Download presentation
Presentation is loading. Please wait.

1
Summary of Panels and Next Steps Michael Marsiske AIR Meeting 11/10/2014

3
Rebok

5
Improving outcome assessment

6
Kueider & Gross

7
Transfer of Cognitive Training

8
Willis

9
Jaeggi

12
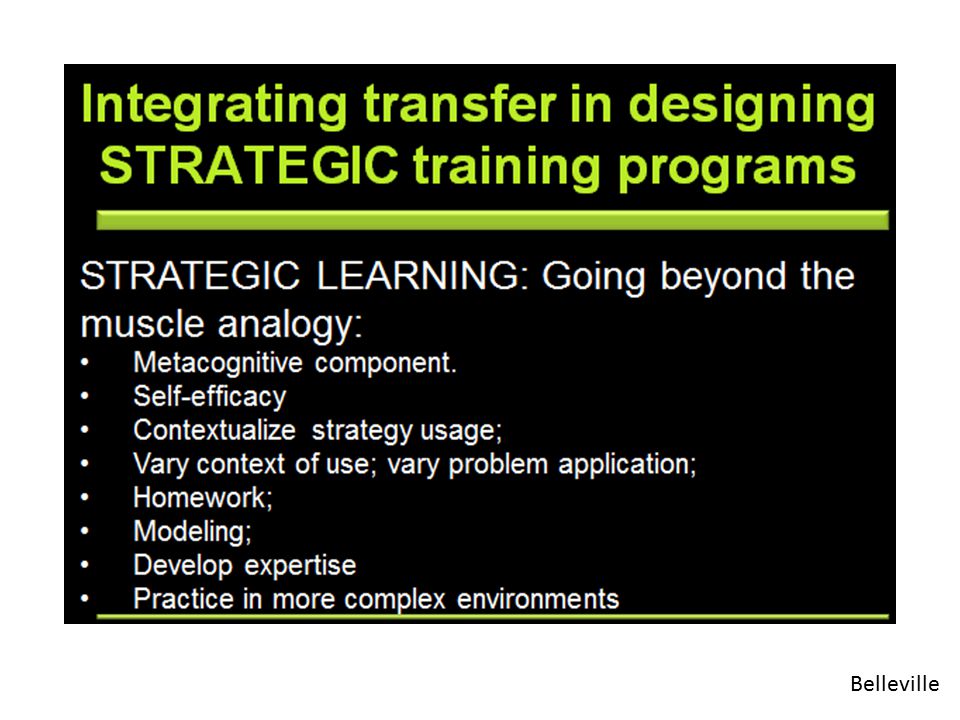
Belleville

14
Grappling with transfer Liz Stine-Morrow repeatedly asked the question: “What is transfer?” We have seen several answers today: – Generalization at the level of shared variance (Thorndike’s Law of Equivalent Elements) – Training on a mechanism that undergirds more complex cognition – A meta-cognitive skill, in which one recognizes and applies learning from one domain to another
 – Training on a mechanism that undergirds more complex cognition – A meta-cognitive skill, in which one recognizes and applies learning from one domain to another")
15
Grappling with transfer Robin West said: “Older adults really want to affect everyday memory skills”. The problem is that most training really hasn’t started at that outcome How did we get here? As Sherry Willis noted, in some ways early training research was a proof of concept. Training targets were selected because (a) they could be well controlled experimentally, and (b) they were known to be “age sensitive”
 they could be well controlled experimentally, and (b) they were known to be age sensitive .")
16
Grappling with transfer Today’s discussion suggests that we need to create some consensus about – What type of transfer we wish to achieve – What is the optimal approach for achieving that transfer But returning to Robin West: Starting with the goal of cognitive training – complex, functionally relevant everyday tasks. We have an exemplar:

17
Ball

19
What did Karlene say? Started with the observation of a functional problem (“people could not see” – was not a visual problem) Drew on basic research that there were multiple potential mechanisms at fault Developed training for multiple mechanisms The specific training approach for any participant might vary, based on need
 Drew on basic research that there were multiple potential mechanisms at fault Developed training for multiple mechanisms The specific training approach for any participant might vary, based on need.")
20
An alternative question: Can we leverage specificity of training? Rather than a negative feature of intervention, doesn’t it mean that we can be remarkably precise in targeting interventions? – “spot training”

