Download presentation
Presentation is loading. Please wait.

1
Hemorrhage, Hemostasis and Circulatory Shock

2
Hemorrhage Extravasation of blood due to ruptured vessels From hemo = blood, rrhagia = to burst forth Hemorrhage may be external or internal Hemorrhage may be obvious (gross) or hidden (occult) This is whole blood with RBCs, not just edemic transudates or exudates
 or hidden (occult) This is whole blood with RBCs, not just edemic transudates or exudates")
3
How much blood loss? Class I: up to 15% of blood volume typically no change in vital signs routine blood donation amounts to ~10% Class I: 15-30% of total blood volume tachycardia (rapid heart beat) with a narrowing of the difference between the systolic and diastolic blood pressures compensatory peripheral vasoconstriction; cool, pale skin; altered mental status, dizzy or confused fluid resuscitation with saline or Lactated Ringer's solution Class III: 30-40% of circulating blood volume blood pressure drops, heart rate increases, peripheral perfusion worsens, mental status worsens fluid resuscitation and/or blood transfusion Class IV: >40% of circulating blood volume hypovolemic shock--limit of the body's compensation is reached aggressive resuscitation is required to prevent death
 with a narrowing of the difference between the systolic and diastolic blood pressures compensatory peripheral vasoconstriction; cool, pale skin; altered mental status, dizzy or confused fluid resuscitation with saline or Lactated Ringer s solution Class III: 30-40% of circulating blood volume blood pressure drops, heart rate increases, peripheral perfusion worsens, mental status worsens fluid resuscitation and/or blood transfusion Class IV: >40% of circulating blood volume hypovolemic shock--limit of the body s compensation is reached aggressive resuscitation is required to prevent death.")
4
Indications of internal hemorrhage Deep Anemia—fewer circulating RBCs Increased indirect bilirubin (unconjugated, albumin-bound) Surface Hemorrhage under the skin or mucous membranes looks red (oxygenated Hb) or purple (deoxygenated Hb)
 Surface Hemorrhage under the skin or mucous membranes looks red (oxygenated Hb) or purple (deoxygenated Hb)")
5
Enclosed bleeding by size and shape Petechiae are flat, tiny, 1- to 2-mm, multifocal locally increased intravascular pressure, coagulation (platelet) defects, the trauma of sudden hypoxia (strangulation) from Italian, petecchie = flea bites (puh-teek-ee-uh) petechia (s.); petechiae (pl.); petechial (adj) Purpura are flat, small, ≥1 mm, multifocal Term used to describe platelet-related bleeding disorders that result in bruised skin and/or mucous membranes from Latin, purple Ecchymoses, contusions (bruises) are smooth and noticeably large, >1 cm, focal trauma, vascular inflammation chymose = juicy Hematoma are emergent, lumpy, hardened, focal Clotted blood collected near the skin surface or internally at serosal surfaces or aneurysms
 defects, the trauma of sudden hypoxia (strangulation) from Italian, petecchie = flea bites (puh-teek-ee-uh) petechia (s.); petechiae (pl.); petechial (adj) Purpura are flat, small, ≥1 mm, multifocal Term used to describe platelet-related bleeding disorders that result in bruised skin and/or mucous membranes from Latin, purple Ecchymoses, contusions (bruises) are smooth and noticeably large, >1 cm, focal trauma, vascular inflammation chymose = juicy Hematoma are emergent, lumpy, hardened, focal Clotted blood collected near the skin surface or internally at serosal surfaces or aneurysms")
6
Colors of bruising Initial hemorrhage of RBCs into tissue is cleared by macrophages, which process Hb Oxyhemoglobin and Deoxyhemoglobin Deoxyhemoglobin and Biliverdin Biliverdin and Bilirubin Bilirubin and Hemosiderin Hemosiderin When iron and porphyrins are completely cleared, tissue resumes normal color

7
Distribution of hemorrhage(s) Multifocal indicates problem affecting vessels or platelets thrombocytopenia or thrombocytopathy reduced number or function of platelets preventing coagulation inherited coagulation defects—hemorrhagic diathesis anticoagulants inhibit production of vitamin K-dependent coagulation proteins end stage hepatic disease. With approximately 80% loss of functional hepatic tissue, production of coagulation factors can become inadequate. disseminated intravascular coagulation (DIC) coagulation out of control vasculitis immune mediated--precipitation of Ag-Ab complexes, which are chemotactic for neutrophils, resulting in vascular damage infections of endothelium Focal distribution single or a few focal hemorrhages are typical of trauma regional neoplasm, thrombosis, or microbial invasion problems with protein clotting factors
 coagulation out of control vasculitis immune mediated--precipitation of Ag-Ab complexes, which are chemotactic for neutrophils, resulting in vascular damage infections of endothelium Focal distribution single or a few focal hemorrhages are typical of trauma regional neoplasm, thrombosis, or microbial invasion problems with protein clotting factors.")
8
Petechiae from strangulation

