Download presentation
Presentation is loading. Please wait.

1
Clinical pharmacy in gastroenterology

2
The structure of digestive or alimentary tract

3
Digestion is the first stage of metabolism
This system does secretory, motor, absorption, excretion and immune functions

4
Anatomico-physiological bases
Secretory function - formation and exudation of digestive juices into intestinal lumen Daily secretion: 1,5 l saliva, 2,5 l gastric juice, 1,0 l pancreas juice, 1,2 l bile, 2,5 l intestinal juice

5
Anatomico-physiological bases
Motor function - food movement into intestinal pipe and its permanent mixing with digestive juices Absorbtion - absorption of some ingredients from undigested food and indigestible material

6
Anatomico-physiological bases
Excretion - moving off undigested food remainders and also some matters picked out in intestinal lumen Immune function In wall of large intestine there are accumulations of lymphoid tissue - “Peyer’s plaques”, where ripening of lymphocytes takes place

7
Anatomico-physiological bases
Stomach Duodenum Small intestine Large intestine

8
Anatomico-physiological bases
Basic stomach functions: physical and chemical processing of food, his depositing and evacuation; participation in metabolism; participation in hemostasis (synthesis of gastromucoprotein by parietal cells etc.); participation in water-salt metabolism; Synthesis of prostaglandines and gastrointestinal hormones
; participation in water-salt metabolism; Synthesis of prostaglandines and gastrointestinal hormones.")
9
Клиническая фармация в гастроэнтерологии
Factors that play the great role of the development of inflammation diseases in the gastroduodenal area Protective factors mucus Ionic gradient bicarbonates prostaglandins Epithelial cells Mucus membrane blood supply Aggression factors Drugs and medicines (NSAIDs) hydrochloric acid Pepsin Helicobacter pylori Клиническая фармация в гастроэнтерологии
 hydrochloric acid. Pepsin. Helicobacter pylori. Клиническая фармация в гастроэнтерологии.")
10
Ways of examination: questioning
The main complaints of GIT impairment: Pain (in epigastric area) Appetite disorders Dysgeusia Eructation Heartburn Nausea Vomitting Constipation Diarrhea Meteorism Fatigue Клиническая фармация в гастроэнтерологии
 Appetite disorders. Dysgeusia. Eructation. Heartburn. Nausea. Vomitting. Constipation. Diarrhea. Meteorism. Fatigue. Клиническая фармация в гастроэнтерологии.")
11
Laboratory and instrumental methods of examination
Fiber-optic gastroduodenoscopy Клиническая фармация в гастроэнтерологии

12
Laboratory and instrumental methods of examination
Colonoscopy and biopsy Клиническая фармация в гастроэнтерологии

13
Laboratory and instrumental methods of examination
X-ray examination of GIT Клиническая фармация в гастроэнтерологии

14
Laboratory and instrumental methods of examination
Bacteriologic, histologic and fast urea test of Н. Pylori Клиническая фармация в гастроэнтерологии

15
Laboratory and instrumental methods of examination
Non-invasive test : Breath test with urea Клиническая фармация в гастроэнтерологии

16
An algorithm approach to the diagnosis of GIT disorders
Клиническая фармация в гастроэнтерологии

17
Laboratory and instrumental methods of examination
Hematology Клиническая фармация в гастроэнтерологии

18
Laboratory and instrumental methods of examination
Urinalysis and blood biochemistry tests Клиническая фармация в гастроэнтерологии

19
Laboratory and instrumental methods of examination
Faeces analysis Клиническая фармация в гастроэнтерологии

20
Main syndromes in gastroenterology:
Gastric dyspepsia Intestinal dyspepsia Maldigestion and malabsorption Hypovitaminosis Gastrointestinal bleeding Asthenoneurotic syndrome Anemic syndromes Pain syndrome

21
Syndromes in GIT disorders
Hypovitaminosis: skin dryness, angular cheilosis, stomatitis, hair loss, trophic changes of nails

22
Basic stomach diseases
Chronic gastritis - chronic inflammatory-dystrophyc process in stomach mucous, being attended with violation of cells regeneration processes and progressing atrophy of glandular epithelium

