteoporosis

28
Rectal steroids Only for patient not responding to rectal mesalazine
Hydrocortisone (Colifoam) 1 od-bd High plasma levels after administration Prednisolone NaPhos (Predsol) 1 bd Rectal mucosa only Prednisolone metosulphbenzoate (Predenema 1 od) Poorly absorbed Increased spread (reached ascending colon in some patient) Prednisolone metosulphbenzoate (Predfoam 1od-bd) Retained in rectum and sigmoid colon
 1 od-bd. High plasma levels after administration. Prednisolone NaPhos (Predsol) 1 bd. Rectal mucosa only. Prednisolone metosulphbenzoate (Predenema 1 od) Poorly absorbed. Increased spread (reached ascending colon in some patient) Prednisolone metosulphbenzoate (Predfoam 1od-bd) Retained in rectum and sigmoid colon.")
29
Rectal steroids Rectal steroid Peak plasma nmols/L Peak tissue ng/g
Prednisolone phosphate 20mg 365 (2hrs) 44 Predenema Prednisolone meta- sulphbenzoate 20mg 45 (2hrs) 257 Predfoam 320 (4hrs) 4874 Colifoam Hydrocortisone Acetate 125mg 510(4hrs) Not recorded
 44. Predenema. Prednisolone meta- sulphbenzoate 20mg. 45 (2hrs) 257. Predfoam. 320 (4hrs) Colifoam. Hydrocortisone Acetate 125mg. 510(4hrs) Not recorded.")
30
Optimisation Correct dose Correct formulation Prevent osteoporosis
Start at 40mg and slow reduction Correct formulation Know where the disease is located Prevent osteoporosis Consider infection risk

31
Rectal reparations: site of action and indication
Formulation Site of action Disease extent Suppository Rectum Proctitis Foam Sigmoid Colon Procto-sigmoiditis Enema Descending colon to splenic flexure and in some cases even distal part of transverse colon. Left sided ( distal)colitis
colitis.")
32
5-ASA Dose: Crohn’s: UC: Rectal preparations (PINCE)
higher doses ≥ 4g no evidence (post op only) UC: Induction of remissions ≥ 4g/day Maintenance of remission ≥ 2g/day Rectal preparations (PINCE) 15% past splenic flexure:2g bd oral + 1g OD rectal (64% remission at week 8 vs 43% oral) Compliance at week 8 (PODIUM: OD vs BD:71% vs 59% remission)
 UC: Induction of remissions ≥ 4g/day. Maintenance of remission ≥ 2g/day. Rectal preparations (PINCE) 15% past splenic flexure:2g bd oral + 1g OD rectal (64% remission at week 8 vs 43% oral) Compliance at week 8. (PODIUM: OD vs BD:71% vs 59% remission)")
33
pH-dep. delayed release (>6) and matrix
Drug Formulation Optimal drug release pH Site of drug release Mesalazine Asacol MR 400mg: Enteric coated with Eudragit S 800mg: Enteric coated with layer of Eudragit S followed by Eudragit S+L pH-dep. delayed release (>7) Terminal ileum & large bowel (colon & rectum) Ipocol Enteric coated with Eudragit S >7 Terminal ileum & colon Mesren MR Octasa MR Mezavant XL Film coated with methacrylate copolymers Type A, Type B Gastroresistant coating with Lipophylic and hydrophilic matrix (>7) Colon Pentasa Ethylcellulose coated microgranules to allow slow continuous release Diffusion through semi-permeable membrane (Enteral pH) Duodenum to rectum Salofalk Tablets: Enteric coated with Eudragit L Granules: Eudragit L and matrix granule structure (slow continuous release) pH-dep. delayed release (>6) and matrix Azo-bonded preparations Salazopyrin (Sulfasalazine) Colazide (Balsalazide) Dipentum (Olsalazide) 5-ASA +SA Prodrug Dimer Cleavage by intestinal bacteria Azoreductase
 Terminal ileum & large bowel (colon & rectum) Ipocol. Enteric coated with Eudragit S. >7. Terminal ileum & colon. Mesren MR. Octasa MR. Mezavant XL. Film coated with methacrylate copolymers Type A, Type B. Gastroresistant coating with Lipophylic and hydrophilic matrix. (>7) Colon. Pentasa. Ethylcellulose coated microgranules to allow slow continuous release. Diffusion through semi-permeable membrane (Enteral pH) Duodenum to rectum. Salofalk. Tablets: Enteric coated with Eudragit L. Granules: Eudragit L and matrix granule structure (slow continuous release) pH-dep. delayed release (>6) and matrix. Azo-bonded preparations. Salazopyrin (Sulfasalazine) Colazide (Balsalazide) Dipentum (Olsalazide) 5-ASA +SA. Prodrug. Dimer. Cleavage by intestinal bacteria. Azoreductase.")
34
Adherence and switching
39% adherence in maintenance Robinson; APT 2013 61% chance of relapse vs 11% Increased risk of CRC 31% vs 3% 75% risk reduction in adherers Cost :14% admission = 49% of cost Kane 2006, Bassi 2004, Hawthorne 2008 Switch patients had 3.5-fold risk of relapse Endoscopic healing rate is not equivalent

35
Optimisation Top and tail in sever flares Consider switching carefully
Support Adherence Tailor formulation to patient Reinforce message of CRC prevention Consider switch of preparation carefully Consider impact on endoscopic healing

Similar presentations













 Kristina Blaslov Mentor: A. Žmegač Horvat.>")








 Ulcerative colitis is an inflammatory bowel disease (IBD) that causes chronic inflammation of the digestive tract It is.>")


 Idiopathic IBD is comprised of CD+UC and is characterized by chronic bowel inflammation. Idiopathic IBD is comprised of.>")