9
Petechiae

11
Petechiae or purpurae

12
Senile or actinic purpura

13
Echymoses or contusions

14
Hematoma--subdural

15
Hematoma

16
Subcapsular hematoma

17
Hemopericardium This is hemopericardium as demonstrated by the dark blood in the pericardial sac opened at autopsy. Penetrating trauma or massive blunt force trauma to the chest (often from the steering wheel) causes a rupture of the myocardium and/or coronary arteries with bleeding into the pericardial cavity. The extensive collection of blood in this closed space leads to cardiac tamponade. A pericardiocentesis, with needle inserted into the pericardial cavity, can be a diagnostic procedure.
 causes a rupture of the myocardium and/or coronary arteries with bleeding into the pericardial cavity. The extensive collection of blood in this closed space leads to cardiac tamponade. A pericardiocentesis, with needle inserted into the pericardial cavity, can be a diagnostic procedure..")
18
Gastrointestinal hemorrhage When rate is slow, blood is digested or lost in feces In upper GI, blood turns black and tarry as it is digested and is called melena Melena is symptomatic of peptic ulcers, ruptured esophageal varices, cancers In lower GI, blood remains red and is excreted with feces Fecal occult blood test; now fecal immunochemical test –FOBT used dye adsorbed on paper to detect Fenton reaction catalyzed by heme iron –FIT uses Ab against globin portion of hemoglobin

19
Hemorrhage into cavities Pleural hemorrhage—hemothorax Build-up of pressure prevents lung expansion Prevents gas exchange May lead to lung collapse Instigates coughing or hiccups, which exacerbates bleeding Pericardial hemorrhage—hemopericardium Build-up of external pressure inhibits filling Cardiac tamponade = compression Intracranial hemorrhage Always bad because of the rigid cranium CSF pressure increases rapidly if bleeding rate is greater than rate of fluid resorption

20
Hemodynamics Maintenance of blood volume Maintenance of blood pressure Mainenance of clot-free flow plasmin Development of clot in response to vascular damage—hemostasis thrombin-fibrin

