Download presentation
Presentation is loading. Please wait.

1
Anurag Goel ST5 Royal Preston Hospital.
Refeeding Syndrome Anurag Goel ST5 Royal Preston Hospital.

2
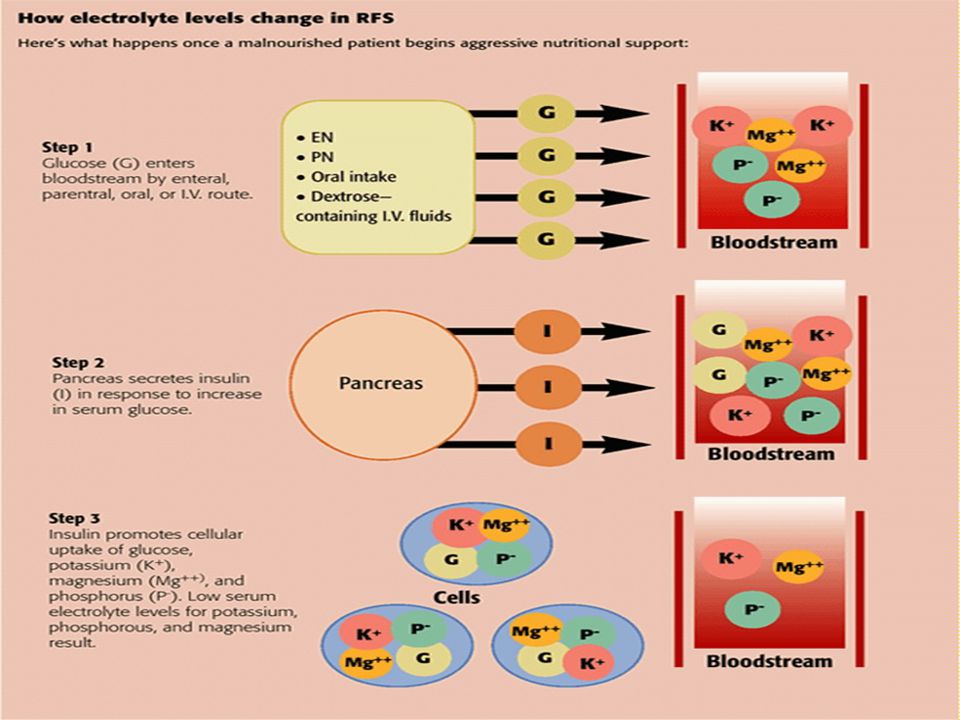
What is It? Potentially fatal shifts in fluids and electrolytes that may occur in malnourished patients receiving artificial refeeding (whether enterally or parenterally) The hallmark biochemical feature of re feeding syndrome is hypophosphataemia JPEN J Parenter Enteral Nutr 1990;14:90-7
 The hallmark biochemical feature of re feeding syndrome is hypophosphataemia. JPEN J Parenter Enteral Nutr 1990;14:90-7.")
3
Discovery of RFS Observed & described after WWII
Victims of starvation experienced cardiac and/or neurologic dysfunction After being reintroduced to food Neurologic signs & symptoms developed later

4
How common is RFS? True incidence is unknown
Study1 of 10,197 patients, incidence of hypophosphatemia = 43 % Malnutrition one of strongest risk factors Parenteral patients = 100% incidence of hypophosphatemia (if no PO4 in PN) ; 18% with PO4 containing PN2. 1. Mineral & Electrolyte Metabolism 1990;16:365-8 2. Nutr Hosp 2006;21:
 ; 18% with PO4 containing PN2. 1. Mineral & Electrolyte Metabolism 1990;16: Nutr Hosp 2006;21:")
5
Understanding Starvation
Glucose is normally the main fuel. Starvation - Shifts to protein & fat Insulin ↓ (due to ↓ availability of glucose) Catabolism of protein → loss of cellular & muscle mass → atrophy of vital organs & internal organs Respiratory & cardiac function ↓ due to muscular wasting & fluid/electrolyte imbalances Body is now surviving by slowly consuming itself
 Catabolism of protein → loss of cellular & muscle mass → atrophy of vital organs & internal organs. Respiratory & cardiac function ↓ due to muscular wasting & fluid/electrolyte imbalances. Body is now surviving by slowly consuming itself.")
6
Starvation The serum concentrations of electrolytes may appear normal in the starved state!! (Due to alterations in renal excretion rates of electroytes.)
")
8
Effects of Refeeding on the Cardiovascular System
Increases in heart rate, blood pressure, oxygen consumption, cardiac output expansion of plasma volume Response is dependent on amount of calories, protein and sodium given The malnourished heart can easily be given a metabolic demand that is too high for it to supply

9
Effects of Refeeding on the Cardiovascular System
Congestive Heart Failure is a common complication of refeeding Cardiac output can’t increase enough to meet the needs from the increased plasma volume, increased oxygen consumption and increases in blood pressure and heart rate

