Download presentation
Presentation is loading. Please wait.

1
Lower Extremity Wounds: The role of the vascular technologist
Jesse Thomas, RVT UNC Health Care

2
Disclosures No relevant conflicts of interest to declare

3
Objectives Review types of wounds Discuss risk factors
Role of Duplex Imaging Role as a Technologist This presentation will NOT address the use of ultrasound as a wound management and/or treatment tool.

5
Types of Wounds Arterial Venous Neuropathic Small vessel/Vasculitis
Pressure ulcers

6
Arterial Ischemic wounds Result of inadequate blood supply
Tissue hypoxia and tissue damage Most commonly result of atherosclerotic disease (PAD)
")
7
PAD Narrowing of arteries to the limbs that reduces blood flow
More common in LE Atherosclerosis – build up of fatty deposits (plaque)
")
8
Arterial Risk Factors High cholesterol Aging HTN Diabetes Smoking
Family hx of cardiovascular disease Obesity

10
PAD Approximately 8 million people in the US 12-20% in those >60
Public awareness around 25% Associated with significant morbidity and mortality Source: National Center for Chronic Disease Prevention and Health Promotion

11
PAD May present with variety of signs/symptoms Claudication – to limp
Aching, cramping pain brought on by exercise and relieved with rest Calf, thigh, hips or buttocks

12
PAD Rest pain Non-healing ulceration gangrene

13
Arterial Ulcers Characteristics “punched out” appearance
Smooth wound edges Surrounding skin may exhibit dusky erythema Cool to touch Hairless, thin, brittle with shiny texture

14
Arterial Ulcers Typically lower leg Lateral foot Toes
Pressure points or where injury has occurred

15
Arterial Ulcers Jesse, why do I care what these look like and are you done showing these nasty pictures?

16
Role of Sonographer Patient history Physical exam ABI’s
Clues to what is going on before you put the transducer on the patient

17
Role of Duplex Presence or absence of disease Severity Physiologic
Anatomic Location Single level Asymptomatic claudication Multi-level Claudication Rest pain ulcerations

18
Pressures Ankle/Brachial Index (ABI) 1.0-1.2 Normal
may indicate presence of arterial obstruction < Evidence of arterial obstruction, claudication <0.40 associated with rest pain or tissue loss

19
Pressures--Toe Photoplethysmography (PPG)
Infrared light which responds to changes in blood content near the surface of the skin Waveform analysis and pressure measurement

20
Pressures--Toe Disease from the level of the ankle to the toe
Diabetics Wound healing potential Absolute number and index

21
Pressures--Toe A toe/ankle index >0.60 suggests the absence of hemodynamically significant obstruction between the ankle and the toe A toe/brachial index >0.60 suggests the absence of hemodynamically significant obstruction between the heart and the digit

22
Pressures--Toe

23
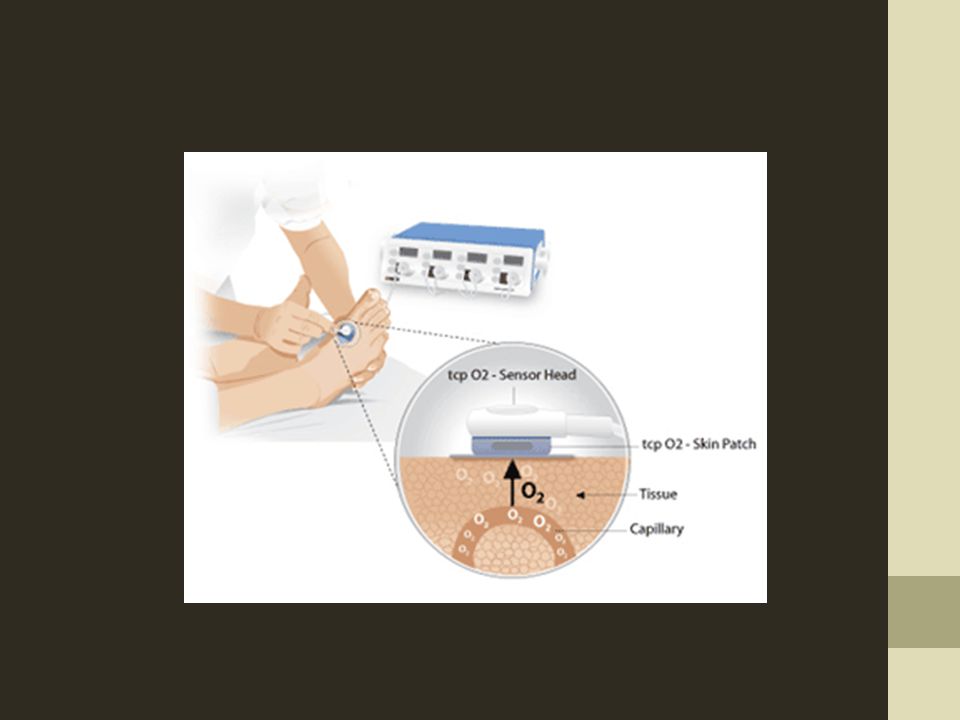
TCPo2 Transcutaneous oxygen tension Patient in supine position
Evaluates oxygen delivery to tissue Indirect measure of local blood flow Aids in determining wound healing potential Patient in supine position Small electrodes placed at chest, below knee, and 2 over dorsum of foot Electrodes in the sensors heat area underneath the skin to dilate capillaries Results recorded and measured in mmHg >30 mmHg – greater success for wound healing <30 mmHg - suggests high likelihood of wound not healing

