Download presentation
Presentation is loading. Please wait.

1
Blood Instructor: DU Jing Office: 0850 physiological sciences Email: dujing771028@163.com Jining medical college Department of Physiology

2
TestUses Complete blood count (CBC), which includes: white blood cell count (WBC), red blood cell count (RBC), platelet count; hematocrit red blood cell volume (HCT); hemoglobin concentration (HB) ; differential WBC count ; ??? Clotting time (CT) Common hematology tests: Some common hematology tests include the following:
 Common hematology tests: Some common hematology tests include the following:.")
3
Lecture map Body fluid & plasma Physiology of blood cells -- Erythrocytes -- Leukocytes -- Platelets Physiology of hemostasis -- Formation of a platele plug -- Clot formation -- Anticlotting systems -- The fibrinolotic system -- Anticlotting drugs blood types

4
Blood Volume: Blood Volume: 7%~8% of body weight (e.g. 70kg — 5.5L)
")
5
1. Distribution & Transport O 2, CO 2, nutrients, hormones, wastes 2. Regulation (maintenance of homeostasis) pH (by buffers in blood), temperature 3. Protection "seal" vessel damage (platelets form plug), protection from infections (WBCs) Major Functions of Blood
 pH (by buffers in blood), temperature 3. Protection seal vessel damage (platelets form plug), protection from infections (WBCs) Major Functions of Blood.")
6
bright red (oxygenated), dark red/purplish (unoxygenated) much more dense than pure water pH range from 7.35 to 7.45 (slightly alkaline) slightly warmer than body temperature; typically 7%~8% of body weight Characteristics of Blood Blood is the only fluid tissue in the body.
, dark red/purplish (unoxygenated) much more dense than pure water pH range from 7.35 to 7.45 (slightly alkaline) slightly warmer than body temperature; typically 7%~8% of body weight Characteristics of Blood Blood is the only fluid tissue in the body.")
7
Relationship between the volume of body fluid & plasma (The values shown are calculated for a 70 kg man).
.")
8
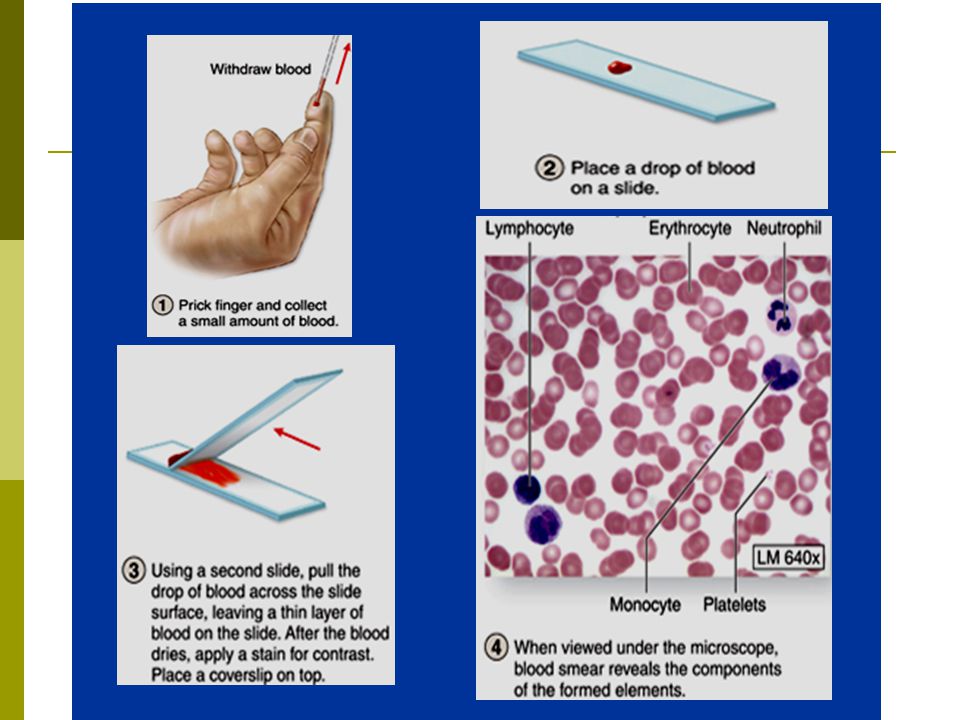
Hematocrit: the percentage of blood volume occupied by erythrocytes. (M: 45% ; F: 42%) It reflects the relative consistency of RBCs. Blood is defined as a mixture of cellar components suspended in a fluid called plasma. Plasma (55% ) Formed elements Leukocyctes and platelets (<1% ) Erythrocytes (45% ) Withdraw blood and place in tube 1 2 Centrifuge (3000r/min for 30’)
 It reflects the relative consistency of RBCs. Blood is defined as a mixture of cellar components suspended in a fluid called plasma. Plasma (55% ) Formed elements Leukocyctes and platelets (<1% ) Erythrocytes (45% ) Withdraw blood and place in tube 1 2 Centrifuge (3000r/min for 30’).")
9
Components of Blood

