Download presentation
Presentation is loading. Please wait.

1
Clinical Decision Making in Emergency Medicine Richard Wolfe, MD Chief, Department of Emergency Medicine Harvard Medical Faculty Physicians

2
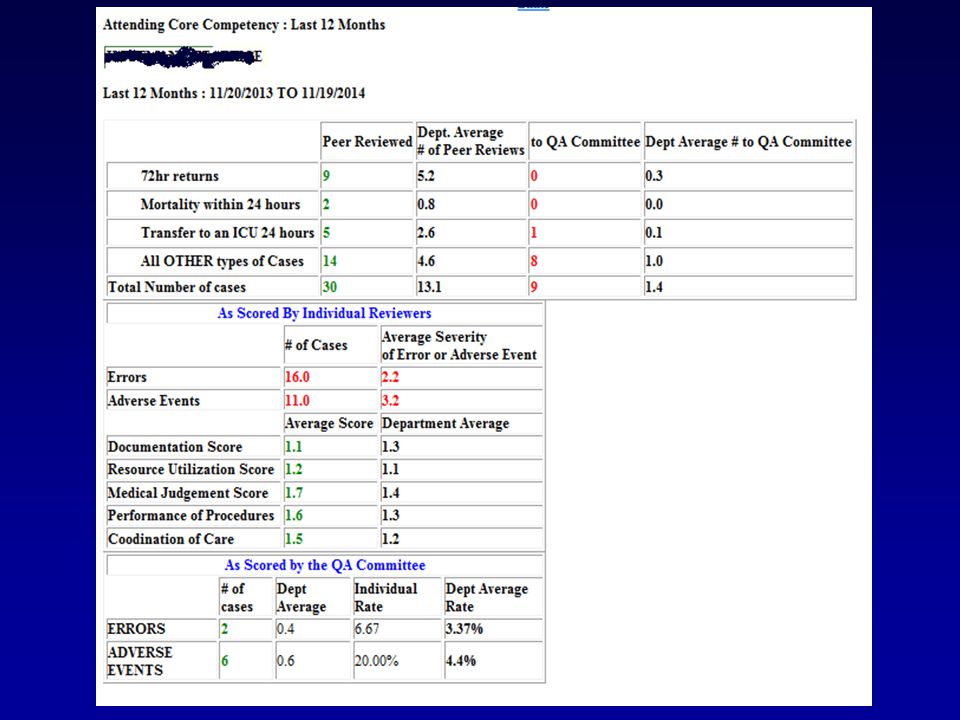
Decision Making and Clinical Errors Individual or System?

3
How do we make clinical decisions in medicine? Chief Complaints Basic Data Collection Pattern Recognition Workable Differential Diagnosis Process to prove the correct diagnosis and exclude the incorrect etiologies Management of the Working Diagnosis Disposition

4
Intuitive and Analytic Thinking

5
What is unique about Emergency Medicine? The medical decision process in the Emergency Department

6
5 Features of Emergency Medicine 1.NEED FOR SPEED 2.SPECIALIZED KNOWLEDGE 3.SHORT TERM VALUE BASED JUDGEMENTS 4.LIMITED RAPPORT WITH PATIENTS 5.COMMUNICATIONS ARE CRITICAL

7
Traditional approach in primary care Comprehensive history and physical exam Formulate comprehensive problem list Formulate long term diagnostic and therapeutic plan

8
Primary Care

9
What is the Emergency Medicine approach? Identify the chief complaints/problems Perform a focused history and physical exam Immediate recognition and empiric treatment of the potential life threats Disposition only once all life threats are identified, stabilized, or ruled out. Ensure a safe follow up plan GOALS STABILIZATION AND DISPOSITION

10
Emergency Medicine

11
How do I identify the chief complaints/problems? What brought you to the ED *now* ? What has you worried, what is new? What are others worried about? How can we help? Wait for an answer

12
What is the key question to ask a patient with a chronic complaint such as headache or abdominal pain? Is this pain different from your previous pain? If so, how is it different?