23
Basic stomach diseases
Chronic gastritis Chronic autoimmune gastritis (type A) Chronic gastritis (type B) In accordance with dominant etiologic factor…
 Chronic gastritis (type B) In accordance with dominant etiologic factor…")
24
Basic stomach diseases
Chronic autoimmune gastritis (type A) - variant of chronic gastritis, conditioned by appearance of antibodies to parietal (acid-secretory) cells of stomach mucous
 - variant of chronic gastritis, conditioned by appearance of antibodies to parietal (acid-secretory) cells of stomach mucous.")
25
Basic stomach diseases
Etiology At the beginning of this disease there is fundamental importance of combination of the exogenic and endogenic factors Pathogeny Along of antibodies making to parietal cells of mucous stomach takes place her damage. Hereinafter develops diffuse atrophy of stomach mucous, his secretory function lowers, up to significant secretory insufficiency. In part of cases there is a produce of auto-antibodies to gastromucoprotein (internal Castle’s factor) then which lead to the development of В12-deficiency anemia.
 then which lead to the development of В12-deficiency anemia.")
26
Chronic autoimmune gastritis (type A)
Clinical manifestations/ syndromes 1.Pain syndrome: pain in epigastric area, temporary aching after food. Patients complaints about heaviness or sense of stomach enlargement, pressure in epigastric area and left subcostal area. 2.Syndrome of gastric dyspepsia: lowering of appetite, disagreeable taste in mouth, eructation, nausea with possible vomiting. 3.Syndrome of intestinal dyspepsia: rumbling sounds in abdomen, flatulency, leaning to diarrhea.

27
Chronic autoimmune gastritis (type A)
Clinical manifestations/ syndromes 4.Maldigestion and malabsorption: dehydration due to diarrhea, hypovitaminosis, weight loss. 5.Neurotic (asthenoneurotic) syndrome: weakness, irritability, paresthesias, cold sensations in the extremities, neurogenic, cardiogenic, vascular symptoms (angina like pains, hypotension).
 syndrome: weakness, irritability, paresthesias, cold sensations in the extremities, neurogenic, cardiogenic, vascular symptoms (angina like pains, hypotension).")
28
Chronic autoimmune gastritis (type A)
Diagnostic criteria of chronic gastritis type А Clinical manifestations Special methods of investigation Complaints - blunt pains in epigastrium, appetite loss, disagreeable taste in mouth, nausea, heaviness after food, belch rotten, diarrheas. Examination - coated tongue, symptoms hypovitaminosis (skin dryness, hair loss, stomatitis and etc.), flatulency. X-ray examination- tone and peristalsis is weak, forced stomach evacuation. Gastroscopy faded mucous. Biopsy - stomach mucous atrophy and inflammation signs
, flatulency. X-ray examination- tone and peristalsis is weak, forced stomach evacuation. Gastroscopy faded mucous. Biopsy - stomach mucous atrophy and inflammation signs.")
29
Chronic autoimmune gastritis (type A) Principles of medicinal therapy
correction of gastric secretion violations (substitution therapy, forcing of gastric secretion). forcing of mucous regeneration process (anabolic hormones, biologic stimulants). correction of metabolic disturbances (aminoacids, vitamins, anabolic hormones). correction of motored violations (prokinetics). correction of intestinal digestion violations (polyenzymatic medications: festal, panzynormum).
. forcing of mucous regeneration process (anabolic hormones, biologic stimulants). correction of metabolic disturbances (aminoacids, vitamins, anabolic hormones). correction of motored violations (prokinetics). correction of intestinal digestion violations (polyenzymatic medications: festal, panzynormum).")
30
Basic stomach diseases
Chronic gastritis (type B) - variant of chronic gastritis, induced by bacterium Нelicobacter pylori.
 - variant of chronic gastritis, induced by bacterium Нelicobacter pylori.")
31
Basic stomach diseases Etiologic factors may be
Endogenous Exogenous

