Download presentation
Presentation is loading. Please wait.

1
FETAL ECHO & FETAL THERAPIES DR SANDEEP.R SR CARDIO

2
INTRODUCTION Congenital heart disease a leading cause of infant mortality – 4-13 /1000 live births Account for about 50% of all neonatal and infant deaths Prenatal detection can improve pregnancy outcomes CHD is more common in low risk pregnancies Screening tools like nuchal fold thickness,ductal venosus doppler less sensitive

3
FETAL ECHO Fetal echocardiography is broadly defined as a detailed sonographic evaluation that is used to identify and characterize fetal heart anomalies before delivery Provides information regarding: Fetal cardiac anatomy & function Fetal heart rhythm Fetal heart failure & distress The Role of Fetal Echocardiography in Fetal Intervention:A Symbiotic Relationship Clin Perinatol 36 (2009) 301–327
 301–327")
4
UNIQUE FEATURES OF FETAL CIRCULATION Presence of intracardiac & vascular passages that allow for streaming of blood( DA,DV& foramen ovale) Many critical CHD’s are well tolerated in utero ( except regurgitant lesions) Cardiac output is exclusively dependent on a narrow range of heart rate Arrhythmia’s are very poorly tolerated
 Many critical CHD’s are well tolerated in utero ( except regurgitant lesions) Cardiac output is exclusively dependent on a narrow range of heart rate Arrhythmia’s are very poorly tolerated")
5
ADVANTAGES OF FETAL ECHO – Improvement of fetal outcomes of infants with severe cardiac malformations – Helps in more specific family counselling – Timely referral of mothers with affected fetuses to tertiary cardiac care centers for neonatal management – Early diagnosis of CHD allows prompt evaluation of genetic syndromes and analysis of the fetal karyotype. – Prenatal detection of arrhythmias allows for in utero treatment – Identifies patients for in utero cardiac interventions that may be performed at certain select centers ASE GUIDELINES FOR FETAL ECHO Journal of the American Society of Echocardiography Volume 17 Number 7 2004

6
EQUIPMENT High Frames rates required All modalities of Doppler including color, pulse, high PRF, CW required Tissue Doppler imaging used in the assessment of fetal arrhythmia High frequency probes for resolution & detail Curvilinear probes more patient friendly Real time assesment required than still images ASE GUIDELINES FOR FETAL ECHO Journal of the American Society of Echocardiography Volume 17 Number 7 2004 CURVILINEAR PROBE

7
WHO SHOULD PERFORM FETAL ECHO? Physician should be – Well versed in various modalities eg.M-mode,2D, color Doppler – Able to identify simple & complex CHD – Should have knowledge of natural H/O of CHD in pregnancy – Should know limitations of fetal echo – Should have understanding of fetal arrhythmias – Aware of latest dvpnt in fetal therapy – Should have an understanding of maternal fetal physiology Appropriately trained obstetricians, maternal-fetal medicine specialists, pediatric cardiologists & radiologists with special expertise in fetal imaging ASE GUIDELINES FOR FETAL ECHO Journal of the American Society of Echocardiography Volume 17 Number 7 2004

8
TIMING OF FETAL ECHO Fetal echo possible by transvaginal approach by 9-10 weeks of gestation In the first trimester (11-14 weeks), cardiac details may not be elicited well, but the presence of a pulsatile ductus venosus or tricuspid regurgitation - a very strong marker for cardiac and chromosomal anomalies. Optimal timing - 18 - 22 weeks gestational age Image acquisition difficult after 30 weeks – Fetal rib shadowing, – Fetal position – Maternal body habitus ANITA SAXENA ET al FETAL ECHO WERE ARE WE? INDIAN JOURNAL OF PEDIATRICS July 2005

