Download presentation
Presentation is loading. Please wait.

1
Ventilation and mechanics
Lecture -2 Ventilation and mechanics

2
Objectives Define airway resistance (RAW) and lung compliance (CL) and discuss the components of each and factors affecting them. Discuss the mechanics and measurement of surface tension. Discuss the role of pulmonary surfactant in the optimal functioning of the respiratory system . Explain the “work of breathing” and discuss the effects of resistance, compliance and surface tension on it .

3
Pulmonary ventilation & gas exchange
Explain the relevance of the Gas Laws in respiratory physiology List the normal fractional concentrations and partial pressures (at sea level) for the main constituents of air . Calculate the partial pressures of gases in atmospheric & alveolar air Define & quantitate alveolar ventilation (VA), physiologic dead space and anatomic dead space (VD). Explain the concept of the ventilation/perfusion ratio . Discuss the regional differences in normal alveolar ventilation and pulmonary blood flow. Describe the various laboratory methods used to assess ventilatory function . Relate abnormal ventilation/perfusion ratios to PaO2 and PaCO2 values .
 for the main constituents of air . Calculate the partial pressures of gases in atmospheric & alveolar air. Define & quantitate alveolar ventilation (VA), physiologic dead space and anatomic dead space (VD). Explain the concept of the ventilation/perfusion ratio . Discuss the regional differences in normal alveolar ventilation and pulmonary blood flow. Describe the various laboratory methods used to assess ventilatory function . Relate abnormal ventilation/perfusion ratios to PaO2 and PaCO2 values .")
4
Self study Describe what happens when pulmonary ventilation is either too much or too little. Describe the physiological significance of the residual volume and RV/TLC ratio . Explain flow-volume curves with special reference to the effort-dependent and effort-independent regions and their change with disease states . Distinguish between obstructive and restrictive lung diseases. Explain the concept of dynamic compression of airways . Explain the measurement and significance of “closing volume” . Define diffusion capacity (transfer factor) and discuss its measurement and factors affecting it . Discuss the various types of hypoxia. Explain the significance of an elevated alveolar to arterial PO2 difference . Explain the physiological bases for hypoxaemia .
 and discuss its measurement and factors affecting it . Discuss the various types of hypoxia. Explain the significance of an elevated alveolar to arterial PO2 difference . Explain the physiological bases for hypoxaemia .")
5
Ventilation by bulk flow
F = Δ P/R Flow is proportional to pressure difference between atmosphere Patm and alveoli Palv & inversely proportional to the resistance R. F= (Patm - Palv )/R All pressures in the RS are given relative to atmospheric pressure (760mm Hg) So zero alveolar pressure= same as atmospheric. Change in dimensions of lung bring change in alveolar pressure.
/R. All pressures in the RS are given relative to atmospheric pressure (760mm Hg) So zero alveolar pressure= same as atmospheric. Change in dimensions of lung bring change in alveolar pressure.")
6
Black lines show lung’s position at beginning of insp or exp & blue lines at end.

9
Pneumothorax Surgery/trauma-chest wall pierced without damaging lung.
Atmospheric air rushes into interpleural space & interpleural pressure goes from -4 mmHg to 0 mmHg. The transpulmonary pressure acting to hold lungs open is thus eliminated and lungs collapses & the chest wall moves outward since its elastic recoil is no longer opposed.

10
Summary of changes in pressures and volumes

11
Inspiration

12
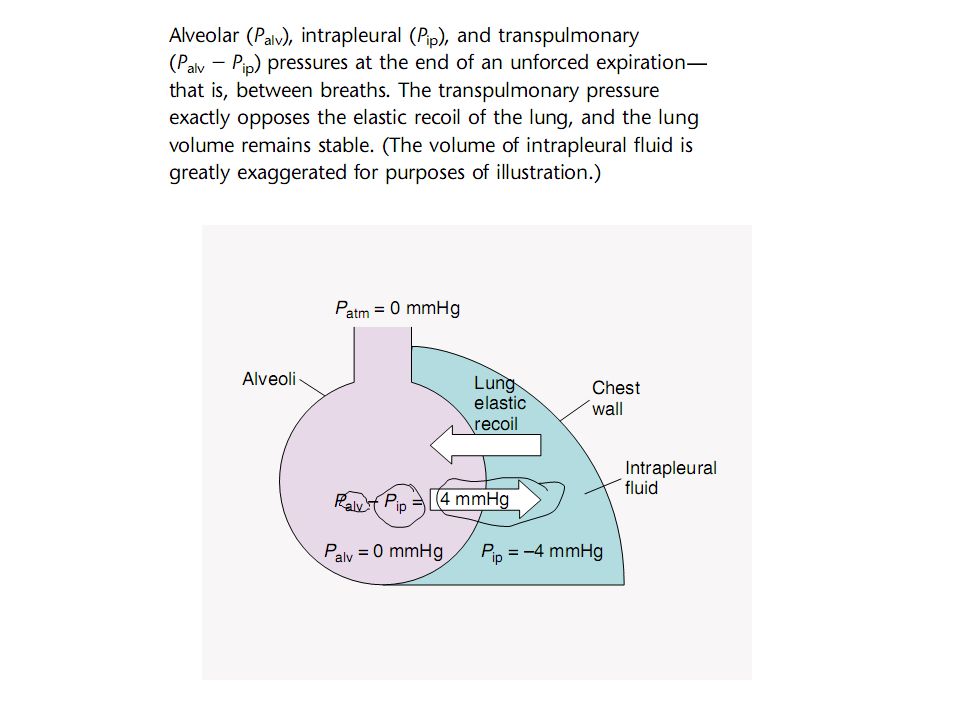
In between the breaths Palv- Pip= 0- (-4)=4mmHg Patm-Pip=0-(-4)=4mmHg
The transpulmonary pressure exactly opposes the elastic recoil of lung-lung volume remains stable.