21
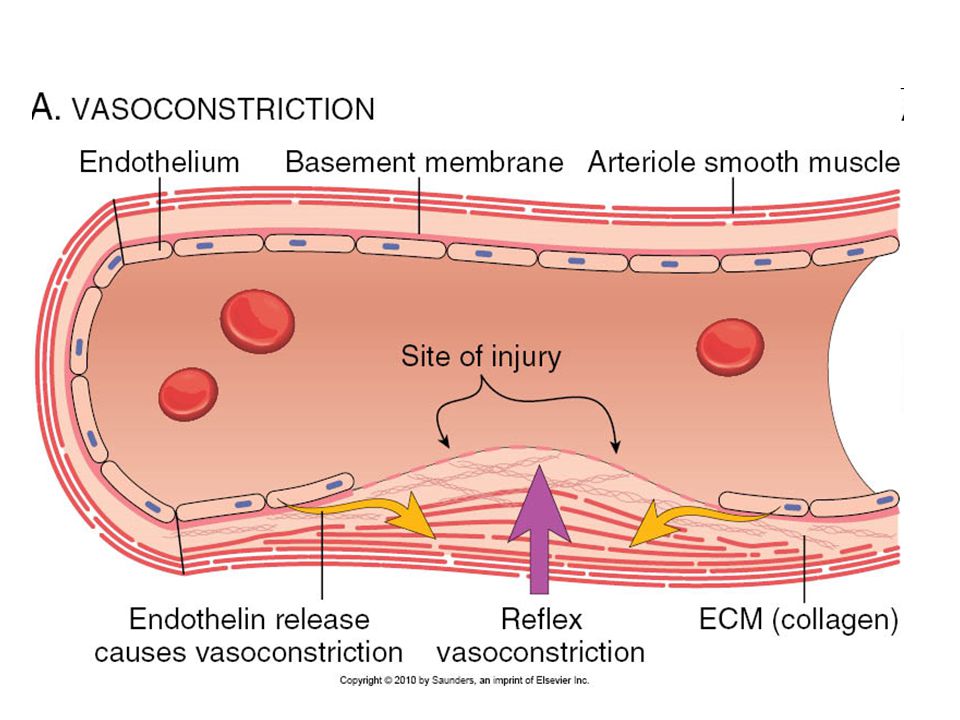
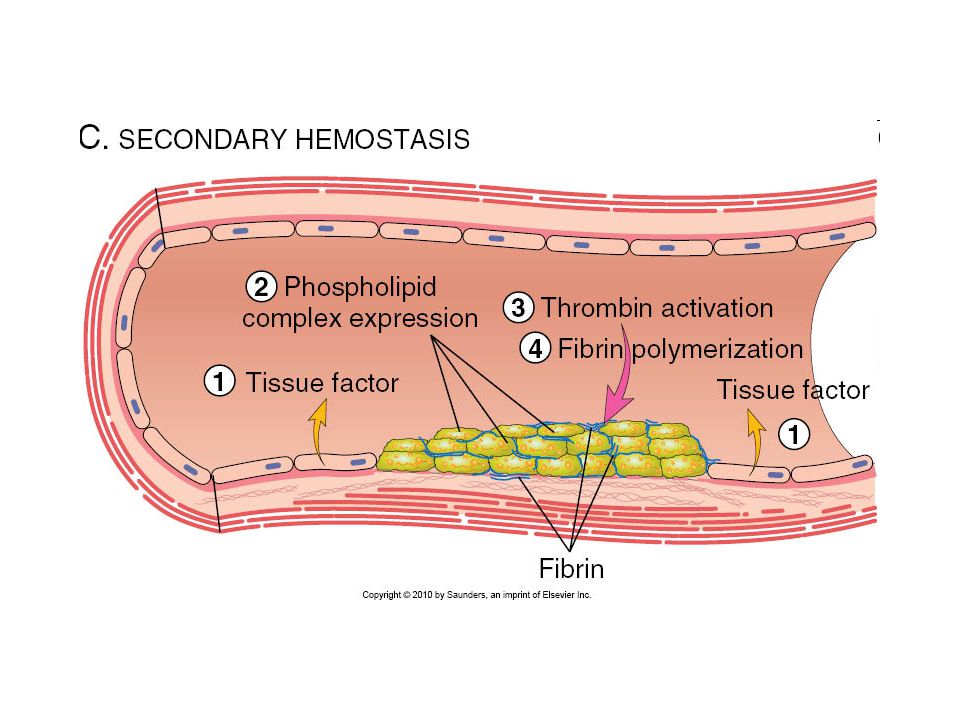
Mechanism of hemostasis Reflex sympathetic noradrenergic vasoconstrictor system activated locally Damaged vascular endothelium releases endothelin 10 times more potent than angiotensin II Platelets contact collagen—primary hemostasis Adhere: GpIb receptor tethered to collagen via vWF Secrete: ADP, TxA2, Ca++, growth and clotting factors Aggregate: Ca++ bridges with surface phosphoserine Coagulation cascade—secondary hemostasis Stimulated by tissue factor (factor III) Platelets, fibrin, net of captured RBCs and WBCs
 Platelets, fibrin, net of captured RBCs and WBCs")
22
Primary hemostatic clot formation Platelets are activated by contact with Extra Cellular Matrix Circulating von Willebrand Factor tethers platelet glycoprotein receptors to ECM collagen Thrombin is released to cleave fibrinogen creating fibrin nets that capture more platelets as well as RBCs and WBCs Platelets contract with microtubular contractile proteins, consolidating plug