10
Plasma Plasma Water(92%) — the solvent in plasma Water(92%) — the solvent in plasma Proteins(7%) --- solutes, exert plasma osmotic pressure Proteins(7%) --- solutes, exert plasma osmotic pressure Albumins(4.2g/100ml) Albumins(4.2g/100ml) Glubulins(2.8g/100ml) Glubulins(2.8g/100ml) Fibrinogen(0.3g/100ml) Fibrinogen(0.3g/100ml) Other solutes(1%) Other solutes(1%) Electrolytes Electrolytes Nutrients Nutrients Respiratory gases Respiratory gases Waste products Waste products osmotic pressure, transporting, clotting factors, enzymes, Antibodies, hormones A/G = (1.5~2.5):1 A/G↓-- liver dysfunction founctions in clotting higher molar concentration e.g.Na +, K + -- membrane excitability Ca 2 + -- clotitng factor H +, HCO3 - -- maintaining PH
 — the solvent in plasma Water(92%) — the solvent in plasma Proteins(7%) --- solutes, exert plasma osmotic pressure Proteins(7%) --- solutes, exert plasma osmotic pressure Albumins(4.2g/100ml) Albumins(4.2g/100ml) Glubulins(2.8g/100ml) Glubulins(2.8g/100ml) Fibrinogen(0.3g/100ml) Fibrinogen(0.3g/100ml) Other solutes(1%) Other solutes(1%) Electrolytes Electrolytes Nutrients Nutrients Respiratory gases Respiratory gases Waste products Waste products osmotic pressure, transporting, clotting factors, enzymes, Antibodies, hormones A/G = (1.5~2.5):1 A/G↓-- liver dysfunction founctions in clotting higher molar concentration e.g.Na +, K + -- membrane excitability Ca clotitng factor H +, HCO maintaining PH")
11
Plasma versus Serum Both are fluid components of the blood. Both are fluid components of the blood. Plasma is the liquid portion of the blood that is separated from the blood cells by centrifugation. Plasma is the liquid portion of the blood that is separated from the blood cells by centrifugation. Serum is the leftover fluid that presents 1~2h after blood clotting. Serum is the leftover fluid that presents 1~2h after blood clotting. Serum does not contain the components in plasma necessary for the clotting reaction (such as fibrinogens and many clotting factors). Serum does not contain the components in plasma necessary for the clotting reaction (such as fibrinogens and many clotting factors). Plasma “yields” serum after clotting.
. Serum does not contain the components in plasma necessary for the clotting reaction (such as fibrinogens and many clotting factors). Plasma yields serum after clotting..")
12
Lecture map Body fluid & plasma Physiology of blood cells -- Erythrocytes -- Leukocytes -- Platelets Physiology of hemostasis -- Formation of a platele plug -- Clot formation -- Anticlotting systems -- The fibrinolotic system -- Anticlotting drugs blood types

14
Blood cells

15
Erythrocytes (red blood cells; RBCs) Count: M -- 5.1~5.8millon/mm 3 ; F -- 4.3~5.2millon/mm 3 (most abbundent blood cells) Structural characteristics: biconcave disk shape:high surface-to-volume ratio --- ideal for gas exchange; allows easy shape change. mature cells --- no nucleus; no mitochondria (only anaerobic metabolism) contains specific polysaccharides and proteins on the membrane mainly a hemoglobin carrier: hemoglobin --- carries >98% of O 2
 contains specific polysaccharides and proteins on the membrane mainly a hemoglobin carrier: hemoglobin --- carries >98% of O 2.")
16
Fe

17
Erythrocytes Function: Transporting oxygen & carbon dioxide. >98% O 2 is combined with hemoglobin; CO 2 in forms of bicarbonate(88%) and carbamino hemoglobin(7%) ※ ※ normal hemoglobin levels (g/l00 ml blood) --- infants 14-20 --- adult female 12-16 --- adult male 13-18 Useful in clinical diagnosing
 and carbamino hemoglobin(7%) ※ ※ normal hemoglobin levels (g/l00 ml blood) --- infants adult female adult male Useful in clinical diagnosing.")
18
Hematopoiesis – blood cell formation Hematopoiesis occurs in the red bone marrow of the: axial skeleton and girdles heads of the humerus and femur Hematopoietic stem cells can give rise to precursors of any of the different blood cells Erythrocytes Production of Erythrocytes

19
Erythrocytes Production of Erythrocytes in the bone marrow enter blood circulation Precursor cells

20
Normally stay in the bone marrow; Many reticulocytes found in blood --- presence of unusually rapid erythrocytes production. ※ Reticulocytes -- Young erythrocytes still containing a few ribosomes.

21
Erythrocytes Destruction of Erythrocytes The life span of an erythrocyte is about 120 days. About 0.8% of old RBCs are destructed everyday. Destruction normally occurs in the spleen and the liver. 90% of dying erythrocytes are engulfed by macrophages. Old erythrocytes become rigid and fragile, and their hemoglobin begins to degenerate. Iron is salvaged for reuse. Major breakdown production – bilirubin, gives plasma yellowish color. Some of proteins are broken down into amino acid to make new RBCs.

