Download presentation
Presentation is loading. Please wait.

1
Wound Breakdown, Fungating Lesions, Pressure Sores, Fistulae
Rebecca Owen

2
Objectives Stages of Wound Healing Fungating Lesions overview
Types of wound + dressing suggestions Pressure Sores – common areas and treatment pathway Fistulae overview Summary

3
Stages of Wound Healing
Haemostasis Clotting cascade Inflammatory Bacteria and debris phagocytosed and removed Release of factors causing migration + proliferation Proliferative Angiogenesis, collagen deposition, granulation tissue formation, epithelialisation, wound contraction Remodelling Collagen remodelled and realigned along tension lines and unneeded cells removed by apoptosis

4
Wound Healing Phases

5
Wound Healing – Primary Intention
“Involves epidermis and dermis without total penetration of dermis healing by process of epithelialization” When wound edges are brought together so that they are adjacent to each other (re-approximated) Minimizes scarring Most surgical wounds Wound closure is performed with sutures (stitches), staples, or adhesive tape Examples: well-repaired lacerations,well reduced bone fractures,healing after flap surgery
 Minimizes scarring. Most surgical wounds. Wound closure is performed with sutures (stitches), staples, or adhesive tape. Examples: well-repaired lacerations,well reduced bone fractures,healing after flap surgery.")
7
Wound Healing – Secondary Intention
The wound is allowed to granulate Granulation results in a broader scar Healing process can be slow due to presence of drainage from infection Wound care must be performed daily to encourage wound debris removal to allow for granulation tissue formation Surgeon may pack the wound with a gauze or use a drainage system examples:gingivectomy,gingivoplasty,tooth extraction sockets, poorly reduced fractures.

8
Wound Healing – Tertiary Intention
(Delayed primary closure or secondary suture): The wound is initially cleaned, debrided and observed, typically 4 or 5 days before closure. The wound is purposely left open examples:healing of wounds by use of tissue grafts.
: The wound is initially cleaned, debrided and observed, typically 4 or 5 days before closure. The wound is purposely left open. examples:healing of wounds by use of tissue grafts.")
14
Fungating Lesions Can be associated with
Pain Pruritis Exudate Malodour Bleeding Infection Consider topical morphine, NSAIDs (pruritis), abx, Treat exudate + infection with appropriate dressing
, abx, Treat exudate + infection with appropriate dressing.")
15
Fungating Lesions Malodour Psychological Support
Clense and debride surface Topical/systemic metronidazole Live Yoghurt (topically) Manuka Honey (Activon) (topically) Mask odour with camphor, herbs,incense Psychological Support
 Manuka Honey (Activon) (topically) Mask odour with camphor, herbs,incense. Psychological Support.")
17
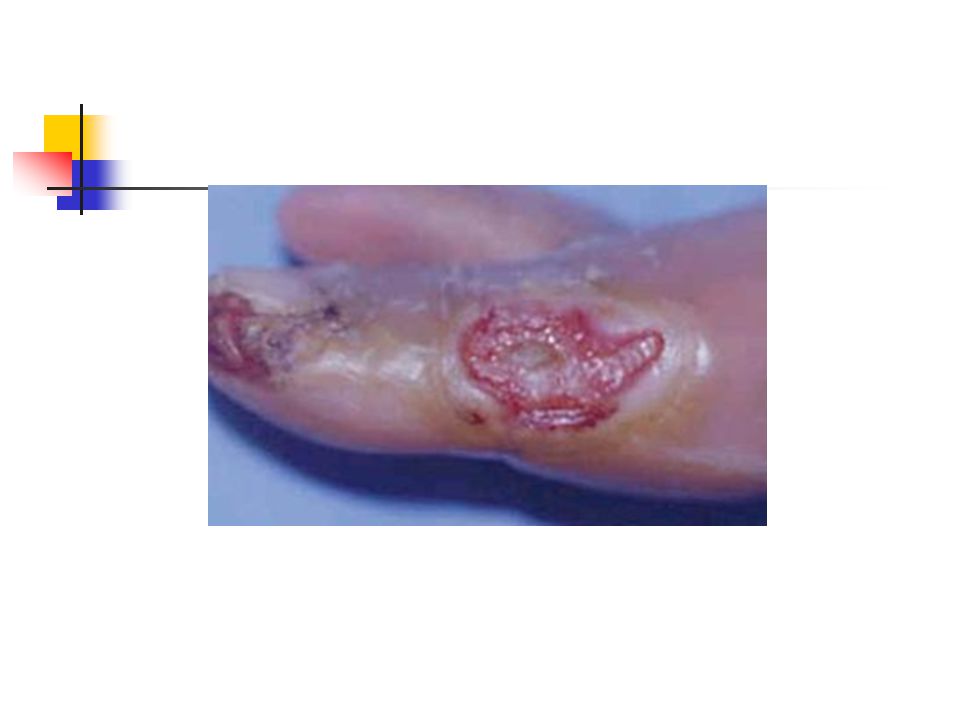
Skin Tear Occurs when friction + shearing forces cause tissue layers to slide across each other breaking blood vessels Caused by sliding patients in bed,agitated patients moving in bed, removal of adhesive dressings

18
Skin Tear Management Remove dressings using “lateral pull” technique
Mepitel dressing + dry gauze Change Mepitel every 5-7 days Change gauze when saturated

20
Wet Wound with Granulating Tissue
Aims Minimise dressing changes Relieve the pressure that caused the ulcer If increasing exudate then consider infection Maximise nutrition and hydration Suggested dressing – Aquacel Place sheets in wound bed and cover with dry dressing Cover dressing depends on wetness Daily – Gauze; 2-3/7 – Alldress, 3-5/7 – Allevyn/Mepilex Multiple layers of aquacel can minimise dressing changes Change Aquacel when it has turned into a gel

