Download presentation
Presentation is loading. Please wait.

1
The Map Between Lung Mechanics and Tissue Oxygenation The Map Between Lung Mechanics and Tissue Oxygenation

3
Alveolar Units Gas exchange Communication with capillary network O 2 O 2 O 2 O 2 O 2 O 2 O 2 O 2 O 2 O a a O 2 O 2 O 2 O 2 O 2 O 2 2

5
Lung Compliance and Elasticity Compliance is ability of lungs to stretch Low compliance in fibrotic lungs (and other restrictive lung diseases) and when not enough surfactant Elasticity (= Elastance) is ability to return to original shape Low Elasticity in case of emphysema due to destruction of elastic fibers. Normal lung is both compliant AND elastic

6
Pulmonary circulation Thin walled, greater internal diameters and less vascular smooth muscle than the systemic vessels. Rapidly divides into 280 billion capillaries. More distensible and compressible than the systemic system and there is less resistance to blood flow. Lower intravascular pressures Are subject to alveolar and pleural pressures. Form a sheet of blood Thin walled, greater internal diameters and less vascular smooth muscle than the systemic vessels. Rapidly divides into 280 billion capillaries. More distensible and compressible than the systemic system and there is less resistance to blood flow. Lower intravascular pressures Are subject to alveolar and pleural pressures. Form a sheet of blood