21
Translation and Policy

22
West A consequence would be more widely available and extended dosages. Existing dosages are miniscule. For example…

23
Next steps Over a 5 week period, participants in original training spent up to 900 minutes in training That represents just 1.8% of the available time during that period. Over the ten year period, even those who received booster spent just 003% of time in training Education 21, rehabilitation science 22, and physical exercise science 23 all tell us that dosages must be continuous, ongoing, protracted, and embedded into everyday life Optimal delivery mechanism? Increasing dosage 21 Ary et al, 2010 23 Paterson & Warburton, 2010 22 Whyte & Barrett, 2012

24
But…shifting to extended dosages may have costs

25
Boot

27
Wally Boot’s been at the forefront of helping us see that many video game intervention studies are a mess. But: They work at least somewhat…

28
Four intervention arms 1. UFOV 2. Medal of Honor 3. Tetris 4. No contact control

29
…but so does Tetris!? A first-person shooter game that improves selective visual attention in young adults does so for elders too… Belchior, Marsiske, et al 2013. Computers in human behavior)
.")
30
As Wally’s own work says… People often enjoy them – Some participants (and my own mother) devote hundreds (or thousands) of hours to engaging games – (Teenagers are a testament to how engaging games can be) – That seems to give us a lens into how we can foster and support adherence with something that might also happen to be good for you Fun, engaging
 devote hundreds (or thousands) of hours to engaging games – (Teenagers are a testament to how engaging games can be) – That seems to give us a lens into how we can foster and support adherence with something that might also happen to be good for you Fun, engaging")
31
Implications for compliance? Maybe more importantly, older gamers are positively engaged by gaming more than they are by formal training programs Source: Belchior, Marsiske, Sisco, Yam & Mann, 2013 Belchior, P., Marsiske, M., Sisco, S. M., Yam, A., & Mann, W. (2013). Older adults’ engagement with a video game training program. Activities, Adapation and Aging.
. Older adults’ engagement with a video game training program. Activities, Adapation and Aging..")
32
…and they appear to experience widespread gains in visual processing speed, some measures of everyday function, and affect. Belchior, Marsiske et al., REVIVA Study (Robert Wood Johnson Foundation, manuscript in preparation) Elders will be compliant with up to three- months of in-home computer based training/gaming…
 Elders will be compliant with up to three- months of in-home computer based training/gaming….")
33
What are these video games doing? Cognitive practice? Engagement (stimulation, arousal, emotional benefits?) – As Liz Stine-Morrow has also said, this is a concept that needs clarification too Complexity (multiple abilities needed; widespread attentional monitoring and response), adaptive difficulty, and novelty all seem to be involved.
 – As Liz Stine-Morrow has also said, this is a concept that needs clarification too Complexity (multiple abilities needed; widespread attentional monitoring and response), adaptive difficulty, and novelty all seem to be involved..")
34
Training occurs in a context Resources Individual differences Cultural variation – A nonchalant claim to “go for a hike” or “learn a new language” is actually remarkably naïve Cognitive status and level of baseline ability