9
INDICATIONS OF FETAL ECHO MATERNAL INDICATIONSFETAL INDICATIONS Family history of CHD Metabolic disorders (eg,diabetes, PKU) Exposure to teratogens Exposure to prostaglandin synthetase inhibitors (eg, ibuprofen, salicylic acid) Rubella infection Autoimmune disease (eg,SLE, Sjogren’s) Familial inherited disorders (Ellisvan Creveld, Marfan,Noonan’s, etc) In vitro fertilization Abnormal cardiac screening examination Abnormal heart rate or rhythm Fetal chromosomal anomaly Extracardiac anomaly ( Git/spina bifida) Non immune hydrops Increased nuchal translucency >3.5mm Monochorionic twins Unexplained severe polyhydramnios ASE GUIDELINES FOR FETAL ECHO Journal of the American Society of Echocardiography Volume 17 Number 7 2004
 Exposure to teratogens Exposure to prostaglandin synthetase inhibitors (eg, ibuprofen, salicylic acid) Rubella infection Autoimmune disease (eg,SLE, Sjogren’s) Familial inherited disorders (Ellisvan Creveld, Marfan,Noonan’s, etc) In vitro fertilization Abnormal cardiac screening examination Abnormal heart rate or rhythm Fetal chromosomal anomaly Extracardiac anomaly ( Git/spina bifida) Non immune hydrops Increased nuchal translucency >3.5mm Monochorionic twins Unexplained severe polyhydramnios ASE GUIDELINES FOR FETAL ECHO Journal of the American Society of Echocardiography Volume 17 Number")
10
RECURRENCE RISK OF CHD Cardiac anomalies are known to cluster in families; the risk of having a child with a cardiac anomaly is as follows : – If a previous child was born with a CHD, the probability of a subsequent child being born with a CHD is 1:20 to 1:100 – If two previous children were born with CHD, the risk is 1:10 to 1:20 – If the mother has CHD, the risk is as high as 1:5 to 1:20 – If the father has CHD, the risk is 1:30 Indian journal of radiology imaging,Feb 2009,Vol19, issue 1

11
LIMITATIONS Operator dependent Technical limitations – Poor fetal positioning – Difficult imaging due to maternal body habitus. – Multiple fetuses may create a shadowing phenomenon Difficult to diagnose – Small VSD – Difficult to differentiate OS ASD vs flow through the foramen ovale – Anomalies of pulmonary veins – PDA Pediatr Clin N Am 56 (2009) 709–715
 709–715.")
12
FIRST TRIMESTER MARKERS OF CHD (11-14 WKS) Nuchal fold thickness > 3.5mm is associated with increased incidence of chromosomal anomalies & CHD The presence of tricuspid regurgitation (TR) determined by pulsed wave Doppler has been shown to be a marker for trisomy 21 & CHD Abnormal flow( absenceof a wave or reversal of a wave ) in the Ductus venosus doppler associated with an increased risk of chromosomal abnormalities and CHD FIRST TRIMESTER FETAL ECHOCARDIOGRAPHY. STATE OF THE PROBLEM TMJ 2009, Vol. 59, No. 2

13
FETAL POSITION J AM SOC ECHOCARDIOGRAPHY 1994;7:47-53 POSITION OF SPINE IS FIXED Transducer aligned in a sagittal plane Index marker toward maternal head Fetal lie is established (cephalic/breech, etc.) Transducer is rotated 90° counter-clockwise Left/right fetal orientation is established
 Transducer is rotated 90° counter-clockwise Left/right fetal orientation is established")
14
TRANSVERSE ABDOMINAL VIEW J AM SOC ECHOCARDIOGRAPHY 1994;7:47-53

15
SITUS Transverse view of abdomen Stomach lies on the left Aorta anterior and left of spine IVC anterior and to right of aorta IVC & aorta of same size

16
4-CHAMBER VIEW

17
POSITION OF THE HEART Cardiac position Levocardia (normal) Mesocardia Dextrocardia Cardiac malposition High incidence of CHD association Heterotaxy Syndrome (“bilateral sidedness”) May be caused by space-occupying lesions Congenital Cystic Adenomatoid Malformation (CCAM) Congenital Diaphragmatic Hernia (CDH) Congenital Lobar Emphysema Pulmonary Sequestrations Lung hypoplasia/agenesis
 Mesocardia Dextrocardia Cardiac malposition High incidence of CHD association Heterotaxy Syndrome ( bilateral sidedness ) May be caused by space-occupying lesions Congenital Cystic Adenomatoid Malformation (CCAM) Congenital Diaphragmatic Hernia (CDH) Congenital Lobar Emphysema Pulmonary Sequestrations Lung hypoplasia/agenesis")
18
4- CHAMBER VIEW - AXIS OF THE HEART NORMAL AXIS - 45 ± 20 degrees towards the left side of fetus Abnormal axis increases the risk of a cardiac malformation involving the outflow tracts Maybe associated with chromosomal anomalies Abnormal cardiac position can be caused by a diaphragmatic hernia or space-occupying lesion, such as cystic adenomatoid malformation or fetal lung hypoplasia or agenesis