7
Gas meets blood A >a >v a >A >v a >v >A Best V/Q !!!

8
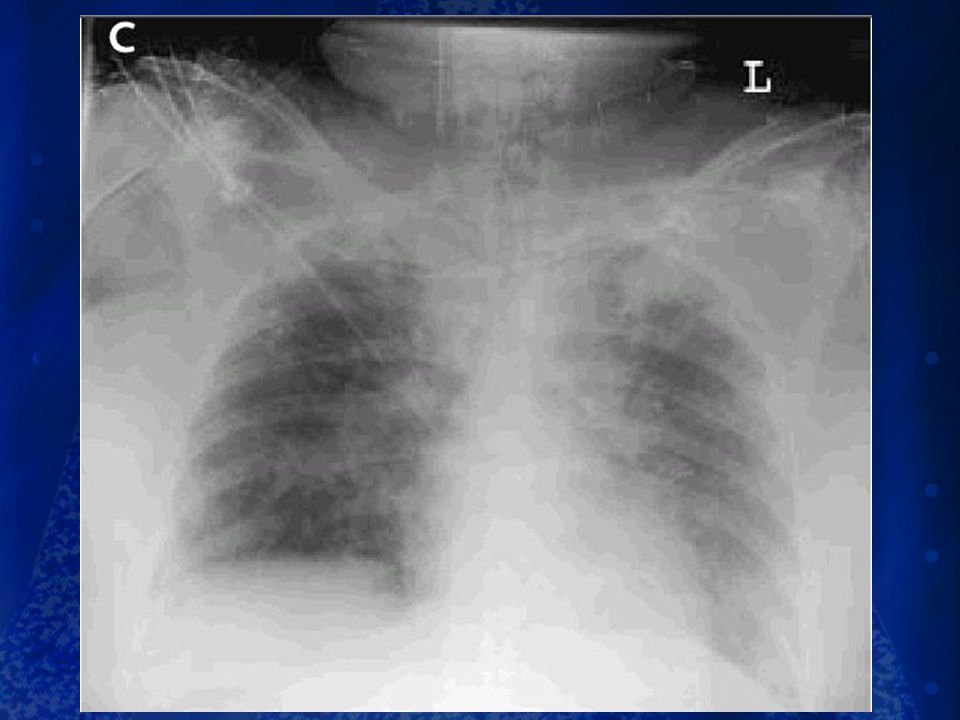
ARDS… Ware & Mattha y NEJM, 2000

9
Lung Fluid Balance = Formation and Resolution of Lung Edema in ALI/ARDS

10
Gas meets blood A >a >v a >A >v a >v >A Best V/Q !!!

12
Gas meets blood A >a >v a >A >v a >v >A Best V/Q !!!

13
V/Q inequality Increases A-a PO 2 (norm. 5-20 mmHg) Reduces PaO 2 – V/Q more blood than gas venous admixture – V/Q more gas than blood venous admixture Q flows only through unaffected regions, thus it relatively there Increases A-a PO 2 (norm. 5-20 mmHg) Reduces PaO 2 – V/Q more blood than gas venous admixture – V/Q more gas than blood venous admixture Q flows only through unaffected regions, thus it relatively there
 Reduces PaO 2 – V/Q more blood than gas venous admixture – V/Q more gas than blood venous admixture Q flows only through unaffected regions, thus it relatively there Increases A-a PO 2 (norm mmHg) Reduces PaO 2 – V/Q more blood than gas venous admixture – V/Q more gas than blood venous admixture Q flows only through unaffected regions, thus it relatively there.")
14
Pulmonary Measures P/F ratio = Pa02/ Fi02 100/ 0.21= 470 P/F ratio = Pa02/ Fi02 100/ 0.21= 470

15
Which is BEST P/F ratio –1. 90 on 1.0 –2. 60 on 0.50 –3. 70 on 0.21 P/F ratio –1. 90 on 1.0 –2. 60 on 0.50 –3. 70 on 0.21

16
What can I do about it?

17
Blood flow increase towards lung bases Zone 3: –resistance decrease due to distension related to volume weight and gravity (dependence: water glass) –Pa and Pv are higher than PA What does this have to do with my patient? Zone 3: –resistance decrease due to distension related to volume weight and gravity (dependence: water glass) –Pa and Pv are higher than PA What does this have to do with my patient?
 –Pa and Pv are higher than PA What does this have to do with my patient .")
18
Lung Fluid Balance = Formation and Resolution of Lung Edema in ALI/ARDS

19
When you ventilate only with…..

21
Simple Ventilation terms Fraction of Inspired Oxygen (FIO2) –Amount or percent of oxygen mixed into the atmospheric pressurized gas Optimal < 40% Any patient on > 50% for more than two days is very sick and at risk for long vent stays Pressure –A means of measuring and/or controlling the effects of the volume delivery to the lung Peak pressures > 50 cm H20 indicate stiff sick lungs and risk for long vent stays Mean pressures or Plateau pressures > 35 cm H20 may indicate respiratory distress syndrome and very long vent stays Pressure control ventilation may also indicate respiratory distress syndrome and very long vent stays Fraction of Inspired Oxygen (FIO2) –Amount or percent of oxygen mixed into the atmospheric pressurized gas Optimal < 40% Any patient on > 50% for more than two days is very sick and at risk for long vent stays Pressure –A means of measuring and/or controlling the effects of the volume delivery to the lung Peak pressures > 50 cm H20 indicate stiff sick lungs and risk for long vent stays Mean pressures or Plateau pressures > 35 cm H20 may indicate respiratory distress syndrome and very long vent stays Pressure control ventilation may also indicate respiratory distress syndrome and very long vent stays
 –Amount or percent of oxygen mixed into the atmospheric pressurized gas Optimal < 40% Any patient on > 50% for more than two days is very sick and at risk for long vent stays Pressure –A means of measuring and/or controlling the effects of the volume delivery to the lung Peak pressures > 50 cm H20 indicate stiff sick lungs and risk for long vent stays Mean pressures or Plateau pressures > 35 cm H20 may indicate respiratory distress syndrome and very long vent stays Pressure control ventilation may also indicate respiratory distress syndrome and very long vent stays Fraction of Inspired Oxygen (FIO2) –Amount or percent of oxygen mixed into the atmospheric pressurized gas Optimal < 40% Any patient on > 50% for more than two days is very sick and at risk for long vent stays Pressure –A means of measuring and/or controlling the effects of the volume delivery to the lung Peak pressures > 50 cm H20 indicate stiff sick lungs and risk for long vent stays Mean pressures or Plateau pressures > 35 cm H20 may indicate respiratory distress syndrome and very long vent stays Pressure control ventilation may also indicate respiratory distress syndrome and very long vent stays")
22
Simple Ventilation Terms Minute ventilation (V E or MV): –the amount of volume exhaled per minute (V E ) or measured as RR × V T (MV) –Normal 8-10 liters/minute Peak Inspiratory Pressure (PIP) –peak pressure measured when the tidal volume is pushed into the airways –value used to set high and low pressure alarm limits Minute ventilation (V E or MV): –the amount of volume exhaled per minute (V E ) or measured as RR × V T (MV) –Normal 8-10 liters/minute Peak Inspiratory Pressure (PIP) –peak pressure measured when the tidal volume is pushed into the airways –value used to set high and low pressure alarm limits
: –the amount of volume exhaled per minute (V E ) or measured as RR × V T (MV) –Normal 8-10 liters/minute Peak Inspiratory Pressure (PIP) –peak pressure measured when the tidal volume is pushed into the airways –value used to set high and low pressure alarm limits Minute ventilation (V E or MV): –the amount of volume exhaled per minute (V E ) or measured as RR × V T (MV) –Normal 8-10 liters/minute Peak Inspiratory Pressure (PIP) –peak pressure measured when the tidal volume is pushed into the airways –value used to set high and low pressure alarm limits")
23
Simple Ventilation Terms Flow rate: The rate of speed of volume delivery –impacts I:E ratio –slow flow: I time, E time –fast flow: I time, E time Flow rate: The rate of speed of volume delivery –impacts I:E ratio –slow flow: I time, E time –fast flow: I time, E time