22
Fate of Erythrocytes

23
Erythrocytes Materials Required in Erythropoiesis Proteins, lipids, and carbohydrates Iron – essential for synthesizing the hemoglobin Small amount of iron is lost from the body. The body has considerable store of iron mainly in the liver, bound up with ferritin. Iron from old RBCs is bound to transferrin and dilivered to the bone marrow to make new RBCs. Iron deficiency → inadequate Hg production → iron deficiency anemia. Folic acid and Vitamin B 12 – auxiliary factors for formation of DNA. Folic acid – essential for normal cell division;

24
Erythrocytes Vitamin B 12 – required for the action of folic acid. Absorption of VB 12 from the gastrointestinal tract requires intrinsic factor secreted by the stomach. Lack of intrinsic factor→VB 12 deficiency → RBC deficiency → pernicious anemia. e.g. patients after stomach resection (surgical therapy for stomach cancer ) usually have anemia Materials Required in Erythropoiesis
 usually have anemia Materials Required in Erythropoiesis.")
25
Erythrocytes Regulation of Erythrocyte Production Circulating erythrocytes – the number remains constant and reflects a balance between RBC production and destruction Too few red blood cells leads to tissue hypoxia Too many red blood cells causes undesirable blood viscosity Erythropoiesis is hormonally controlled and depends on adequate supplies of iron, amino acids, and Vit B. esp. EPO

26
Hormonal Control of Erythropoiesis Erythropoietin (EPO) released by the kidneys is triggered by: A decreased oxygen delivery to the kidneys Insufficient pumping of blood by the heart Lung disease Anemia Exposure to high altitude Enhanced erythropoiesis increases the: RBC count in circulating blood Oxygen carrying ability of the blood
 released by the kidneys is triggered by: A decreased oxygen delivery to the kidneys Insufficient pumping of blood by the heart Lung disease Anemia Exposure to high altitude Enhanced erythropoiesis increases the: RBC count in circulating blood Oxygen carrying ability of the blood")
27
Reduces O 2 levels in blood Erythropoietin stimulates red bone marrow Enhanced erythropoiesis increases RBC count Normal blood oxygen levels Insufficient pumping of blood by the heart; Lung disease; Anemia; Exposure to high altitude Kidney (and liver to a smaller extent) releases erythropoietin Increases O 2 -carrying ability of blood Decrease O2 delivery to the kidneys Hormonal Control of Erythropoiesis by EPO
 releases erythropoietin Increases O 2 -carrying ability of blood Decrease O2 delivery to the kidneys Hormonal Control of Erythropoiesis by EPO")
28
Erythrocytes Erythrocyte Disorders Anemia -- blood has abnormally low oxygen- carrying capacity. a symptom rather than a special disease Blood oxygen levels cannot support normal metabolism. It is due to: -- total RBCs ↓ -- concentration of Hb ↓ -- combination of both Signs/symptoms include fatigue, paleness, shortness of breath, and chills

29
Major Causes of Anemia Dietary deficiencies of iron,Vit-B 12, or folic acid Bone marrow failure due to toxic drugs or cancer Blood loss from body (hemorrhage) → iron deficiency Inadequate secretion of EPO in kidney disease Excessive destruction of erythrocyte (e.g. sickle-cell anemia--an inherited blood disorder )
.")
30
Several Normal Erythrocytes and Several “Sickle” Erythrocytes

31
Polycythemia– too many RBCs in blood an adaptive response that occurs in high- altitude dwellers. excessive RBCs that increase blood viscosity. Erythrocyte Disorders

