Download presentation
Presentation is loading. Please wait.

1
Nancy Pares, RN, MSN Metro Community College

2
Apply basic knowledge of healthy maternal newborn care (recall from PN year) Describe ethical and legal issues of maternal newborn nursing, current legislation and community resources available. Demonstrate appropriate therapeutic communication and assessment of high risk pregnancy.

3
Context ◦ Who is involved, what is the setting ◦ What other information is needed ◦ What personal beliefs of the nurse may impact the situation Clarification of the issues ◦ What are the ethical issues ◦ Who should decide the issue Identification of alternatives and potential outcomes

4
Ethical reasoning ◦ What ethical theories have bearing on the situation ◦ Should some theories be given greater weight in the decision making process ◦ What legal or social constraints are factors ◦ What obligations might be present in the role of the nurse

5
Resolution ◦ What is the best action in this situation ◦ What strategy should be used to carry out this action Evaluation ◦ What were the outcomes ◦ Should this same action be used in the future for similar dilemmas

6
Professional Nurse Certified Registered Nurse Nurse Practitioner Clinical Nurse Specialist Certified Nurse Midwife

7
Religion and social beliefs Presence and influence of the extended family Socialization within the ethnic group Communication patterns Beliefs and understanding about health and illness Permissible physical contact with strangers education

8
Standards of care: ◦ Minimum criteria for competent, proficient, delivery of nursing care Institutional policies Ethical implications Scope of practice ◦ Defined by state Nurse Practice Act laws

9
There was a duty to provide care. The duty was breached. Injury occurred. The breach of duty caused the injury (proximate cause).
..")
10
Divergence between rights of mother and rights of fetus: ◦ Mother may refuse fetal intervention. ◦ Fetal intervention may be forced on mother. Fetal research: ◦ Therapeutic vs. non-therapeutic

11
Intrauterine fetal surgery: ◦ Therapy for anomalies incompatible with life ◦ Health of the mother and fetus is at risk ◦ Surrogate, frozen embryo, ◦ Female circumcision

12
Abortion ◦ Can be performed until point of viability ◦ After viability, if mother’s health in jeopardy Nursing role ◦ Have right to refuse to assist ◦ Responsible for ensuring a qualified replacement is available

13
Infertility Human stem cells Cord blood Maternal refusal for c/del Maternal refusal for fetal surgery

14
Womens’ health standards by Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN) State Boards Individual facilities policy
 State Boards Individual facilities policy")
15
A holistic interpersonal approach Adequate documentation Communication Updated and realistic policies and procedures Appropriate delegation Question deviations from the standar Follow chain of command

16
Transforms research findings into clinical practice: ◦ Efficiency improvement ◦ Better outcomes ◦ Quality improvement

17
Identify vulnerable periods during which malformations of various organs may occur and describe the resulting anomalies. Describe the function and structure of the placenta during intrauterine life. (review PN year)
.")
18
Mitosis: ◦ Exact copies of original cell Meiosis: ◦ Production of new organism

19
Deletion ◦ Loss of chromosome material Translocation ◦ Misplacement Nondisjunction ◦ Chromosomes don’t separate correctly Karotype ◦ Chromosomal make up of an individual Mosaicism two or more genetically different cell populations in an individual

21
Interphase Prophase Metaphase Anaphase Telophase

22
First division: ◦ Chromosomes replicate, pair, and exchange information. ◦ Chromosome pairs separate, and cell divides. Second division: ◦ Chromatids separate and move to opposite poles. ◦ Cells divide, forming four daughter cells.

23
Ovary gives rise to oogonial cells. Cells develop into oocytes. Meiosis begins and stops before birth. Cell division resumes at puberty. Development of Graafian follicle.

24
Production of sperm First meiotic division: ◦ Primary spermatocyte replicates and divides. Second meiotic division: ◦ Secondary spermatocytes replicate and divide. Produce four spermatids.