32
Basic stomach diseases
Endogenous factors Genetic predisposition: augmentation of parietal cells; surplus gastrin liberation; rise of pepsinogen level in blood; Violation in gastroduodenal movements; lack of pepsin inhibitors; violation of Ig A structure; blood group 0 (I); positive Rh-factor; Presence of antigenes HLA В5, В15, В35.
; positive Rh-factor; Presence of antigenes HLA В5, В15, В35.")
33
Basic stomach diseases
Exogenous factors violation of nutrition; harmful habits (smoking, alcohol, abuse of coffee); professional influences and mode of life; damaging action of medicinal preparations (anti-inflammatory drugs, corticosteroids, some antibiotics, iron preparations, potassium). To be infected by Helicobacter pylori
; professional influences and mode of life; damaging action of medicinal preparations (anti-inflammatory drugs, corticosteroids, some antibiotics, iron preparations, potassium). To be infected by Helicobacter pylori.")
34
Basic stomach diseases Clinical manifestations
Pain syndrome: “hungry” pain (nighttime pain) in epigastric area, which can stop after food intake; Neurotic syndrome: irritability, fatiguability, bad sleep; Syndrome of gastric dyspepsia: heartburn, nausea, sour belch; Syndrome of intestinal dyspepsia: constipations.
 in epigastric area, which can stop after food intake; Neurotic syndrome: irritability, fatiguability, bad sleep; Syndrome of gastric dyspepsia: heartburn, nausea, sour belch; Syndrome of intestinal dyspepsia: constipations.")
35
Basic stomach diseases
Diagnostic criterions of chronic gastritis type В Clinical manifestations Special methods of investigation Complaints - hungry epigastric pains, vomiting on pains height, heart-burn, belch sour, constipation. Examination - sickliness attached to epigastral palpation X-ray exam- raised tonus of stomach antral area, peristalsis is weakened, hypersecretion signs. Gastroscopy - edema and hyperemia of mucous, folds hypertrophy mucous stomach. Biopsy - signs of chronic inflamma-tion and hyperplasia mucous of stomach antral area.

36
Symptoms of Dyspepsia Ulcer-like Dominant Dysmotility-like Dominant
Nocturnal pain Localized epigastric burning Better with food Heartburn Retrosternal burning Nausea Bloating Early satiety Worse with food

37
Major Causes of Dyspepsia
Williams 1988 Stanghellini 1996 Heikkinen (n=1386) (n=1057) (n=766) % of Patients with Diagnosis Gastric Cancer Peptic Ulcer Esophagitis/ Functional
 (n=1057) (n=766) % of Patients with Diagnosis. Gastric Cancer Peptic Ulcer Esophagitis/ Functional.")
39
Helicobacter pylori A spiral shaped, Gram-negative, microaerophilic, and flagellated bacterium, living in the stomach and duodenum About 3 microns long with a diameter of about 0.5 micron Causing up to 80% of peptic ulcers, more than 90% of duodenal ulcers, and some types of gastritis Rediscovered in 1982 by the laureates and made connection with stomach ulcers and gastritis Helicobacter pylori (blue bars, curved, 2-4 microns) localized in the mucus on the mucous surface, at the intercellular lines. Photo: tangential section of the gastric mucous
 localized in the mucus on the mucous surface, at the intercellular lines. Photo: tangential section of the gastric mucous.")
40
Epidemiology Approximately two-thirds of the world's population is infected with H. pylori. 70% - 90% in developing countries 25% - 50% in developed countries Over half the population is infected in early childhood in China. Most of those infected never have symptoms. The bacteria are most likely spread from person to person through fecal-oral or oral-oral routes. Possible environmental reservoirs include contaminated water sources. The source of H.pylori is unknown yet .