32
Leukocytes (White blood cells,WBCs) The only complete cells in blood Less numerous than RBCs, make up 1% of blood volume Can leave capillaries via diapedesis Can move through tissue spaces to the infective area and phagocytize bacterial microorganism Characteristics Function Fight infections --bacterial, viral, fungal, and parasitic infections Leukocytosis (increase of WBCs over 11,000/mm 3) --- general response to bacterial or viral invasion Classes & Count Normal count of total WBCs is 4000~11,000/mm 3
 The only complete cells in blood Less numerous than RBCs, make up 1% of blood volume Can leave capillaries via diapedesis Can move through tissue spaces to the infective area and phagocytize bacterial microorganism Characteristics Function Fight infections --bacterial, viral, fungal, and parasitic infections Leukocytosis (increase of WBCs over 11,000/mm 3) --- general response to bacterial or viral invasion Classes & Count Normal count of total WBCs is 4000~11,000/mm 3")
33
Leukocytes (WBCs) Granulocytes Granulocytes – neutrophils, eosinophils, and basophils Contain cytoplasmic granules that can be stained specifically with Wright’s stain, Are larger and usually shorter-lived than RBCs, Have multilobed nuclei and aboundant granules, Are all phagocytic cells.
 Granulocytes Granulocytes – neutrophils, eosinophils, and basophils Contain cytoplasmic granules that can be stained specifically with Wright’s stain, Are larger and usually shorter-lived than RBCs, Have multilobed nuclei and aboundant granules, Are all phagocytic cells.")
34
Leukocytes (WBCs) Granulocytes --- Neutrophils Account for 50%~70% of WBCs Neutrophils have two types of granules that: Take up both acidic and basic dyes Give the cytoplasm a purple color Neutrophils are our body’s bacteria “slayers” Attracted by chemokines (e.g. bacteria, toxin, Ag-Ab) ; Reache the focus of infection by diapedesis, phagocytize bacteria (phagocytosis) and digest them; Infection/inflammation – neutrophils >70%
 ; Reache the focus of infection by diapedesis, phagocytize bacteria (phagocytosis) and digest them; Infection/inflammation – neutrophils >70%.")
35
Bacteria (indicated by the red arrows ) are phagocytozed into the cytoplasma of a neutrophil
 are phagocytozed into the cytoplasma of a neutrophil")
36
Leukocytes (WBCs) Granulocytes --- Eosinophils Account for 1– 4% of WBCs Have red-staining granules and bilobate nuclei connected via a broad band of nuclear material Lead the body’s counterattack against parasitic worms Lessen allergies by phagocytizing immune complexes Infected by parasitic worms or in allergic reaction -- eosinophils >4%
 Granulocytes --- Eosinophils Account for 1– 4% of WBCs Have red-staining granules and bilobate nuclei connected via a broad band of nuclear material Lead the body’s counterattack against parasitic worms Lessen allergies by phagocytizing immune complexes Infected by parasitic worms or in allergic reaction -- eosinophils >4%")
37
Account for 0.5% of WBCs Have blue-staining granules and U- or S-shaped nuclei with two or three conspicuous constrictions Play a role in acute allergic reactions. Release histamine, heparin and other substances --- cause increased vascular permeability, smooth muscle spasm, vasodilation, that give the clinical symptoms of an allergic reaction: watery eyes, runny nose, and difficult breathing. Enhance the migration of leukocytes to the inflamed sites Leukocytes (WBCs) Granulocytes --- Basophils
 Granulocytes --- Basophils.")
38
Leukocytes (WBCs) Agranulocytes Agranulocytes – lymphocytes and monocytes: Lack visible cytoplasmic granules Are structurally similar, but functionally distinct Have oval (lymphocytes) or kidney-shaped (monocytes) nuclei
 Agranulocytes Agranulocytes – lymphocytes and monocytes: Lack visible cytoplasmic granules Are structurally similar, but functionally distinct Have oval (lymphocytes) or kidney-shaped (monocytes) nuclei")
39
Leukocytes (WBCs) Agranulocytes --- Monocytes Monocytes account for 2 – 8% of leukocytes The largest leukocytes Have abundant pale-blue cytoplasms Have purple-staining, U- or kidney-shaped nuclei Stay in circulation for 2~3days, enter tissue, and differentiate into macrophages (mature cells) Swallow more and bigger bacteria than neutrophils do, but migrant slower than neutrophils Activate lymphocytes to mount an immune response
 Agranulocytes --- Monocytes Monocytes account for 2 – 8% of leukocytes The largest leukocytes Have abundant pale-blue cytoplasms Have purple-staining, U- or kidney-shaped nuclei Stay in circulation for 2~3days, enter tissue, and differentiate into macrophages (mature cells) Swallow more and bigger bacteria than neutrophils do, but migrant slower than neutrophils Activate lymphocytes to mount an immune response")
40
Phagocytosis is an important part of the innate immune system. Both macrophages and neutrophils are capable of phagocytizing. Neutrophils is the main phgocytotic blood cells and number of neutrophils usually increases during the early period of inflammation. Macrophages occurs later. When the number of neutrophils in blood decreases to 1,000/mm 3, the ability of preventing infection obviously declines.

41
Leukocytes (WBCs) Agranulocytes --- Lymphocytes Account for 20~40% of WBCs and: Have large, dark-purple, circular nuclei with a thin rim of blue cytoplasm Are found mostly enmeshed in lymphoid tissue (some circulate in the blood) There are two types of lymphocytes: T cells and B cells T cells function in the immune response B cells give rise to plasma cells, which produce antibodies
 Agranulocytes --- Lymphocytes Account for 20~40% of WBCs and: Have large, dark-purple, circular nuclei with a thin rim of blue cytoplasm Are found mostly enmeshed in lymphoid tissue (some circulate in the blood) There are two types of lymphocytes: T cells and B cells T cells function in the immune response B cells give rise to plasma cells, which produce antibodies")
42
Platelets Normal count is 150.000 ~ 400,000/mm 3 Platelets are fragments of megakaryocytes with a blue- staining outer region and a purple granular center Their granules contain serotonin, Ca 2+, enzymes, ADP, and platelet-derived growth factor (PDGF) Platelets function in the clotting mechanism by forming a temporary plug that helps seal tears in blood vessels
 Platelets function in the clotting mechanism by forming a temporary plug that helps seal tears in blood vessels")
43
4,000 ~11,000 50 ~ 70% 1% ~ 4%

44
0 ~ 1% 20% ~ 40% 2% ~ 8%

45
Lecture map Body fluid & plasma Physiology of blood cells -- Erythrocytes -- Leukocytes -- Platelets Physiology of hemostasis -- Formation of a platele plug -- Clot formation -- Anticlotting systems -- The fibrinolotic system blood types