26
Uniting sperm and ovum form a zygote Ova are fertile for 12 to 24 hours Sperm are fertile for 72 hours Takes place in the ampulla of fallopian tube

27
Capacitation: ◦ Removal of plasma membrane and glycoprotein coat ◦ Loss of seminal plasma proteins Acrosomal reaction: ◦ Release of enzymes ◦ Allows entry through corona radiata

29
Zone pellucida blocks additional sperm from entering Secondary oocyte completes second meiotic division ◦ Forms nucleus of ovum Nuclei of ovum and sperm unite Membranes disappear Chromosomes pair up

30
Fraternal: two ova and two sperm Identical: single fertilized ovum - Originate at different stages

31
Cleavage Blastomeres form morula Blastocyst: - develops into embryonic disc and amnion Trophoblast: - develops into chorion

32
Occurs 7 to 10 days after fertilization Blastocyst burrows into endometrium Endometrium is now called decidua

33
Primary germ layers: ◦ Ectoderm ◦ Mesoderm ◦ Endoderm

34
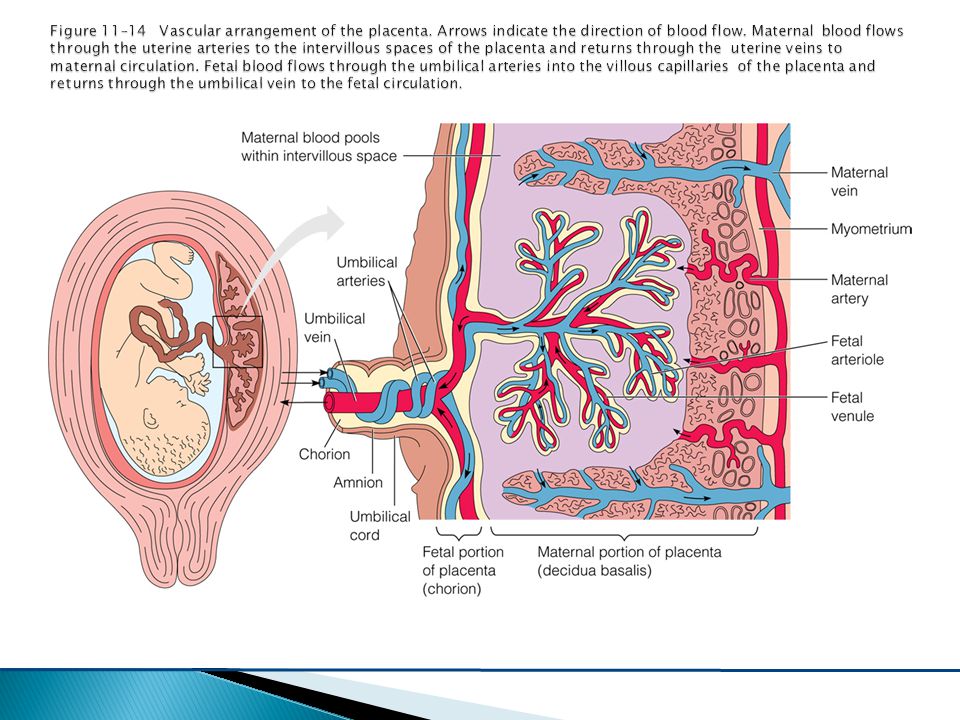
Metabolic and nutrient exchange Maternal portion: ◦ Decidua Fetal portion: ◦ Chorionic villi Fetal surface covered by amnion

35
Chorionic villi form spaces in decidua basalis Spaces fill with maternal blood. Chorionic villi differentiate: ◦ Syncytium: outer layer ◦ Cytotrophoblast: inner layer Anchoring villi form septa

37
Body stalk fuses with embryonic portion of the placenta Provides circulatory pathway from chorionic villi to embryo: ◦ One vein Delivers oxygenated blood to fetus: ◦ Two arteries

39
Nutrition Excretion Fetal respiration Production of fetal nutrients Production of hormones

40
Beginning development of GI tract Heart is developing Somites develop—beginning vertebrae Heart is beating and circulating blood Eyes and nose begin to form Arm and leg buds are present

41
Trachea is developed Liver produces blood cells Trunk is straighter Digits develop Tail begins to recede

42
Eyelids are closed Tooth buds appear Fetal heart tones can be heard Genitals are well-differentiated Urine is produced Spontaneous movement occurs