19
4-C VIEW Cardiac screening examination of the fetus: guidelines for performing the ‘basic’ and ‘extended basic’ cardiac scan

20
4-C VIEW CARDIAC SIZE CARDIAC/THORACIC RATIO Normally ≤.3

21
TILT FOR OUTFLOW VIEWS

22
LVOT VIEW

23
Confirms the presence of a great vessel originating from the LV Continuity seen between the anterior aortic wall and ventricular septum Great vessel is aorta if it can be traced into its arch & with orgin of three arteries into the neck Freely moving aortic valve which is not thickened Able to identify VSD and conotruncal abnormalities

24
RVOT VIEW Documents the presence of a great vessel from a morphologic RV with a moderator band The PA normally arises from the RV and courses toward the left of the more posterior ascending aorta. It is usually slightly larger than the aortic root during fetal life and crosses the ascending aorta at about a 70 0 angle just above its origin

25
RVOT VIEW The pulmonary arterial valves move freely and should not be thickened The RVOT can be confirmed as a pulmonary artery only if its distal end appears bifurcated The distal pulmonary artery normally divides toward the left side into a ductus arteriosus that continues into the descending aorta The right side branches into the right pulmonary artery

26
3 VESSEL VIEW The left and right ventricular outflow tracts are directed almost at right angles to each other at their origin

27
3 VESSEL TRACHEAL VIEW The main features to confirm from this view are that: 1. The vessels from fetal left to right are the PA, AO & SVC with the PA being the more anterior vessel. 2. The aortic arch and pulmonary artery/ductal arch should be approximately equal in width at about 20 weeks At later gestations, the pulmonary artery tends to be a little bigger than the aorta. A marked discrepancy in size (aorta smaller than pulmonary artery) may indicate the presence of coarctation of the aorta
 may indicate the presence of coarctation of the aorta.")
28
AIUM Practice Guideline for the Performance of Fetal Echocardiography J Ultrasound Med 2013; 32: 1067–1082

29
SHORT AXIS VIEW Ventricular minor dimensions Ventricular septal integrity Papillary muscle arrangement Ventricular function

30
LONG AXIS VIEWS Sagittal view of ductal arch not visualized in pt. With conotruncal anomalies Helps in prenatal diagnosis of conotruncal anomalies Enables in diagnosis of coarctation

31
DOPPLER Spectral, CW, color, PW Doppler sonography can be used to evaluate the following structures for potential flow or rhythm abn. Pulmonary veins Foramen ovale Atrioventricular valves Atrial and ventricular septa Aortic and pulmonary valves Ductus arteriosus Aortic arch RT TO LT FLOW THROUGH PFO

32
DOPPLER UMBLICAL VESSELS PULMONARY VEIN DOPPLER VENTRICULAR INFLOW LVOT FLOW RVOT FLOW

33
SPECTRAL DOPPLER IN ARRHYTHMIA CHB ATRIAL FLUTTER 2:1 AV BLOCK SINUS TACHYCARDIA

34
M-MODE M-Mode Echocardiography (Optional) recommended for cardiac rate or rhythm abnormalities Normal fetal heart rate 120-160 BPM Heart rate > 160 beats/ Mt – tachycardia Fetal heart rate < 100/mt - bradycardia Spectral Doppler or m-mode assessment Confirm 1:1 conduction CHB
 recommended for cardiac rate or rhythm abnormalities Normal fetal heart rate BPM Heart rate > 160 beats/ Mt – tachycardia Fetal heart rate < 100/mt - bradycardia Spectral Doppler or m-mode assessment Confirm 1:1 conduction CHB")
35
CARDIAC ARRYTHMIAS

36
SVT SVT WITH SHORT VA INTERVAL SVT WITH LONG VA INTERVAL

37
FETAL ECHO ABNORMALITIES VSD ENOCARDIAL CUSHION DEFECT AORTIC STENOSIS COARCTATION OF AORTA

38
FETAL ECHO ABNORMALITIES TRUNCUS ARTERIOSUS TOF

39
FETAL THERAPIES Fetal treatment (or fetal therapy) is the “operative branch” of fetal medicine It includes a series of interventions performed on the “sick” fetus with the aim of achieving fetal well being These interventions include medical (i.e. non-invasive) and surgical procedures. Doff B. McElhinney, Wayne Tworetzky and James E. Lock Current Status of Fetal Cardiac Intervention 2010;121:1256-1263 Circulation
 and surgical procedures. Doff B. McElhinney, Wayne Tworetzky and James E. Lock Current Status of Fetal Cardiac Intervention 2010;121: Circulation.")
40
FETAL INTERVENTIONS