26
Pressures--Segmental
Typically 3 or 4 cuff system High thigh, above knee, calf, ankle Measures pressure at each level >30mmHg gradient from level to level is significant >40mmHg indicates occlusion >20mmHg from side to side is also significant

27
Pressures--Segmental
Pitfalls include Medial arterial calcification Limb girth Inappropriate cuff size Can be uncomfortable for patient

28
Pressures--Segmental

29
Pulse Volume Recordings (PVR)
Measures pressure changes in the bladder of the cuff wrapped around the leg These changes reflect change in cuff volume Can use same cuffs as used for segmental pressures

30
PVR A 1mmHg pressure change detected in the cuff produces a 20mm deflection (amplitude) on the chart recorder Using appropriate size cuffs, a preset pressure is obtained A recording is then obtained

31
PVR

32
PVR/Segmental Pressures
PVR waveforms and segmental pressures are complimentary tests If differences exist then a source of error should be investigated

33
Duplex Image based evaluation
Looking for anatomic disease and physiologic disease

34
Duplex – Segmental

35
Duplex

36
PW Doppler--Duplex Velocity Ratio (VR) = 6.1 Velocity Ratio = v2/v1
V2= highest peak systolic velocity V1= proximal normal vessel Velocity Ratio (VR) = 6.1
 = 6.1.")
37
Arterial Ulcers Role of Duplex essential to understanding presence, location, and severity of disease Guides intervention and management Indicator wound healing potential

38
Changing Gears

39
Venous Ulcers Result of sustained venous hypertension (Chronic venous insufficiency) Incompetent valves or poor calf muscle pump Local venous dilatation and pooling Traps leukocytes that may release proteolytic enzymes that destroy tissues May also “trap” important growth factors within vein rendering them unavailable for wound repair

40
Venous 70%-90% of chronic wound cases
Estimated 2.5 million patients in the US Rarely fatal - can severely diminish quality of life

41
Venous Ulcers CVI Risk factors > Age Hx DVT Surgery
Restricted mobility CHF Cancer Obesity Smoking Family hx VTE Hypercoable state (Factor V Leiden, Protein C/S deficiency, etc.) Sedentary lifestyle Varicosities
 Sedentary lifestyle. Varicosities.")
42
Venous Ulcers Wound characteristics Gaiter region – medial malleolus
Superficial, irregular shape Skin shiny and tight (edema) Brown or purple discoloration – “stasis skin changes”
 Brown or purple discoloration – stasis skin changes")
43
Stasis Skin Changes

44
Varicose Veins

45
Varicose Veins

46
Varicose Veins

47
Varicose Veins Complications
Swelling Pain/aching itching Leg heaviness Phlebitis – inflammation of vein Superficial thrombophlebitis bleeding Cosmetic Not commonly associated with venous ulcers when isolated to the superficial system

48
Role of the Sonographer
Patient history Physical exam Clues to what is going on before you put the transducer on the patient

49
Role of Duplex Presence or absence of disease Severity Physiologic
Anatomic Location Deep Superficial

50
Venous Obstruction Presence or absence of deep or superficial venous obstruction Compression ultrasound

51
Venous Obstruction Thrombus Characteristics Acute Chronic
Softly echogenic Spongy Dilated vein Smooth borders Chronic Brightly echogenic Rigid Contracted vein Irregular borders Presence of collaterals

54
Acute or Chronic? These distinguishing characteristics are not absolute “Can be useful in estimating the age of a thrombus and the risk of its embolization.” (Techniques of Venous Imaging. Talbot, Oliver. 1992)
")
55
Venous Duplex Complete and careful evaluation Deep Superficial CFV Fv
Pop Tibials Gastrocs, soleals, etc. Superficial Great Saphenous Vein (GSV) Small Saphenous Vein (SSV) tributaries
 Small Saphenous Vein (SSV) tributaries.")
60
Venous Insufficiency Evaluation of reflux (deep and superficial)
Supine Manual hand augments Standing Rapid inflation/deflation cuff system “stresses” vein – hydrostatic pressure Valsalva Patient unable to stand

62
Venous Insufficiency Patient standing Cuff around calf
Rapidly inflates Measure reflux on cuff deflation Ergonomic challenges Patient limitations

66
Venous Insufficiency Normal values Abnormal
< 0.5 seconds Abnormal > 0.5 seconds Indication of valvular incompetency (reflux)
")
67
Perforator Assessment
Connection between deep and superficial systems Drains superficial into deep system Contain valves Associated with ulcer formation

68
Perforator Assessment
Dodd’s Boyd’s Cockett’s Name given by 1st physician who described them

70
Venous Duplex Other considerations Size of veins “map” of veins
May help determine intervention method Too large may not respond well to local sclerotherapy or some types of venous ablation “map” of veins Anatomical blueprint sometimes required Help guide intervening physician

71
Venous Ulcers Role of Duplex essential to understanding presence, location, and severity of disease Guides intervention and management

72
Conclusion Patients presenting with ulcerations to the vascular lab is a common occurrence Technologist and physician education important Use all available skills and tools to assess your patients Wound management is complex and your role is critical in providing the necessary vascular information

73
Thank you!

Similar presentations



























 A National Public Awareness Campaign from the P.A.D. Coalition and the National Heart,>")