43
Lanugo begins to develop Blood vessels are clearly developed Active movements are present Fetus makes sucking motions Swallows amniotic fluid Produces meconium

44
Subcutaneous brown fat appears Quickening is felt by mother Nipples appear over mammary glands Fetal heartbeat is heard by fetoscope

45
Eyes are structurally complete Vernix caseosa covers skin Alveoli are beginning to form

46
Testes begin to descend Lungs are structurally mature

47
Rhythmic breathing movements Ability to partially control temperature Bones are fully developed but soft and flexible

48
Increase in subcutaneous fat Lanugo begins to disappear

49
Skin appears polished Lanugo has disappeared except in upper arms and shoulders Hair is now coarse and approximately 1 inch in length Fetus is flexed

50
Quality of sperm or ovum Genetic code Adequacy of intrauterine environment Teratogens

51
Maternal effects: ◦ Malnutrition ◦ Bone-marrow suppression ◦ Increased incidence of infections ◦ Liver disease Neonatal effects: ◦ Fetal alcohol spectrum disorders (FASD)
")
53
Seizures and hallucinations Pulmonary edema Respiratory failure Cardiac problems Spontaneous first trimester abortion, abruptio placentae, intrauterine growth restriction (IUGR), preterm birth, and stillbirth
, preterm birth, and stillbirth")
54
Decreased birth weight and head circumference Feeding difficulties Neonatal effects from breast milk: ◦ Extreme irritability ◦ Vomiting and diarrhea ◦ Dilated pupils and apnea

55
Maternal effects: ◦ Poor nutrition and iron-deficiency anemia ◦ Preeclampsia-eclampsia ◦ Breech position ◦ Abnormal placental implantation ◦ Abruptio placentae ◦ Preterm labor

56
Maternal effects: ◦ Premature rupture of the membranes (PROM) ◦ Meconium staining ◦ Higher incidence of STIs and HIV Fetal effects: ◦ IUGR ◦ Withdrawal symptoms after birth
 ◦ Meconium staining ◦ Higher incidence of STIs and HIV Fetal effects: ◦ IUGR ◦ Withdrawal symptoms after birth")
57
Marijuana: difficult to evaluate, no known teratogenic effects PCP - maternal overdose or a psychotic response MDMA (Ecstasy) - long-term impaired memory and learning
 - long-term impaired memory and learning")
59
Identify tests used to detect abnormalities, fetal well being and infertility management. Discuss age related considerations of pregnancy. Explain the nursing process as it relates to maternal fetal medical conditions.

60
Favorable cervical mucus Clear passage between cervix and tubes Patent tubes with normal motility Ovulation and release of ova

61
No obstruction between ovary and tubes Endometrial preparation Adequate reproductive hormones

62
Normal semen analysis Unobstructed genital tract Normal genital tract secretions Ejaculated spermatozoa deposited at the cervix

63
Ovulation Cervix Uterine structures Tubal patency Semen analysis

65
Ovulatory: ◦ Pharmacologic treatment ◦ Donor oocytes Cervical: ◦ THI, IVF, GIFT

66
Uterine/Tubal: ◦ IVF, GIFT ◦ Donor oocytes or gestational carrier Sperm: ◦ THI, IVF, GIFT ◦ Micromanipulation

68
Marriage may be stressed Relationship affected by intrusiveness Guilt Frustration Anger Shame

69
Loss of control Feelings of reduced competency and defectiveness Loss of status and ambiguity as a couple A sense of social stigma Stress on the personal and sexual relationship A strained relationship with healthcare providers

70
Counselor Educator Advocate

71
Maternal age 35 or over Family history: ◦ Known or suspected Mendelian genetic disorder ◦ Birth defects and/or mental retardation

72
Previous pregnancies: ◦ Previous child with chromosomal anomaly ◦ Previous child with metabolic disorder ◦ Two or more first trimester spontaneous abortions

73
Parental genetics: ◦ Couples with a balanced translocation ◦ Couples who are carriers for a metabolic disorder Abnormal MSAFP Women with teratogenic risk