13
The alveolar pressure is the sum of the pleural pressure Ppl and the elastic recoil pressure Pel.

14
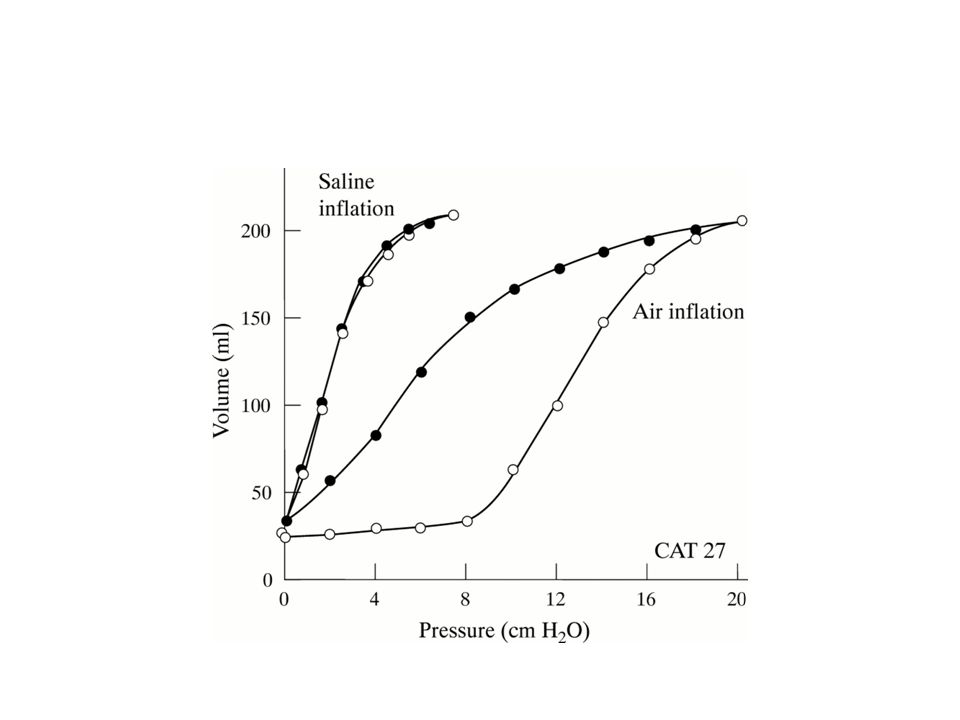
A pressure–volume curve developed from measurements in isolated lung during inflation (inspiration) and deflation (expiration). The slope of each curve is the compliance. The difference in the curves is hysteresis.

16
Determinants of compliance- strechability and surfactant

17
Deflation pressure volume curve (PV).
Because of hysteresis caused by surfactant, the deflation PV curve is used for measurements. Compliance at any point along this curve is the change in volume per change in pressure. From the curve it can be seen that lung compliance varies with lung volume. Compare compliance at 1 vs. 2. By convention, lung compliance is the change in pressure in going from FRC to FRC + 1 L.

18
Note: Deflation curve is curvilinear.
in upper 1/3 of slope line is not very steep- indicating low compliance. Lower portion slope is steep-denoting high compliance. CONCLUSION: Lungs can be easily distended when transpulmonary pressure is low. Benefit: Normally we breath at pressure & volume representing lower 70% of curve- when lungs are more compliant-less work of breathing –economy of ATP coinage. CL = Δ VL Δ PL

19
Fibrosis/emphysema pressure/volume curve.
Normal &asthma-same EXCEPT that asthma has higher FRC. Emphysema-High TLC & FRC but at a lower translung pressure because lungs easily inflate. Fibrosis-stiffness of lungs & ↓ TLC and FRC

20
Compliance changes

21
Relationship between compliance and lung volume
Relationship between compliance and lung volume. Imagine a lung in which a 5 cm H2O change in pressure results in a 1 L change in volume. If half of the lung is removed, the compliance will decrease but when corrected for the volume of the lung there is no change (specific compliance). Even when the lung is reduced by 90%, the specific compliance is unchanged.
. Even when the lung is reduced by 90%, the specific compliance is unchanged.")
22
Determinants of compliance-strechability and surface tension

24
Passive pressure volume curve of chest wall compared to lung- near the TLC lung stiffness, limits the thoracic expansion & near RV chest wall stiffness limits the collapse of lungs

26
Dynamic compliance

27
Dynamic compliance is < static compliance

28
Importance of sigh/yawning-exposure of more surfactant molecules to the surface

29
Airways resistance as a function of the airway generation
Airways resistance as a function of the airway generation. In the normal lung, most of the resistance to airflow occurs in the first eight airway generations

30
Chest radiograph showing left pneumothorax with shift of the mediastinum and trachea to the right side (white arrows). The left lung is not completely collapsed. Pic 2: Chest radiograph showing relief of tension after insertion of a chest tube (white arrow). Left lung is re-expanded, and position of mediastinum and trachea is now central.
. Left lung is re-expanded, and position of mediastinum and trachea is now central..")
31
The relaxation pressure-volume curve of the lung, chest wall, and respiratory system. The curve for the respiratory system is the sum of the individual curves. The curve for the lung is the same.

Similar presentations














 2. Airways resistance work30% 3. Moving tissues 5% Normally >")