22
Cellulitis Local infection of dermis and subcutaneous tissue characterised by spreading redness, pain and swelling. Monitor demarcation by marking and dating the skin Consider systemic/topical antibiotics Use Mepitel on wound bed to reduce surface pain Change every 7/7 or PRN

24
Sacral Ulcer Remove/prevent pressure on area Observe for infection
If problems with incontinence – consider barrier cream i.e. Cavilon Sacral Shaped Tegasorb – dressing of choice

25
Applying a Sacral dressing
Fold sacral dressing in half Pinch the fold to form a crease "Bookmarking" Peel off the entire backing Insert "bookmark" into the patient's fold, above the rectum and secure the dressing up the middle Secure the dressing out the sides using the heat of your hand and slight pressure to help it adhere Slowly peel away the border while securing the tegaderm with your fingers

27
Clean Wound with Granulating Tissue
Remove/prevent pressure on affected area Maximise nutrition and hydration Sugessted foam dressing such as Mepilex Dressings can remain on wound for 7/7

29
Wound with Yellow Slough
Stage X as wound bed cannot be visualised Pain management with dressing changes 2 options of treatment: Option 1 - cut silver dressing, such as Acticoat to fit into the wound bed and moisten with sterile water. Cover with a light dressing (gauze and tape or “island dressing” such as Alldress). Ensure daily that Acticoat dressing is moist. Change Acticoat 3/7. Option 2 - Spread a thin layer of Iodosorb on a gauze and place in wound bed.Cover with island dressing (such as Alldress) or foam. Change dressing q 3 days, when Iodasorb changes to a creamy colour. (NB) make sure patient doesn’t have thryroid issues—Iodosorb has iodine & contraindicated if thyroid condition or breast-feeding mother).
. Ensure daily that Acticoat dressing is moist. Change Acticoat 3/7. Option 2 - Spread a thin layer of Iodosorb on a gauze and place in wound bed.Cover with island dressing (such as Alldress) or foam. Change dressing q 3 days, when Iodasorb changes to a creamy colour. (NB) make sure patient doesn’t have thryroid issues—Iodosorb has iodine & contraindicated if thyroid condition or breast-feeding mother).")
31
Diabetic/Neuropathic Ulcer
Most common on plantar aspect of foot,heels and over metatarsal heads Dry,warm, cracked, fissured skin, thickened nails Usually no oedema/exudate Causes – peripheral neuropathy,arterial insufficiency, poor microvascular circulation, inadequate blood glucose control Treatment – debridement plus mepilex/Allevyn + Intrasite gel

32
Pressure Sores Several factors that increase risk of developing a pressure sore: Mobility problems Poor nutrition Underlying health condition Age >70 yrs Urinary &/or bowel incontinence Serious mental health conditions

34
Treatment of Pressure Sores
Changing position Mattresses and cushions Dressings Creams and ointments Antibiotics Nutrition Debridement Maggot therapy Surgery

36
Fistulae Abnormal communication between 2 hollow organs or between a hollow organ and the skin Aetiology Anastomotic leaks Trauma - often iatrogenic post surgery Inflammatory bowel disease Malignancy Radiotherapy

37
Fistulae Types Rectovaginal/Rectovesical fistulas
Conservative/Surgical Enterocutaneous fistulas Simple Single orifice with intact abdominal wall Multiple Multiple orifices in abdominal wall Disrupted Fistula caused by dehiscence or surgical wound/scar

38
Imaging Important to determine anatomy of fistula
Fistulography will define tract Small bowel or barium enema will define state of intestine or distal obstruction US and CT will define abscess cavities

42
Management of Fistulae
Usually conservative management - at least initially - consisting of: Skin protection Upper GI contents are very corrosive Correction of fluid and electrolyte loss Require careful fluid balance & restoration of blood volume Correction of acid-base imbalance H2 Antagonist, proton pump inhibitor to reduce gastric secretions Somatostatin analogues (e.g. Octreotide) to reduce GI and pancreatic secretions
 to reduce GI and pancreatic secretions.")
43
Management of Fistulae
Tissue viability review Nutritional support Restrict oral intake and possibly an nasogastric tube Malnutrition corrected with either parenteral or enteral nutrition Total parenteral nutrition given via Dacron-cuffed tunneled feeding line Radiological screening to ensure tube in correct site Enteral nutrition can be given distal to fistula Control of sepsis Abscess cavities should be drained Antibiotics

44
Enterocutaneous fistulas will not close if:
There is total discontinuity of bowel ends There is distal obstruction Chronic abscess cavity exists around the site of the leak Mucocutaneous continuity has occurred

45
Fistulas are less likely to close if:
They arise from disease intestine (e.g. Crohn's Disease) They are end fistulae The patient is malnourished They are internal fistulas
 They are end fistulae. The patient is malnourished. They are internal fistulas.")
46
60% will close in one month once sepsis has been controlled with conservative treatment
Mortality associated with fistula is still at least 10% Surgery should be considered if fistula does not close by days

47
Summary Fully assess area and cleanse thoroughly
Use appropriate dressing – if in doubt ask Treat malodour Be aware need of ongoing psychological support

48
Any Questions?

49
References Symptom Management in Advanced Cancer; (2009) Twycross, Wilcock, Toller. Blowers A L Irving M. Enterocutaneous fistulas. Surgery 1992; 10.2: 27 – 31 Dubrick S J, Maharaj A R, McKelvey A A. Artificial nutritional support in patients with gastrointestinal fistulas. World J Surg 1999; 23: Mcintyre P B. Management of enterocutaneous fistulas: a review of 132 cases. Br J Surg 1984; 71:

Similar presentations























, However it is often misdiagnosed and mistreated.>")