23
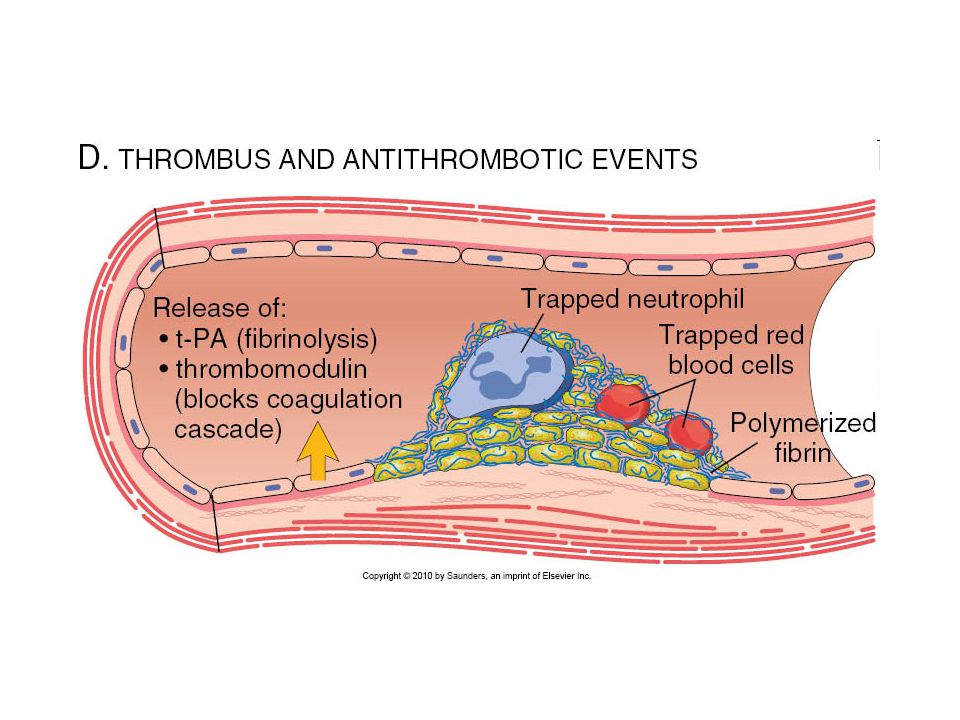
Hemostatic clot resolution tPA, tissue plasminogen activator, cleaves plasminogen to plasmin Plasmin digests fibrin clot Tightly regulated yin-yang of hemostasis

28
Platelet structure Anuclear cell fragments synthesized in marrow Surface glycoprotein Ib and IIa/IIIb receptors Internal alpha granules containing Factors V and VIII and IV Fibrinogen, fibronectin, thromboxaneA2 PDGF, TGF-b Internal dense granules containing ATP, ADP and Ca++ Histamine, serotonin, epinephrine Internal canaliculi—open canals Contractile cytoskeletal fibers

29
Platelet structure

30
Platelet actions Adhesion to extracellular matrix GpIb links to collagen via vWF GpIIb/IIIa links platelets via fibrinogen Secretion from granules into canaliculi and exterior Transition of phosphlipids to outer lamina Aggregation Primary hemostatic plug Contraction Secondary hemostatic plug

31
Platelet aggregation

32
Clotting v. thrombosis THROMBUS: Blood that has solidified within the vascular lumens or cardiac chambers CLOT: Blood that has solidified anywhere else THROMBOEMBOLISM: Portion of thrombus that travels through the vasculature to form a plug elsewhere EMBOLISM: vascular plug, not always from a thrombus

33
Consequences of acute hemorrhage Loss of blood beyond a certain volume will cause systemic hypotension rapid compensation by the baroreceptor response leads to peripheral vasoconstriction fluids shift from the interstitial into the IV compartment slower response from the renin-angiotensin-aldosterone system results in vasoconstriction and retention of sodium and water by the kidney antidiuretic hormone (ADH) also kicks in, acts on nephron to promote water resorption Loss of blood beyond the body's ability to compensate will cause systemic hypotension, reduced cardiac filling, reduced tissue perfusion, loss of erythrocytes and their Hb, hypoxemia, and a further cascade of events called shock
 also kicks in, acts on nephron to promote water resorption Loss of blood beyond the body s ability to compensate will cause systemic hypotension, reduced cardiac filling, reduced tissue perfusion, loss of erythrocytes and their Hb, hypoxemia, and a further cascade of events called shock")
34
Hypovolemic, cardiogenic shock Causes Blood loss Dehydration Reduced cardiac output Deranged peripheral vasomotor control Consequenses Inadequate perfusion Hypoxia, lactic acidosis Recovery dependent on duration and severity

35
Stages of Shock Early Stage Compensatory mechanisms maintain perfusion of vital organs Include increased heart rate and increased peripheral resistance Progressive Stage Compensatory systems no longer adequate with tissue hypoperfusion Onset of circulatory and metabolic imbalance, especially metabolic acidosis from lactic acidemia Irreversible Stage Organ damage and metabolic disturbances Survival not possible

36
Clinical consequences Hypotension Weak, rapid pulse (tachycardia) Shallow rapid breathing (tachypnea) Cool, damp, cyanotic skin Tissue injuries are due to hypoxia
 Shallow rapid breathing (tachypnea) Cool, damp, cyanotic skin Tissue injuries are due to hypoxia")
Similar presentations










 http://usmlewiki.org/index.php?title=USMLE_Wiki:Hemodynamic_Disorders http://www.pathguy.com/lectures/fluids.htm#intro http://www.pathologyoutlines.com/coagulation.html.>")


 and plasma (the liquid in which the cells.>")