35
Cjaza

36
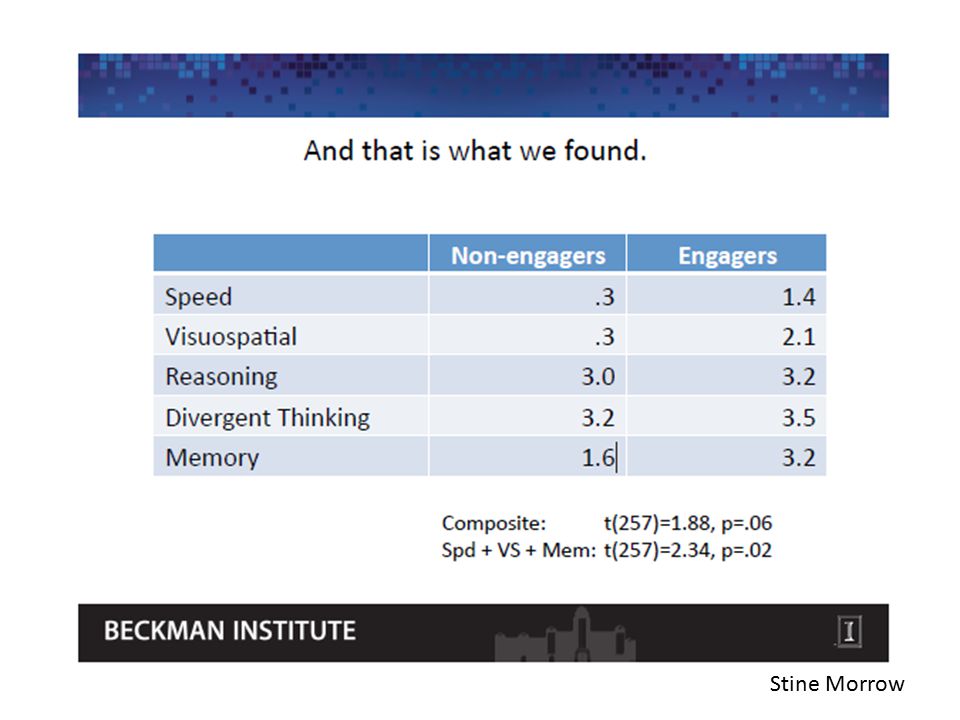
Stine Morrow

38
Multimodal interventions

39
The arsenal Arsenal Educate Brain Health Spot- train MoodEngage Jerri Edwards noted “training” is an umbrella term for a wide variety of approaches. So is “education”

40
Stine-Morrow

41
Stine Morrow

42
Design Randomized parallel-group study of cognitive training combined with exercise

44
Parisi

46
Carlson

47
What Alden Gross heard at GSA “Randomized trials are used to determine an average effect” But we have spoken a great deal about moderators and individual differences in training response…

48
Next steps It is tempting to use technology (internet, computer-based training programs 24-27 ) and increasingly available platforms (computers, tablets) to deliver longer, more adaptive, more multi-component interventions Technology access issues Appropriateness for cognitively frail elders? Same compliance issues as exercise interventions Absence of evidence regarding transfer Tailored interventions 24 Lumosity, http://www.lumosity.com/ 25 PositScience, http://www.positscience.com/ 26 Vigorous Mind, http://www.vigorousmind.com/ 27 Cogmed, http://www.cogmed.com/

49
Practice Effects: Nuisance?

50
Kueider & Gross

51
The easiest thing to do is to provide practice Arguably, practice effects are an active ingredient in any intervention effect While it is important to separate effects of retest from those of strategic training or adaptive drills, retest effects show how plastic the aged CNS is, behaviorally Can we leverage this?

52
3-year retest-gain in several Reasoning measures (ACTIVE control sample)
")
53
Practice by itself probably provides gains that are too narrow

54
Daily Practice Effects: Reasoning Allaire, J. C., & Marsiske, M. (2005). Intraindividual variability may not always indicate vulnerability in elders' cognitive performance. Psychology and Aging, 20, 390-401
. Intraindividual variability may not always indicate vulnerability in elders cognitive performance. Psychology and Aging, 20,")
55
Practice is even helpful in persons with early memory loss …perhaps because it invokes implicit learning mechanisms

56
Equivalent practice related gain, regardless of cognitive status Source: Marsiske & McCoy, in preparation Note that the function is quadratic, but never quite hits diminishing returns

57
Next steps

58
Key issues today What is transfer? How do we optimize it? – How long does it take? (Carlson/Buman; ACTIVE) – Are we talking about skilled performance? Or subjective outcomes? How do we train for particular outcomes, rather than particular underlying functions? How do we customize for individual differences? What is the role of/for retest? How much do we extend dosages? As we extend dosages and make interventions more customized and embedded in everyday life, how do we grapple with adherence? What is the optimal recipe for “combining”?
 – Are we talking about skilled performance. Or subjective outcomes. How do we train for particular outcomes, rather than particular underlying functions. How do we customize for individual differences. What is the role of/for retest. How much do we extend dosages. As we extend dosages and make interventions more customized and embedded in everyday life, how do we grapple with adherence. What is the optimal recipe for combining .")
59
Rebok

60
To these I’d add… Working less in a “cognitive” model and more in an applied or clinical model: Working backward for outcome measures, training for transfer, direct instruction Working on the compliance/adherence issues in parallel with the dosage increase issues Doing better work on dose-response and on multi-component interventions: – In particular, are we ready to begin to pilot tailored interventions – Requires different kinds of design

61
To these I’d add… Physical therapy uses a different toolkit for prevention/prehabilitation and rehabilitation, and they are clear on how these differ Physical therapy knows precise, targeted exercises, therapies (heat/cold, massage) for particular problems This implies an underlying taxonomy of which exercises affect which muscles / tendons / ligaments, and which in turn affect particular functions. – It is here that basic science is needed on the cognitive side

Similar presentations






















 De Anza College 14 April 2011.>")

>")