41
CLASSIFICATION FETAL CARDIAC INTERVENTION(FCI) Doff B. McElhinney, Wayne Tworetzky and James E. Lock Current Status of Fetal Cardiac Intervention 2010;121:1256-1263 Circulation. PHARMACOLOGICAL FCI INVASIVE FCI CLOSED FCIOPEN FCI

42
PHARMACOLOGICAL FCI FETAL TACHYARRYTHMIAS –VT/SVT/ATRIAL FLUTTER Fetal SVT – AVRT / atrial flutter most common indication for pharmacological cardiac intervention Digoxin has been a mainstay of therapy other agents used are Sotalol Amiodarone Flecainide Propranolol Modes of administeration 1)Intravenous 2)Transplacental 3)Umblical vein 4)Maternal oral administeration INDICATION FOR THERAPY 1.FETAL HYDROPS 2. SUSTAINED TACHYCARDIA 3.CARDIAC DYSFUNCTION

43
PHARMACOLOGICAL FCI FETAL BRADYCARDIA Sustained fetal bradycardia may be caused by sinus node dysfunction, long-QT syndrome, AV block, or fetal distress with acidosis The most common fetal bradyarrhythmia and the primary indication for FCI is high- grade AV block with ventricular rate < 55/mt AV BLOCK associated with 1) L-TGA 2) HETEROTAXY 3) AUTOIMMUNE DUE TO ANTI Ro/Sa Autoimmune fetal AV block can be treated with maternal administration of dexamethasone and/or sympathomimetic agents Efficacy of this combination doubtful
 L-TGA 2) HETEROTAXY 3) AUTOIMMUNE DUE TO ANTI Ro/Sa Autoimmune fetal AV block can be treated with maternal administration of dexamethasone and/or sympathomimetic agents Efficacy of this combination doubtful")
45
OTHER PHARMACOLOGICAL FCI INDICATION Fetal hydrops due to other structural cardiac anomalies Transplacental treatment with digoxin – Ebstein’s anomaly – Absent Pulmonary valve syndrome – Right heart dysfunction from left heart disease – Premature closure of the ductus arteriosus – Cardiac tumor – Cardiomyopathy Efficacy of digoxin not known

46
OPEN FETAL CARDIAC INTERVENTION “Open FCI” denotes any intervention in which the uterus is opened surgically or accessed through a surgical trochar 3 mm in diameter, which includes most fetoscopic techniques The first reported open FCI procedure in a human fetus was pacemaker placement for complete AV block

47
CLOSED FETAL CARDIAC INTERVENTION Denotes mechanical interventions in which the uterus is not opened or accessed with a port > 3 mm in diameter The first reported case of closed FCI was a balloon aortic valvuloplasty performed in 1989

48
FETAL AORTIC VALVULOPLASTY The most common closed FCI procedure Some patients with HLHS are diagnosed during the 2 nd trimester with valvar AS and a normal-sized or dilated LV evolve into HLHS over the course of gestation In other fetuses diagnosed with AS in midgestation, left heart growth and function will remain sufficient for a biventricular outcome Physiological features in favour of progression into HLHS – Retrograde flow in the transverse aortic arch – Severe LV dysfunction – Monophasic & short mitral inflow – Left to right flow through foramen ovale

49
FETAL AORTIC VALVULOPLASTY Aim of fetal aortic balloon valvuloplasty is to prevent progressive damage to the ventricular muscle and development of pulmonary vascular hypertension in utero This may allow a greater chance of surgical success postnatally

50
PROCEDURE Fetal aortic balloon valvuloplasty is performed at 21–32 weeks gestation under maternal LA and sedation, by inserting a needle through the mother’s abdominal wall into the uterine cavity under ultrasound guidance Fetal position is important for procedure success