24
SIMPLE METHODS Ventilatory Modes –CMV, IMV, SIMV, A/C, PCV Adjuncts to Mechanical Ventilation –PEEP, CPAP, PSV Ventilatory Modes –CMV, IMV, SIMV, A/C, PCV Adjuncts to Mechanical Ventilation –PEEP, CPAP, PSV

25
Simple Ventilation Modes and Adjuncts When anticipation is that the patient will not require lengthy support > 3-5 days, simple modes are generally applied: Modes –Controlled Mandatory or assist control ventilation: CMV or ACMV –Intermittent Mandatory Ventilation: IMV –Synchronized Intermittent Mandatory Ventilation: SIMV When anticipation is that the patient will not require lengthy support > 3-5 days, simple modes are generally applied: Modes –Controlled Mandatory or assist control ventilation: CMV or ACMV –Intermittent Mandatory Ventilation: IMV –Synchronized Intermittent Mandatory Ventilation: SIMV

26
Volume vs… Pressure Control Ventilation Volume Ventilation Volume delivery constant Inspiratory pressure varies Inspiratory flow constant Inspiratory time determined by set flow and V T Volume Ventilation Volume delivery constant Inspiratory pressure varies Inspiratory flow constant Inspiratory time determined by set flow and V T Pressure Ventilation Volume delivery varies Inspiratory pressure constant Inspiratory flow varies Inspiratory time set by clinician

27
Lung Compliance and Elasticity Compliance is ability of lungs to stretch Low compliance in fibrotic lungs (and other restrictive lung diseases) and when not enough surfactant Elasticity (= Elastance) is ability to return to original shape Low Elasticity in case of emphysema due to destruction of elastic fibers. Normal lung is both compliant AND elastic

28
Pressure time PIP: compliance resistance volume flow PEEP

29
PIP Pplat resistance flow compliance tidal volume No active breathing Treats lung as single unit end-inspiratory alveolar pressure

30
What else can I look at??

31
0 20 40 60 -20 -40 -60 0.2 0.4 0.6 LITERS P aw cmH 2 O VTVT Pressure-Volume Loop Changes

32
Indicates a drop in compliance (higher pressure for the same volume) 0 20 40 60 20 40 -60 0.2 0.4 0.6 LITERS P aw cmH 2 O VTVT Changes in Compliances
 LITERS P aw cmH 2 O VTVT Changes in Compliances")
33
B A 0 20 40 60 -20 -40 -60 0.2 0.4 0.6 LITERS P aw cmH 2 O C A = inspiratory pressure B = upper inflection point C = lower inflection point VTVT Overdistension