74
Multigenerational 50% chance of passing on the gene Males and females equally affected Varying degrees of presentation Diseases ◦ Achondroplasia ◦ Marfans ◦ Neurofibromotosis

75
Achondroplasia ◦ Most common dwarfism, lifespan and IQ WNL Marfans ◦ Connective tissue disorder, triad of ocular, skeletal and CV alterations Neurofibromotosis (Von Recklinhausen) ◦ Soft tumor development of peripheral nerves
 ◦ Soft tumor development of peripheral nerves")
77
Carrier parents 25% chance of passing on abnormal gene 25% chance of an affected child If child is clinically normal, 50% chance child is carrier Males and females equally affected Diseases: CF, Sickle Cell, PKU, Tay Sachs

79
No male-to-male transmission 50% chance carrier mother will pass the abnormal gene to sons (affected) 50% chance carrier mother will pass the abnormal gene to daughters (carrier) Diseases: Hemophilia A, Duchennes MD, Trisomies, Klinefelters, Turner’s Cri du chat, Fragile X
 50% chance carrier mother will pass the abnormal gene to daughters (carrier) Diseases: Hemophilia A, Duchennes MD, Trisomies, Klinefelters, Turner’s Cri du chat, Fragile X")
81
Genetic ultrasound Genetic amniocentesis Chorionic villus sampling Percutaneous umbilical blood sampling MSAFP

83
Educate about tests Provide support Refer for counseling Resource during and after counseling

84
Identify the maternal fetal effects of TORCH (toxoplasmosis, other, rubella, cytomegalovirus, herpes) infections and the corresponding nursing interventions.
 infections and the corresponding nursing interventions.")
85
Toxoplasmosis Rubella Cytomegalovirus Herpes simplex virus Group B streptococcus Human B-19 parvovirus

86
Retinochoroiditis Convulsions Coma Microcephaly Hydrocephalus

87
Congenital cataracts Sensorineural deafness Congenital heart defects

88
Neurologic complications Anemia Hyperbilirubinemia Thrombocytopenia Hepatosplenomegaly SGA

89
Preterm labor Intrauterine growth restriction Neonatal infection

90
Respiratory distress or pneumonia Apnea Shock Meningitis Long-term neurologic complications

91
Spontaneous abortion Fetal hydrops Stillbirth

92
Discuss pathophysiology, treatment and nursing interventions for pregnant women with: ◦ Cardiac Disease, Chorioamnionitis, Gestational trophoblastic disease, diabetes, Rh sensitivity, pregnancy induced hypertension and HELLP syndrome, HIV, hyperemesis gravidarium.

93
Endocrine disorder of carbohydrate metabolism Results from inadequate production or utilization of insulin Cellular and extracellular dehydration Breakdown of fats and proteins for energy

94
Carbohydrate intolerance of variable severity Causes: ◦ An unidentified preexistent disease ◦ The effect of pregnancy on a compensated metabolic abnormality ◦ A consequence of altered metabolism from changing hormonal levels

95
Early pregnancy: ◦ Increased insulin production and tissue sensitivity Second half of pregnancy: ◦ Increased peripheral resistance to insulin

96
Hydramnios Preeclampsia-eclampsia Ketoacidosis Dystocia Increased susceptibility to infections

97
Perinatal mortality Congenital anomalies Macrosomia IUGR RDS Polycythemia

98
Hyperbilirubinemia Hypocalcemia

99
Assess risk at first visit: ◦ Low risk - screen at 24 to 28 weeks ◦ High risk - screen as early as feasible

100
Age over 40 Family history of diabetes in a first-degree relative Prior macrosomic, malformed, or stillborn infant Obesity Hypertension Glucosuria

101
One-hour glucose tolerance test: ◦ Level greater than 130-140 mg/dl requires further testing 3-hour glucose tolerance test: ◦ GDM diagnosed if 2 levels are exceeded

102
Maintain a physiologic equilibrium of insulin availability and glucose utilization Ensure an optimally healthy mother and newborn Treatment: ◦ Diet therapy and exercise ◦ Glucose monitoring ◦ Insulin therapy

103
AFP Fetal activity monitoring NST Biophysical profile Ultrasound

104
Assessment of glucose Nutrition counseling Education about the disease process and management Education about glucose monitoring and insulin administration Assessment of the fetus Support