46
Physiological Hemostasis -- A series of reactions designed for stoppage of bleeding. -- Most effective in small vessels Raising the bleeding part above the heart – stop hemorrhage in a vein. Bleeding from a medium or large artery is not controlled by the body (Shock, MSOF). Accumulation of blood in the tissue – hematoma. Physiological Hemostasis
. Accumulation of blood in the tissue – hematoma. Physiological Hemostasis.")
47
Three Phases of hemostasis 1. vascular spasms (vasoconstriction at injured site) 2. platelet plug formation (plugging the hole) 3. coagulation (blood clotting - complex mechanism) Physiological Hemostasis They are interdependent and occur in rapid succession. Platelets are involved in both of the late two stages.
 3. coagulation (blood clotting - complex mechanism) Physiological Hemostasis They are interdependent and occur in rapid succession. Platelets are involved in both of the late two stages..")
48
Physiological Hemostasis Vascular Spasms Vasoconstriction (sudden tightening)-- first response to vascular injury is stimulated by: a. compression of vessel by escaping blood b. injury "chemicals" released by injured cells (serotonin, thromboxane A 2 ) c. reflexes from nocent stimulus in the vessel Slow the the flow of blood Constriction presses the opposed endothelial surfaces of vessels together Only short-lived response
 c. reflexes from nocent stimulus in the vessel Slow the the flow of blood Constriction presses the opposed endothelial surfaces of vessels together Only short-lived response.")
49
Physiological Hemostasis Formation of a plate plug begins within 15 seconds after injury Formation of A platelet Plug Normally---platelets do not stick to the collagen because the intact endothelial lining covers the inside wall of blood vessels.

50
Physiological Hemostasis Formation of A platelet Plug When a vessel is injured: Disrupts the endothelium and exposes the collagen. With the help of von Willebrand factor (VWF), platelets adhere to the collagen. Release serotonin and ADP — induce platelet activation; More platelets adhesion — platelet aggregation; TXA 2 further stimulates platelet aggregation and releasing of chemical agents; Fibrinogen forms bridges between aggregating platelets. The platelet plug is further enhanced by contraction of vascular smooth muscle.
, platelets adhere to the collagen. Release serotonin and ADP — induce platelet activation; More platelets adhesion — platelet aggregation; TXA 2 further stimulates platelet aggregation and releasing of chemical agents; Fibrinogen forms bridges between aggregating platelets. The platelet plug is further enhanced by contraction of vascular smooth muscle..")
53
Physiological Hemostasis Formation of A platelet Plug Why does the platelet plug not continuously expand in both directions? The platelet plug is limited to the area of the injury with the help of PGI 2 and NO!

54
Physiological Hemostasis Blood Coagulation The platelet plug is the rapid sealer of the break in the vessel wall: begins within 15 seconds after injury. The platelet plug is soften, temporary plug. Platelets are also essential for the following slower prosess of blood coagulation (clotting) that supports and reinforces the platelet plug.
 that supports and reinforces the platelet plug..")
55
Physiological Hemostasis Blood Coagulation Begins 30 seconds or more after the injury A set of reactions in which blood is transformed from a liquid to a gel — a clot (thrombus) consisting of fibrin. Coagulation may start with two different pathways: the intrinsic or the extrinsic pathway. The three phases of coagulation are: Prothrombin activator is formed (two pathways) Prothrombin is converted into thrombin Thrombin catalyzes the joining of fibrinogen into a fibrin mesh
 Prothrombin is converted into thrombin Thrombin catalyzes the joining of fibrinogen into a fibrin mesh.")
56
Blood Coagulation Brief description of clotting: Clotting is a cascade of chemical activation. At each step of the cascade, an inactive clotting factor (Page 76) is activated to a proteolytic enzyme, which then catalyzes the generation of the next enzyme in the sequence.
 is activated to a proteolytic enzyme, which then catalyzes the generation of the next enzyme in the sequence..")
57
reinforces platelet plug fibrinogen fibrin Prothrombin thrombin clot Active factor X Intrinsic pathwayExtrinsic pathway Ⅹ a binding with Ca2+, PF3, Ⅴ a Prothrombin activator(prothrombinase complex) Brief overview of clotting:
 Brief overview of clotting:")
58
Phase 1: Two Pathways to Prothrombin Activator May be initiated by either the intrinsic or extrinsic pathway Triggered by tissue-damaging events Involves a series of procoagulants Each pathway cascades toward factor X Once factor X has been activated, it binds with calcium ions, PF 3, and Va to form the complex-- prothrombin activator

59
The intrinsic & the extrinsic pathways. Genetic abaence of F Ⅷ causes hemophlia Genetic absence of F Ⅷ causes hemophilia

60
Phase 2: Prothrombin is converted to Thrombin Prothrombin activator catalyzes prothrombin into the active enzyme -- thrombin.