51
The potential benefit of FCI for evolving HLHS is that decreasing LV afterload or promoting flow through the left heart may prevent evolution to HLHS 75% to 80% technical success There is solid evidence that balloon dilation of the aortic valve in fetuses with AS and evolving HLHS improves left heart physiology and leads to improved growth of the aortic and mitral valves but has no apparent effect on LV growth per se COMPLICATIONS: 1) Aortic regurgitation 2) Fetal Bradycardia & Rv Dysfunction 3) Hemopericardium 4) Fetal death 5) Premature labour
 Aortic regurgitation 2) Fetal Bradycardia & Rv Dysfunction 3) Hemopericardium 4) Fetal death 5) Premature labour")
52
FETAL ATRIAL SEPTOSTOMY INDICATIONS HLHS with restrictive ASD or intact IAS D-TGA RATIONALE A restrictive atrial communication reduces the forward flow and increases the reversed flow in the pulmonary veins at the time of atrial contraction This causes pulmonary congestion leading to chronic pulmonary hypertension This vascular damage is associated with increased 30-day mortality PREDICTORS OF ATRIAL SEPTOSTOMY Ratios of forward-to-reverse flow in the pulmonary veins Absolute velocities of reversed flow

53
FETAL ATRIAL SEPTOSTOMY CATHETER INDUCED ATRIAL SEPTOSTOMY TECHNICAL DIFFICULTIES – 1) TAMPONADE - atrial wall is thin – 2) Small balloon required as atria is small – 3) Early closure of the small puncture site HIGH-INTENSITY FOCUSED ULTRASOUND (HIFU) Newer non invasive modality Uses ultrasound frequencies ranging from 500 kHz to 10 MHz to cause localized tissue hyperthermia and damage remotely at predictable depths without injuring adjacent tissue
 TAMPONADE - atrial wall is thin – 2) Small balloon required as atria is small – 3) Early closure of the small puncture site HIGH-INTENSITY FOCUSED ULTRASOUND (HIFU) Newer non invasive modality Uses ultrasound frequencies ranging from 500 kHz to 10 MHz to cause localized tissue hyperthermia and damage remotely at predictable depths without injuring adjacent tissue")
54
FETAL PULMONARY VALVULOPLASTY PULMONARY ATRESIA WITH INTACT IVS, SEVERE PS WITH INTACT SEPTA RATIONALE Fetuses having pulmonary atresia with intact IVS show right heart hypoplasia with an overall 5-year survival of only 65% in a large population-based series There is significant morbidity, and postnatal bi-ventricular circulation can be achieved in only 32-55% Intervention offered to prevent or slow progression of ventricular hypoplasia during the 2 ND and 3 RD trimesters and to optimize right (and left) ventricular function especially when there is severe TR & fetal hydrops
 ventricular function especially when there is severe TR & fetal hydrops")
55
FETAL PULMONARY VALVULOPLASTY INDICATION Decreased biventricular cardiac output Severe pulmonary stenosis and/or elevated RV pressure (TR jet) Hydrops PROCEDURE Performed at 21–32 weeks gestation LA with USG guidancxe Fetal analgesic is then injected before advancing the needle through the fetal chest wall into the right ventricular infundibulum of the fetus A guidewire is inserted through the needle and across the pulmonary valve. A balloon catheter is inserted and then inflated to dilate the stenotic valve The catheter and needle are then withdrawn Fetal intervention for cardiac disease: The cutting edge of perinatal care.Seminars in Fetal & Neonatal Medicine (2007