13
How do I identify life threats? Focused history based on chief complaints Focused physical exam Critical interpretation of basic labs

14
Vital signs are: The best objective data we have to identify a life threat. If they are accurately taken and critically interpreted

15
Be aware of “normal” vital signs that identify a life threat. Examples: Acute asthmatic with a respiratory rate of 12 A patient in hemorrhagic shock with a pulse of 64 Elderly patient with a BP 110/80 Respiratory Rate of 20 br/mn

17
Basic labs are: The delayed objective data we have to identify a life threat. If they are accurately ordered and critically interpreted But they can also mislead Before ordering ask: Will this test alter my management?

18
Feed Me!!

19
How do I approach the life threatened patient? Perform technical procedures and administer medication before diagnostic modalities Tube thoracostomy before chest X-ray in tension pneumothorax Antibiotics before lumbar puncture for meningitis Airway management before the crashing patient looks sick.

20
How do I formulate my differential diagnosis? What is the most serious possible cause of this patient’s presenting symptoms and signs?

21
65 year old male with sudden onset of flank pain and near syncope? Ruptured abdominal aortic aneurysm

22
57 year old male with epigastric pain, nausea and vomiting Acute inferior myocardial infarction

23
What is the most common error made in formulating a discharge diagnosis? Giving the patient a benign diagnosis that cannot be supported by the medical record. Examples: Gastroenteritis Gastritis

24
Is the diagnosis possible or necessary on all patients seen in the ED? No, and it is appropriate and ideal to state this in the assessment or diagnosis. Example: Abdominal pain of unknown etiology

25
What is the question to ask when I formulate a discharge plan? What is the most serious complication of the evolving disease process that can occur?

26
A patient with a suspected herniated disc or acute lumbar strain should be informed of: The symptoms and signs of a cauda equina syndrome

27
A patient with abdominal pain of unknown etiology should be informed of: The signs and symptoms of a surgical problem such as appendicitis.

28
What questions should I reflect upon prior to discharging a patient? Is it safe? Have I made the patient feel better? If not, did I provide an explanation as to why?

29
52 yo ♂ presents after slipping in his bathroom and falling onto a sink. He remembers striking his nose. He is complaining of nasal trauma and epistaxis. He is also complaining of epigastric pain, low back pain, and left shoulder pain. He has been seen many times for pain related complaints. PMH: Hepatitis, HIV He wants medication for the pain NOW!

30
Added information Nursing Notes Epigastric pain and left shoulder pain new following the fall. Admits to binge drinking, last drink 3 hours ago Lives alone

31
HR 110 BP 100/84 RR 20 T 37.2 Physical Exam unremarkable Smells of alcohol but clinically sober.

32
Management Nasal films normal CBC, Lipase normal Left shoulder film normal Epistaxis resolves with anterior packing Received GI Cocktail and Morphine

33
ED Course Increasingly hostile with nurses 20 patients in the waiting room Discharged with ibuprofen for pain. DC Diagnosis: Nasal Contusion, Back Strain, Gastritis Follow up with personal MD as needed

34
2 days later EMS called for man found down. Patient found at home in cardiac arrest. GEN:Pale, pupils dilated, non reactive EXT: Cool and clammy Monitor: Asystole Unable to resuscitate in Emergency Department. Post Mortem: Cause of Death: Massive Intraperitoneal Hemorrhage, Splenic rupture

35
Comments by Case Review

36
New onset abdominal pain and left shoulder pain after trauma: Obvious splenic injury. Abdominal life threat not assessed. Tachycardia not addressed? Why did he fall? Wasn’t he too intoxicated to provide an exam or be sent home? Vital signs not repeated Unsafe follow up plan Ibuprofen in patient with bleeding and possible coagulopathy Missed diagnostic studies: –INR –CT Head –FAST Ultrasound –Abdominal CT No follow up for anterior pack

37
The Amazing Retrospectoscope

38
ERROR IDENTIFICATION

41
Causes of Error in the ED Five deadly sins Ignorance: TECHNICAL ERROR Wishful thinking: JUDGEMENTAL ERROR Selfishness: NORMATIVE ERROR Distraction: SENSORY OVERLOAD Deference: RESPONSIBILITY ERROR

42
Technical Error Skills fall short of the task Ex: Did not know low mechanism could cause splenic injury Ex: Not aware of Kehr’s sign. Nasal films useless study. Other examples: Closure of a fight bite Home dispo: Fever + IVDA Adm Nec Fasc to Medicine INDECISION