61
Phase 3: Jointing of Fibrinogen into Fibrin Mesh Thrombin catalyzes the polymerization of fibrinogen into fibrin Insoluble fibrin forms the structural basis of a clot Thrombin with the presence of calcium ions also activates factor XIII XIIIa stabilizes the fibrin network by catalyzing covalent crosslinkages

63
Clot Retraction and Repair A fibrin clot is a temporary device until permanent repair of the vessel occurs. Clot retraction – stabilization of the clot by squeezing serum from the fibrin strands Repair Platelet-derived growth factor (PDGF) stimulates rebuilding of blood vessel wall Fibroblasts form a connective tissue patch Stimulated by vascular endothelial growth factor (VEGF), endothelial cells multiply and restore the endothelial lining Connective tissue cells which secrete an extracellular matrix rich in collagen and other macromolecules.
 stimulates rebuilding of blood vessel wall Fibroblasts form a connective tissue patch Stimulated by vascular endothelial growth factor (VEGF), endothelial cells multiply and restore the endothelial lining Connective tissue cells which secrete an extracellular matrix rich in collagen and other macromolecules..")
64
The Liver Plays Important Role in Clotting The site of production for many plasma clotting factors Produces bile salts — important for absorption of Vitamin K (required when the liver produces prothrombin and several clotting factors)
")
65
Platelets play important roles in clotting: Several cascade reactions take place on the surface of activated platelets. PF released by the activated platelets functions as a cofactor in the steps mediated by the bound clotting factors. Plasma Ca 2+ is required at various steps Fibrin is an essential component – finally, the plug is further reinforced by interweaving fibrin (blood cells are trapped in the fibrin meshwork). In fact, the two pathways can not be completely separated. Physiological Hemostasis
. In fact, the two pathways can not be completely separated. Physiological Hemostasis.")
66
When a plug forms to seal the break in the vessel, there must to be some mechanisms for limiting coagulation in order to keep blood flowing smoothly in the blood vessels. Besides the inhibitors of platelet aggregation, there are still other mechanisms for limiting clot formation and for dissolving a clot after it has formed: Anticlotting systems --- factors that oppose clot formation (to limit clot formation) The fibrinolytic system --- to dissolve a clot after it has formed
 The fibrinolytic system --- to dissolve a clot after it has formed.")
67
Anticlotting System 1. TFPI (secreted by endothelia cells) can bind to TF- Ⅶ a complexes and inhibits the ability of them to activate F Ⅹ. 2. Thrombin + thrombomodulin, → + protein C, → inactivate Ⅷ a and Ⅴ a. (thrombin has double effects on clotting ) 3. Antithrombin Ⅲ binds to heparin and inactivates thrombin and several other clotting factors. Factors that Oppose Clot Formation:
 can bind to TF- Ⅶ a complexes and inhibits the ability of them to activate F Ⅹ. 2. Thrombin + thrombomodulin, → + protein C, → inactivate Ⅷ a and Ⅴ a. (thrombin has double effects on clotting ) 3. Antithrombin Ⅲ binds to heparin and inactivates thrombin and several other clotting factors. Factors that Oppose Clot Formation:.")
68
The Fibrinolytic System The system includes plasminogen activators, plasminnogen and plasmin. The fibrinolytic system --- dissolves a clot after it is formed (dissolves fibrin in a clot).
..")
69
Process of fibrinolysis ( dissolution of fibrin) The fibrinolytic System
 The fibrinolytic System")
70
Analogous to the clotting system--- is cascade of chemical activation. At each step, an inactive protein is activated, then it catalyzes the generation of the next enzyme in the sequence. The Fibrinolytic System

71
In fact, the fibrinolytic system is as complicated as the clotting system. There are multiple plasminogen activators and pathways for generating them. There are also several inhibitors of plasminogen activators in the fibrinolytic system. The Fibrinolytic System

72
Lecture map Body fluid & plasma Physiology of blood cells -- Erythrocytes -- Leukocytes -- Platelets Physiology of hemostasis -- Formation of a platele plug -- Clot formation -- Anticlotting systems -- The fibrinolotic system blood types