105
Maternal complications: ◦ Susceptible to infection ◦ May tire easily ◦ Increased chance of preeclampsia and postpartal hemorrhage ◦ Tolerates poorly even minimal blood loss during birth

106
Fetal complications: ◦ Low birth weight ◦ Prematurity ◦ Stillbirth ◦ Neonatal death

107
Prevention and treatment: ◦ Prevention - at least 27 mg of iron daily ◦ Treatment - 60-120 mg of iron daily

108
Maternal complications: ◦ Nausea, vomiting, and anorexia Fetal complications: ◦ Neural tube defects Prevention - 4 mg folic acid daily Treatment - 1 mg folic acid daily plus iron supplements

109
Maternal complications: ◦ Vaso-occlusive crisis ◦ Infections ◦ Congestive heart failure ◦ Renal failure

110
Fetal complications include fetal death, prematurity, and IUGR. Treatment: ◦ Folic acid ◦ Prompt treatment of infections ◦ Prompt treatment of vaso-occlusive crisis

111
Treatment: ◦ Folic acid ◦ Transfusion ◦ Chelation

112
Asymptomatic women - pregnancy has no effect Symptomatic with low CD4 count - pregnancy accelerates the disease Zidovudine (ZDV) therapy diminishes risk of transmission to fetus Transmitted through breast milk Half of all neonatal infections occurs during labor and birth
 therapy diminishes risk of transmission to fetus Transmitted through breast milk Half of all neonatal infections occurs during labor and birth")
113
Intrapartal or postpartal hemorrhage Postpartal infection Poor wound healing Infections of the genitourinary tract

114
Infants will often have a positive antibody titer Infected infants are usually asymptomatic but are likely to be: ◦ Premature ◦ Low birth weight ◦ Small for gestational age (SGA)
")
115
Counsel about implications of diagnosis on pregnancy: ◦ Antiretroviral therapy ◦ Fetal testing ◦ Cesarean birth

116
Congenital heart disease Marfan syndrome Peripartum cardiomyopathy Eisenmenger syndrome Mitral valve prolapse

117
Rheumatoid arthritis Epilepsy Hepatitis B Hyperthyroidism Hypothyroidism Maternal phenylketonuria

118
Multiple sclerosis Systemic lupus erythematosus Tuberculosis

119
Tubal damage Previous pelvic or tubal surgery Endometriosis Previous ectopic pregnancy Presence of an IUD High levels of progesterone

120
Congenital anomalies of the tube Use of ovulation-inducing drugs Primary infertility Smoking Advanced maternal age

121
Methotrexate Surgery

123
Assess the appearance and amount of vaginal bleeding Monitors vital signs Assess the woman’s emotional status and coping abilities Evaluate the couple’s informational needs. Provide post-operative care

124
Vaginal bleeding Anemia Passing of hydropic vesicles Uterine enlargement greater than expected for gestational age Absence of fetal heart sounds Elevated hCG

125
Low levels of MSAFP Hyperemesis gravidarum Preeclampsia

126
D&C Possible hysterectomy Careful follow-up

128
Monitor vital signs Monitor vaginal bleeding Assess abdominal pain Assess the woman’s emotional state and coping ability

129
Control vomiting Correct dehydration Restore electrolyte balance Maintain adequate nutrition

130
Assess the amount and character of further emesis Assess intake and output and weight. Assess fetal heart rate Assess maternal vital signs Observe for evidence of jaundice or bleeding Assess the woman’s emotional state