43
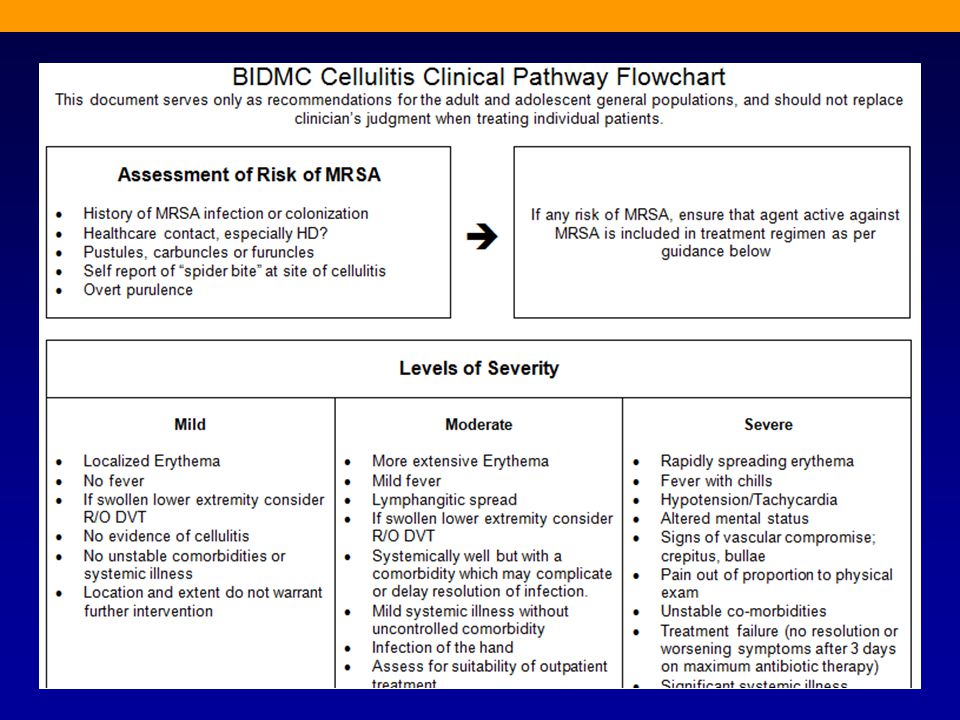
Technical Error Easy access to information Supervision Formal Educational Programs Clinical Pathways

44
Judgmental Errors Incorrect strategy is chosen Ruling out abdominal injury with physical exam only because of low mechanism Other classic examples: Not intubating a critical patient because they look good Treating wide complex tachycardia as an SVT

45
“The greatest derangement of the mind is to believe in something because one wishes it to be so.” Judgmental Error Diagnostic Anchoring Faulty Logic Brain freeze Fatigue

46
Avoiding Judgmental Errors Start with the chief complaint and take small pathophysiologic steps to catagorize the problems Explain anything that does not fit the picture Keep asking why until the answer is “I don’t care” Education in Critical Thinking

48
Normative Error Failure in the eyes of others to discharge one’s role obligations conscientiously. Ex: Undermanaging a difficult patient Ex: Less safe dispositions Other examples: –Failure to perform LP with severe headache and negative CT

49
Avoiding Normative Error Restore sense of value of the front line provider Avoid top down management M&M and intellectual honesty

50
Distraction Error Failure to incorporate all the problems into the plan Epistaxis vs. abdominal pain Boston Marathon: Near amputations vs. shrapnel Ex: Medication errors, wrong side or wrong patient, Delays in treatment

51
Distraction Error Causes: –Excessive Workload/provider –Poor information support systems –Poor communication between providers Solutions: –Work redesign: Staffing patterns, staffing roles –Information system enhancement –Team Training

52
Deference Error Misdirection by authoritative figure or Dogma

54
When all else fails, try heuristics

55
Golden Rule Patients who can’t walk, can’t leave.

56
Golden Rule Once a patient is labeled, all thinking stops. Don’t put a label on that you can’t prove.

57
Golden Rule Assume the worst case scenario and proceed to rule it out

58
Golden Rule Kill as few patients as possible

59
Questions or Comments?

Similar presentations
















>")