41
H. pylori Epidemiology

42
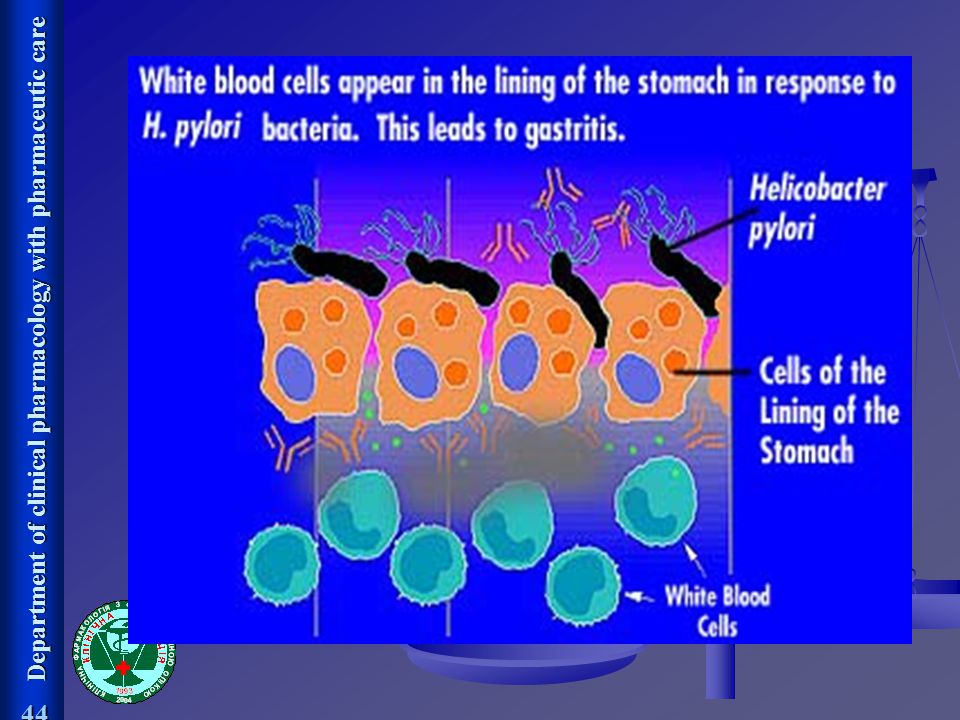
Pathogenicity Stomach acid Gastric epithelium
H.pylori lives in the mucus lining to escape from the highly acidic gastric juice. (Its helical shape facilitates its penetration of the mucus layer.) It can fight the acid by excreting an enzyme called urease. The immune system responds to the infection by sending white cells, killer T cells, and other infection fighting agents. However, they cannot easily get through stomach lining to reach the infection. As the immune response grows, immune cells die and release destructive compounds on the stomach lining cells. Within a few days, gastritis and perhaps eventually a peptic ulcer results. Gastric epithelium
 It can fight the acid by excreting an enzyme called urease. The immune system responds to the infection by sending white cells, killer T cells, and other infection fighting agents. However, they cannot easily get through stomach lining to reach the infection. As the immune response grows, immune cells die and release destructive compounds on the stomach lining cells. Within a few days, gastritis and perhaps eventually a peptic ulcer results. Gastric epithelium.")
45
Symptoms The most common ulcer symptom is burning pain in the epigastrium (the upper middle region of the abdomen). The pain typically occurs when the stomach is empty. Less common symptoms include nausea, vomiting, and loss of appetite. Bleeding can also occur. Recent studies have shown an association between long-term infection and the development of gastric cancer, which is the most common cancer in China.
. The pain typically occurs when the stomach is empty. Less common symptoms include nausea, vomiting, and loss of appetite. Bleeding can also occur. Recent studies have shown an association between long-term infection and the development of gastric cancer, which is the most common cancer in China.")
46
Testing for H. pylori Test Sensitivity Specificity Cost Comments
C13 or C14 90% to 100% 96% to 100% ++ Limited - requires urease breath nuclear medicine test department Serology 91% to 98% 75% to 80% + Widely available commercial labs Capillary % to 90% 75% to 80% + Office test, must purchased by doctor admin Endoscopic 99% 99% ++++ Requires biopsy specialist Invasive (Cutler A. Gastro 1995;109:136. Megraud F. Scand J Gastro 1996;215:57)
")
47
Fundamental rules of anti-ulcer therapy
Steady lowering of acid reaction (рН > 3 not less h/day): Proton pump ihibitors Н2-histaminoblockers Antacids Eradication of Helicobacter pylori: Antibiotics Bismuth Derivative nitromidazole Rise cytoprotection (peculiarly attached to gastric ulcers ): Sucralfate Colloid bismuth Synthetic analogues prostaglandins Reparants Use of medications with minimum side effects Optimum compliance (observance by treatment program)
: Proton pump ihibitors. Н2-histaminoblockers. Antacids. Eradication of Helicobacter pylori: Antibiotics. Bismuth. Derivative nitromidazole. Rise cytoprotection (peculiarly attached to gastric ulcers ): Sucralfate. Colloid bismuth. Synthetic analogues prostaglandins. Reparants. Use of medications with minimum side effects. Optimum compliance (observance by treatment program)")
48
H. pylori Eradication (All given for one week)
Treatments of choice Regimen PPI Antibiotics PPI - AC BID Amoxicillin 1 g bid Clarithromycin 500 mg bid PPI - MC BID Metronidazole 500 mg bid Clarithromycin 250 mg bid Alternate PPI - BMT BID Bismuth 2 tabs qid Metronidazole 250 mg qid Tetracycline 500 mg qid