56
OUTCOMES Fetal intervention for cardiac disease: The cutting edge of perinatal care.Seminars in Fetal & Neonatal Medicine (2007) 12,
 12,")
57
FETAL PACING Congenital heart block is responsible for fetal heart failure and hydrops with > 80% mortality INDICATION Fetus who is premature to be delivered and refractory to medical therapy Performed in only few cases with mixed results Fetal intervention for cardiac disease: The cutting edge of perinatal care.Seminars in Fetal & Neonatal Medicine (2007)
")
58
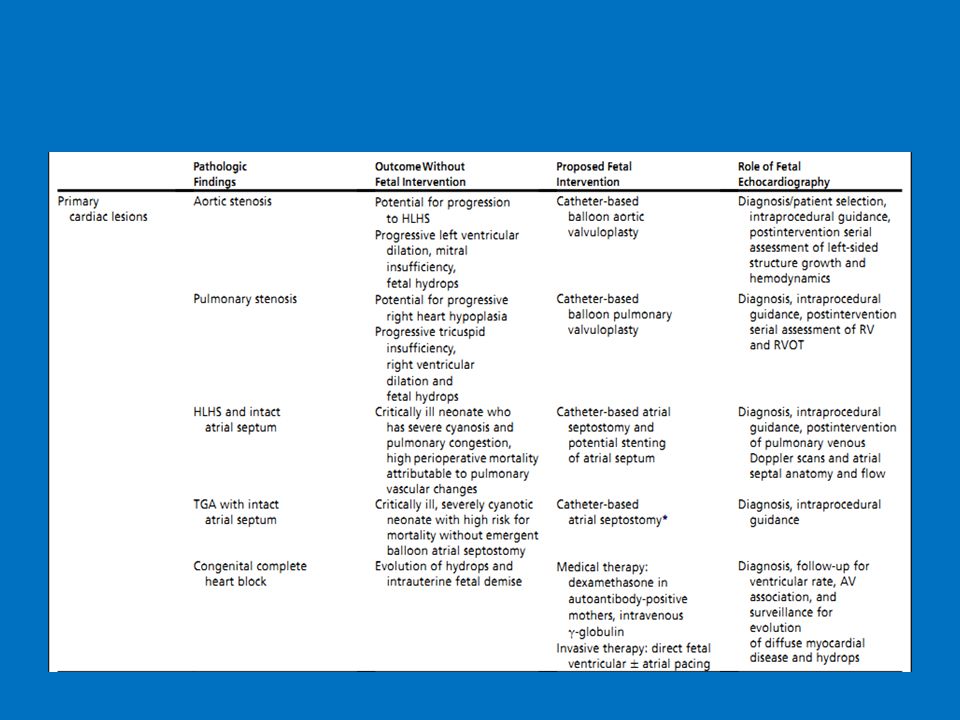
OTHER FETAL THERAPIES The Role of FetalEchocardiography in Fetal Intervention:A Symbiotic Relationship Clin Perinatol 36 (2009) 301–327
 301–327")
59
SUMMARY Comprehensive fetal echocardiography can increase detection rate of subtle CHD by up to 60%, if performed in a systematic, methodical manner Ideal time -18-22 weeks First trimester echo features like nuchal fold thickness, TR etc help in early detection Maternal and fetal indications for fetal echo Fetal therapy is a developing field with discovery of newer and effective interventions

60
THANK YOU

61
Fetal echo is ideally done during A) 12-15 weeks B) 15- 18 weeks C) 18-22 weeks D) 22-26 weeks
 weeks B) weeks C) weeks D) weeks")
62
NUCHAL FOLD THICKNESS THAT IS ASSOCIATED WITH MAXIMUM INCIDENCE OF CHD A) 1.5mm B) 2.0 mm C) 3.0 mm D) 3.5 mm
 1.5mm B) 2.0 mm C) 3.0 mm D) 3.5 mm")
63
First trimester abnormalities that can predict CHD are all except A) TR B) Foramen ovale with right to left flow C) nuchal fold thickness> 3.5 mm D) reversal of a wavein ductus venosus doppler
 TR B) Foramen ovale with right to left flow C) nuchal fold thickness> 3.5 mm D) reversal of a wavein ductus venosus doppler")
64
Fetal tachycardia is diagnosed if fetal heart rate is A)110 B)170 C) 150 D) 120
110 B)170 C) 150 D) 120")
65
Early fetal echo is done at A) 4-7 weeks B) 7-10 weeks C) 11- 14 weeks D) 14-18 weeks
 4-7 weeks B) 7-10 weeks C) weeks D) weeks")
66
Predictors of progression of valvular AS into HLHS are all except a)Retrograde flow in the transverse aortic arch b)Severe LV dysfunction c)Monophasic & short mitral inflow d)Right to left flow through foramen ovale
Retrograde flow in the transverse aortic arch b)Severe LV dysfunction c)Monophasic & short mitral inflow d)Right to left flow through foramen ovale")
67
All are true of fetal therapy in fetal tachycardia except A)AVRT is the most common SVT B)Digoxin is drug of choice C) Hydrops is an indication D) Intermittent tachycardia should be terminated
AVRT is the most common SVT B)Digoxin is drug of choice C) Hydrops is an indication D) Intermittent tachycardia should be terminated")
68
Fetal bradycardia is diagnosed if heart rate is A)110 B) 120 C)130 D)140
110 B) 120 C)130 D)140")
69
All are true except in Indication for fetal therapy in congenital AV block A) Indicated if ventricular rate is < 55/mt B) Presence of fetal hydrops C) Dexamethazone and sympathomimetic are used in autoimmune AV block D) Transcutaneous pacing is the FCI of choice in AVblock
 Indicated if ventricular rate is < 55/mt B) Presence of fetal hydrops C) Dexamethazone and sympathomimetic are used in autoimmune AV block D) Transcutaneous pacing is the FCI of choice in AVblock")
Similar presentations