35
Respiratory rate Max RR at 35 breaths/min Efficiency of ventilation decreases with increasing RR Decreased time for alveolar emptying T V Goal of 10 ml/kg Risk of volutrauma Other means to decrease P a CO 2 Reduce muscular activity/seizures Minimizing exogenous carb load Controlling hypermetabolic states Permissive hypercapnea Preferable to dangerously high RR and T V, as long as pH > 7.15 RR and T V are adjusted to maintain V E and P a CO 2 I:E ratio (IRV) Increasing inspiration time will increase T V, but may lead to auto- PEEP PIP Elevated PIP suggests need for switch from volume-cycled to pressure-cycled mode Maintained at <45cm H 2 O to minimize barotrauma Plateau pressures Pressure measured at the end of inspiratory phase Maintained at <30-35cm H 2 O to minimize barotrauma Vent settings to improve ventilation
 Increasing inspiration time will increase T V, but may lead to auto- PEEP PIP Elevated PIP suggests need for switch from volume-cycled to pressure-cycled mode Maintained at <45cm H 2 O to minimize barotrauma Plateau pressures Pressure measured at the end of inspiratory phase Maintained at <30-35cm H 2 O to minimize barotrauma Vent settings to improve ventilation")
36
PEEP Increases FRC Prevents progressive atelectasis and intrapulmonary shunting Prevents repetitive opening/closing (injury) Recruits collapsed alveoli and improves V/Q matching Resolves intrapulmonary shunting Improves compliance Enables maintenance of adequate P a O 2 at a safe FiO 2 level Disadvantages Increases intrathoracic pressure (may require pulmonary a. catheter) May lead to ARDS Rupture: PTX, pulmonary edema PEEP and FiO 2 are adjusted in tandem Oxygen delivery (DO 2 ), not PaO 2, should be used to assess optimal PEEP. Vent settings to improve oxygenation
 May lead to ARDS Rupture: PTX, pulmonary edema PEEP and FiO 2 are adjusted in tandem Oxygen delivery (DO 2 ), not PaO 2, should be used to assess optimal PEEP. Vent settings to improve oxygenation.")
37
Pressure Limited –FiO 2 –Rate –I-time –PEEP – PIP Pressure Limited –FiO 2 –Rate –I-time –PEEP – PIP Volume Limited –FiO 2 –Rate – Tidal Volume –PEEP –I time MV MAP Dealers Choice

38
ARDSnet NIH NHLBI ARDS Clinical Trials Network

39
Downloaded from www.ardsnet.org

40
APRV

41
HFOV

42
Effects of PPV on Afterload RV afterload (overall: increased) –increased: Starling resistor phenomenon –decreased: RV compression, pulmonary vasodilation due to increased lung volume LV afterload: decreased due to LV and thoracic aorta compression RV afterload (overall: increased) –increased: Starling resistor phenomenon –decreased: RV compression, pulmonary vasodilation due to increased lung volume LV afterload: decreased due to LV and thoracic aorta compression
 –increased: Starling resistor phenomenon –decreased: RV compression, pulmonary vasodilation due to increased lung volume LV afterload: decreased due to LV and thoracic aorta compression RV afterload (overall: increased) –increased: Starling resistor phenomenon –decreased: RV compression, pulmonary vasodilation due to increased lung volume LV afterload: decreased due to LV and thoracic aorta compression")
43
Pulsus Paradoxus

47
Summary What we can do? –hold to a standard of care –define and report appropriately –communicate scientifically –evaluate in the presence and the absence of invasive monitoring What we can do? –hold to a standard of care –define and report appropriately –communicate scientifically –evaluate in the presence and the absence of invasive monitoring

48
Summary Discuss, defend, discuss turn turn turn oygenate? ventilate? flow that blood Discuss, defend, discuss turn turn turn oygenate? ventilate? flow that blood

Similar presentations