49
H. pylori Eradication cure by one medication does not adapt
First line therapy:“triple therapy”: proton pump inhibitor (omeprazolum 20 mg twice/day or pantoprazolum 40 mg/ day) + antibiotics against Н. pylori (amoxicillin 1 g or metronidazol mg twice/day and clarithromycin (500 mg twice/day)) First/Second line therapy: “cure standard” - “quadrotherapy therapy” proton pump inhibitor (omeprazolum 20 mg twice/day or pantoprazolum 40 mg/ day) metronidazol (500 mg triplicate/day) tetracycline (500 mg quadruplicate/day) bismuth (120 mg quadruplicate/day) Course of treatment -10 days Second line therapy:«tripletherapy» includes proton pump inhibitor (omeprazolum 20 mg twice/day or pantoprazolum 40 mg/day) from first to tenth day clarithromycin (500 mg twice/day) levofloxacin (500 mg once/day)
 + antibiotics against Н. pylori (amoxicillin 1 g or metronidazol mg twice/day and clarithromycin (500 mg twice/day)) First/Second line therapy: cure standard - quadrotherapy therapy proton pump inhibitor (omeprazolum 20 mg twice/day or pantoprazolum 40 mg/ day) metronidazol (500 mg triplicate/day) tetracycline (500 mg quadruplicate/day) bismuth (120 mg quadruplicate/day) Course of treatment -10 days. Second line therapy:«tripletherapy» includes. proton pump inhibitor (omeprazolum 20 mg twice/day or pantoprazolum 40 mg/day) from first to tenth day. clarithromycin (500 mg twice/day) levofloxacin (500 mg once/day)")
50
Acid Suppression Therapy for Ulcer-like Functional Dyspepsia
H2-receptor antagonist for 4 weeks OR Proton pump inhibitor for 2 weeks

51
Receptor stimulation of acid secretion

52
Fundamental rules antihelicobacter therapy
In the same patient it is not allowed to repeat the previously used therapy which turned to be ineffective one If two types of treatment regimens are not effective , and there id no significant eradication, then it is necessary to determine the sensitivity of Н.рylori strain to the whole spectrum of used antibiotics Administration of back up “quadritherapy” regimen is desirable only after complete clarification of the failure of the different variants of “triple therapy” The presence of Н. рylori up to year after conducted therapy should be considered as an infection set-back, but and not einfection “Quadrotherapy” regimen must be used in case of infection set-back

53
Management of Ulcer-like Functional Dyspepsia
Ulcer-like Symptoms Dominant Education/lifestyle modification Test Hp + - Trial of acid suppression Eradicate Hp Reassess Success Failure Investigate Trial of prokinetic

54
Lifestyle Modification for Patients with Functional Dyspepsia
Small frequent meals Stop smoking Reduce alcohol Reduce caffeine Avoid irritating foodstuffs Maintain an ideal weight Review medications

55
Risk Factors for Stomach Cancer
Helicobacter pylori was the first bacterium to be officially recognized as a cancer-causing agent. Helicobacter pylori infection. Nitrates and nitrites are substances commonly found in cured meats, some drinking water, and certain vegetables, that can be converted by Helicobacter pylori, into compounds that have been found to cause stomach cancer in animals.

56
Helicobacter pylori: associated pathology
Gastritis B % Ulceration % Gastric Ca <1% Lymphoma (MALT) <1% De todas las patologías asociadas a la infección por Hp, la UGD es la que ha visto mas substancialmente modificado su manejo clínico por la irrupción de esta bacteria
 <1% De todas las patologías asociadas a la infección por Hp, la UGD es la que ha visto mas substancialmente modificado su manejo clínico por la irrupción de esta bacteria.")
57
Gastro-oesophageal reflux disease
chronic symptom of mucosal damage caused by stomach acid coming up from the stomach into the esophagus. GERD is usually caused by changes in the barrier between the stomach and the esophagus, including abnormal relaxation of the lower esophageal sphincter, which normally holds the top of the stomach closed, impaired expulsion of gastric reflux from the esophagus, or a hiatal hernia.

58
Alginate-containing antacid
Gastro-oesophageal reflux disease Endoscopic image of peptic stricture, or narrowing of the esophagus near the junction with the stomach: This is a complication of chronic gastroesophageal reflux disease and can be a cause of dysphagia or difficulty swallowing. Barrett’s oesophagus Alginate-containing antacid

59
Undiagnosed dyspeptic patient
Alginate-containing antacid Heart burn without “alarm symptoms” If symptoms persist after 1 week of regular treatment then H2 antagonist If symptoms persist after 2 weeks of regular treatment the patient should be referred to the general practitioner

60
THE END

Similar presentations







![Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.](/13/3809458/big_thumb.jpg "Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.>")

>")









 Stomach ulcer or peptic ulcer is the damage of the protective layer (lining) of stomach or gastrointestinal tract It may be.>")