73
RBC membranes have glycoprotein antigens on their external surfaces These antigens are: – – Compatible with antibodies in plasma of an individual – – Recognized as foreign if improperly transfused into another individual – – Promoters of agglutination and are referred to as agglutinogens (antibodies to them-- lectins) Presence or absence of these antigens is used to classify blood groups Human Blood Groups Human Blood Groups a conjugated protein in which the nonprotein group is a carbohydrate
 Presence or absence of these antigens is used to classify blood groups Human Blood Groups Human Blood Groups a conjugated protein in which the nonprotein group is a carbohydrate")
74
Humans have 30 varieties of naturally occurring RBC antigens (e.g. ABO, Rh, M, N, Dufy, Kell, and Lewis) The antigens of the ABO and Rh blood groups cause vigorous transfusion reactions when they are improperly transfused Blood groups can be used in Forensic Medcine (e.g. for paternity testing) Human Blood Groups Human Blood Groups
 The antigens of the ABO and Rh blood groups cause vigorous transfusion reactions when they are improperly transfused Blood groups can be used in Forensic Medcine (e.g. for paternity testing) Human Blood Groups Human Blood Groups.")
75
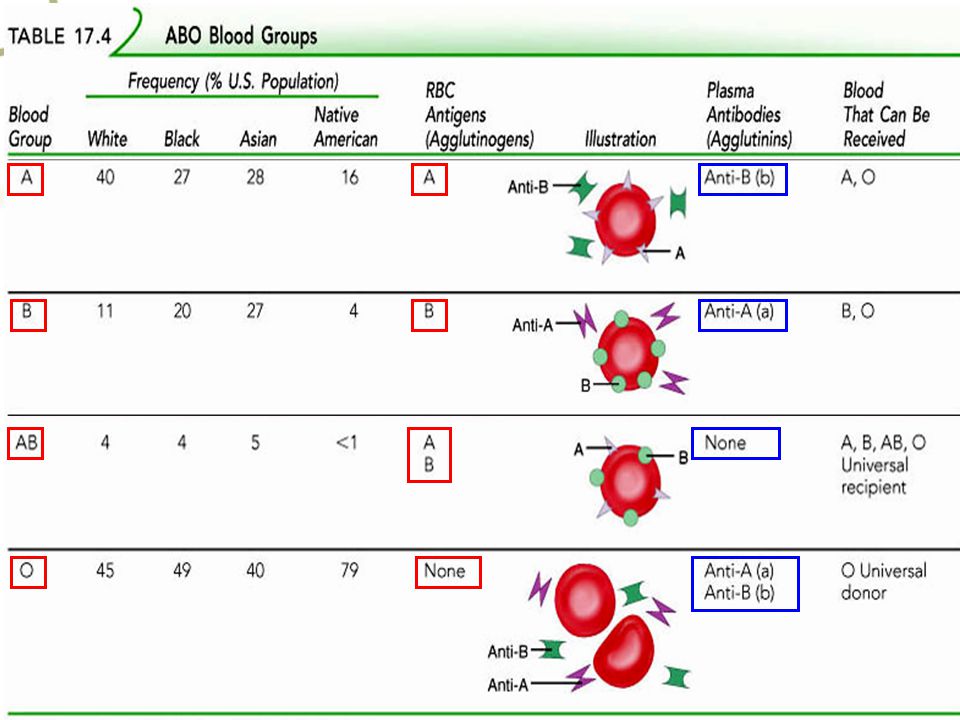
ABO Blood Groups Human Blood Groups Human Blood Groups determined by presence or absence of Type A and Type B agglutinogen proteins on cell membrane of RBCs. Agglutination reaction will occur if the antibodies in the plasma are incompatible with the antigens on the RBCs

77
According to presence or absence of the Rh antigens on RBCs --- Rh+ / Rh- Anti-Rh antibodies are not spontaneously formed in Rh – individuals. However, if an Rh – person receives Rh + blood, anti-Rh antibodies are formed. A second exposure to Rh + blood will result in a typical transfusion reaction in the Rh- person. (e.g. a Rh- person repeatedly receives Rh+ blood transfusion; a Rh- mother is again pregnant with Rh+ baby ) Rh Blood Groups Human Blood Groups Human Blood Groups
 Rh Blood Groups Human Blood Groups Human Blood Groups.")
78
Rh- mother is pregnant with Rh+ fetus for the first time Rh+ RBCs enter the maternal blood and induce Rh+ antibodies. The Rh- mother is pregnant again with Rh+ baby. The anti-Rh antibodies reach the fetus and result in erythroblastosis fetalis.

79
Basic Principles in Blood Transfusion Identify the blood types to ensure the donor’s ABO blood type is compatible with the recipient’s; and for pregnant women or patients needing blood transfusion repeatedly, Rh blood type must also be identified.

80
Cross-matching test must be done before blood transfusion: Basic Principles in Blood Transfusion No aggregation in both sides ---- blood transfusion may be done; Aggregation in the first side (regardless of the results in the secondary side) ---- blood transfusion mustn’t be done; No aggregation in the first side, but aggregation in the secondary side ---- small amount of blood transfusion can be done slowly, and condition of the recipient should be monitored carefully.
 ---- blood transfusion mustn’t be done; No aggregation in the first side, but aggregation in the secondary side ---- small amount of blood transfusion can be done slowly, and condition of the recipient should be monitored carefully.")
81
1. Distribution & Transport O 2, CO 2, nutrients, hormones, wastes 2. Regulation (maintenance of homeostasis) pH, temperature 3. Protection "seal" vessel damage, protection from foreign material & infections Major Functions of Blood
 pH, temperature 3. Protection seal vessel damage, protection from foreign material & infections Major Functions of Blood.")
82
Components of Blood Hematocrit: the percentage of blood volume occupied by erythrocytes. (M: 45% ; F: 42%) It reflects the relative consistency of RBCs.
 It reflects the relative consistency of RBCs..")
83
4,000 ~11,000 50 ~ 70% 1% ~ 4%