131
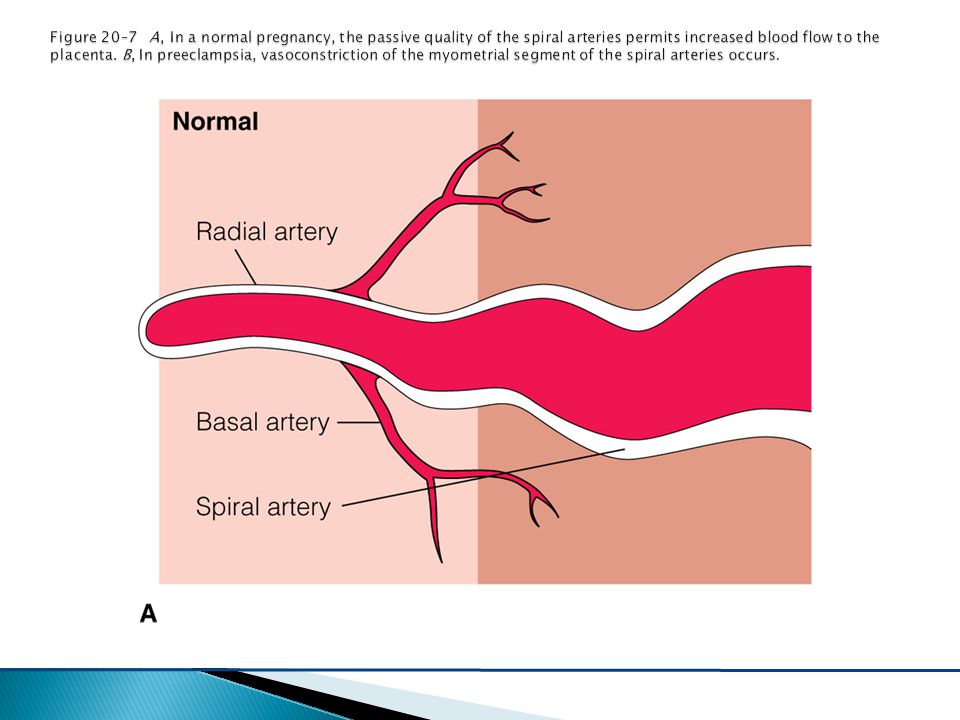
Preeclampsia-eclampsia Chronic hypertension Chronic hypertension with superimposed preeclampsia Gestational hypertension

132
Maternal vasospasm Decreased perfusion to virtually all organs Decrease in plasma volume Activation of the coagulation cascade Alterations in glomerular capillary endothelium Edema

133
Increased viscosity of the blood Hyperreflexia Headache Subcapsular hematoma of the liver

136
Small for gestational age Fetal hypoxia Death related to abruption Prematurity

137
Monitoring for signs and symptoms of worsening condition Fetal movement counts Frequent rest in the left lateral position Monitoring of blood pressure, weight, and urine protein daily NST Laboratory testing

138
Bed rest High-protein, moderate-sodium diet Treatment with magnesium sulfate Corticosteroids Fluid and electrolyte replacement Antihypertensive therapy

139
Scotomata Blurred vision Epigastric pain Vomiting Persistent or severe headache Neurologic hyperactivity

140
Pulmonary edema Cyanosis

141
Assess characteristics of seizure Assess status of the fetus Assess for signs of placental abruption Maintain airway and oxygenation Position on side to avoid aspiration Suction to keep the airway clear

142
To prevent injury, raise padded side rails Administer magnesium sulfate

143
Hemolysis, elevated liver enzymes, low platelets ◦ Hypertension and proteinuria may or may not be present ◦ 90% present with symptoms before 36 wks gest. ◦ All with HELLP should deliver

144
Rh – mother, Rh + fetus Maternal IgG antibodies produced Hemolysis of fetal red blood cells Rapid production of erythroblasts Hyperbilirubinemia

146
After birth of an Rh+ infant After spontaneous or induced abortion After ectopic pregnancy After invasive procedures during pregnancy After maternal trauma

147
Mom is type O Infant is type A or B Maternal serum antibodies are present in serum Hemolysis of fetal red blood cells

148
Incidence of spontaneous abortion is increased in first trimester Insert nasogastric tube prior to surgery Insert indwelling catheter Encourage patient to use support stockings Assess fetal heart tones Position to maximize utero-placental circulation

149
Greater volume of blood loss before signs of shock More susceptible to hypoxemia with apnea Increased risk of thrombosis DIC Traumatic separation of placenta Premature labor

150
Psychological distress Loss of pregnancy Preterm labor Low-birth-weight infants Fetal death Increased risk of STIs

Similar presentations
























>")