84
0 ~ 1% 20% ~ 40% 2% ~ 8%

85
Three Phases of hemostasis 1. vascular spasms (vasocontraction at injured site) 2. platelet plug formation (plugging the hole) 3. coagulation (blood clotting - complex mechanism) Physiological Hemostasis They are interdependent and occur in rapid succession. Platelets are involved in both of the late two stages.
 3. coagulation (blood clotting - complex mechanism) Physiological Hemostasis They are interdependent and occur in rapid succession. Platelets are involved in both of the late two stages..")
86
Physiological Hemostasis Begins within 15 seconds after injury Formation of A platelet Plug

88
Anticlotting System 1. TFPI (secreted by endothelia cells) can bind to TF- Ⅶ a complexes and inhibits the ability of them to activated F Ⅹ. 2. Thrombin inactivated Ⅷ a and Ⅴ a vie protein C. (thrombin has double effects on clotting ) 3. Antithrombin Ⅲ binds to heparin and inactivates thrombin and several other clotting factors. Factors that Oppose Clot Formation:
 can bind to TF- Ⅶ a complexes and inhibits the ability of them to activated F Ⅹ. 2. Thrombin inactivated Ⅷ a and Ⅴ a vie protein C. (thrombin has double effects on clotting ) 3. Antithrombin Ⅲ binds to heparin and inactivates thrombin and several other clotting factors. Factors that Oppose Clot Formation:.")
89
Process of fibrinolysis ( dissolution of fibrin) the fibrinolytic System
 the fibrinolytic System")
90
Tissue plasminogen activator (t-PA) is an important plasminogen activator in the body. Fibrin is not only the result of clotting, but also an important initiator of the fibrinolysis. Endothelial cells has several anticlotting functions ( summarized in Page 79 ).
..")
91
ABO Blood Groups Human Blood Groups Human Blood Groups determined by presence or absence of Type A and Type B agglutinogen proteins on cell membrane of RBCs. determined by presence or absence of Type A and Type B agglutinogen proteins on cell membrane of RBCs. Agglutination reaction will occur if the antibodies in the plasma are incompatible with the antigens on the RBCs Agglutination reaction will occur if the antibodies in the plasma are incompatible with the antigens on the RBCs

93
According to presence or absence of the Rh antigens on RBCs --- Rh+ / Rh- Anti-Rh antibodies are not spontaneously formed in Rh – individuals. However, if an Rh – person receives Rh + blood, anti-Rh antibodies are formed. A second exposure to Rh + blood will result in a typical transfusion reaction in the Rh- person. (e.g. a Rh- person repeatedly receives Rh+ blood transfusion; a Rh- mother is again pregnant with Rh+ baby ) Rh Blood Groups
 Rh Blood Groups.")
94
Basic Principles in Blood Transfusion Identify the blood types to ensure the donor’s ABO blood type is compatible with the recipient’s; and for pregnant women or patients needing blood transfusion repeatedly, Rh blood type must also be identified.

95
Cross-matching test must be done before blood transfusion: Basic Principles in Blood Transfusion No aggregation in both sides ---- blood transfusion may be done; Aggregation in the first side (regardless of the results in the secondary side) ---- blood transfusion mustn’t be done; No aggregation in the first side, but aggregation in the secondary side ---- small amount of blood transfusion can be done slowly, and condition of the recipient should be monitored carefully.
 ---- blood transfusion mustn’t be done; No aggregation in the first side, but aggregation in the secondary side ---- small amount of blood transfusion can be done slowly, and condition of the recipient should be monitored carefully.")
96
Know the following contents: the functions of blood production of red blood cells and its regulation destruction of red blood cells the conception of anemia, major causes Objectives

97
Know well the following contents: composition of blood normal count and the functions of different blood cells Rh blood type Objectives

98
Hold the following contents: the conception of hematocrit three phases of physiological hemostasis the process of platelet plug formation the process of clotting (the intrinsic and the extrinsic pathway) anticlotting systems the fibrinolytic system ABO blood groups basic principles in blood transfusion Objectives
 anticlotting systems the fibrinolytic system ABO blood groups basic principles in blood transfusion Objectives")
99
dujing771028@163.com

100
Leukocytes Functions of Leukocytes can squeeze through capillary walls(diapedesis or extravasation). can crawl into tissues and phagocytize bacteria

101
Leukocytes (White blood cells, WBCs) Classes of Leukocytes
 Classes of Leukocytes")
102
(50%~70%) (20%~40%) (2%~8%)
 (20%~40%) (2%~8%)")
103
Powerful phagocytosis founction of macrophages

104
How to stop bleeding

105
hematoma

107
Tissue plasminogen activator (t-PA) is an important plasminogen activator in the body. t-PA is secreted by endothelia cells. Binding to fibrin, t-PA catalyzes the generation of plasmin from plaminogen.

108
Fibrin is not only the result of clotting, but also an important initiator of the fibrinolysis.. Endothelial cells has several anticlotting functions ( summarized in Page 79 ) Inhibitors of plasminogen activators
 Inhibitors of plasminogen activators.")
109
RBC RBC Serum Serum DonorRecipient First side Secondary side

Similar presentations















 and plasma (the liquid in which the cells.>")


 RBCs WBCs Platelets color ? volume ?>")