10
Effects of Refeeding on the Respiratory System
Excess carbon dioxide production and increased oxygen consumption from giving too much glucose and overfeeding A person with malnutrition-induced respiratory muscle wasting can get short of breath Can’t sustain an increased ventilatory drive Pulmonary edema due to increased water load

11
Effects of Refeeding on the Gastrointestinal System
Activity of the brush border enzymes and pancreatic enzyme secretion return to normal with refeeding Requires a period of readaptation to food to minimize GI complaints Diarrhea, nausea and vomiting

12
Main Pathophysiologic Features
Disturbances of body-fluid distribution Abnormal glucose & lipid metabolisms Thiamine deficiency Hypophosphatemia Hypomagnesemia Hypokalemia

13
Hypophosphatemia Phosphorus is predominantly intracellular
Impaired cellular-energy pathways Adenosine triphosphate (ATP) 2,3-diphosphoglycerate (2,3 DPG) Impaired skeletal-muscle function Including weakness & myopathy Seizures & perturbed mental state Impaired blood clotting processes & hemolysis also can occur
 2,3-diphosphoglycerate (2,3 DPG) Impaired skeletal-muscle function. Including weakness & myopathy. Seizures & perturbed mental state. Impaired blood clotting processes & hemolysis also can occur.")
14
Hypomagnesemia cofactor in most enzyme systems, including oxidative phosphorylation and ATP production. also necessary for the structural integrity of DNA, RNA, and ribosomes. Mild cases: often asymptomatic Severe cases: Cardiac arrhythmias Abdominal discomfort Anorexia Tremors, seizures, & confusion Weakness

15
Hypokalemia major intracellular cation. Serum levels may remain normal in starvation! Features: Cardiac arrhythmias Hypotension Cardiac arrest Weakness Paralysis Confusion Respiratory Depression

16
Thiamin Deficiency Functions as a cofactor in intermediary carbohydrate metabolism (TCA cycle) Amount needed depends on carbohydrate ingested. Mental confusion, ataxia, muscle weakness, edema, muscle wasting, tachycardia and cardiomegaly Wernicke’s encephalopathy can be precipitated by carbohydrate feeding in thiamine-deficient patients

18
Who is at risk? Some risk:
People who have eaten little or nothing for more than 5 days REMEMBER: Even an overweight or obese patient can be malnourished & a victim for RFS NICE guidelines (2006)
")
19
Who is at risk? High Risk Either patient has 1 or more:
BMI <16 Unintentional weight loss >15% in past 3-6 mo Little/no nutritional intake for 10 days Low levels of potassium, phosphate, or magnesium before feeding Or patient has 2 or more: BMI <18.5 Unintentional weight loss >10% in past 3-6 mo Little/no nutritional intake for >5 days History of alcohol misuse or drugs NICE guidelines (2006)
")
20
Patients at high risk: Anorexia nervosa Chronic alcoholism
Oncology patients Postoperative patients Elderly Uncontrolled diabetes mellitus GI fistulas Chronic malnutrition: Marasmus Prolonged fasting or low energy diet Morbid obesity with weight loss Long term antacid users Long term diuretic users

21
Managing refeeding syndrome
Identifying patients who are at risk. Prevent Refeeding syndrome. Once refeeding starts: Replace K, PO4, Mg even if normal (not if levels high) Potassium: 2-4 mmol/kg/day Phosphate: mmol/kg/day Magnesium: Oral 0.4 mmol/kg/d OR i.v. 0.2mmol/kg/d PS : Prefeeding replacement is not required even if electrolytes abnormal !!
 Potassium: 2-4 mmol/kg/day. Phosphate: mmol/kg/day. Magnesium: Oral 0.4 mmol/kg/d OR i.v. 0.2mmol/kg/d. PS : Prefeeding replacement is not required even if electrolytes abnormal !!")
22
Managing refeeding syndrome
Identifying patients who are at risk. Prevent Refeeding syndrome. Prefeeding replacement is not required if electrolytes abnormal Replace K, PO4, Mg even if normal (not if levels high) Potassium: 2-4 mmol/kg/day Phosphate: mmol/kg/day Magnesium: Oral 0.4 mmol/kg/d OR i.v. 0.2mmol/kg/d MANTAINANCE
 Potassium: 2-4 mmol/kg/day. Phosphate: mmol/kg/day. Magnesium: Oral 0.4 mmol/kg/d OR i.v. 0.2mmol/kg/d. MANTAINANCE.")
25
Managing refeeding syndrome
Feed cautiously – 10kcal/kg for first 2 days, 5kcal/kg in extreme cases Increase slowly (over 4 -7 days) No more than 150 to 200 gm of glucose gm of protein per kg actual bodyweight 20-30% of calories from fat PS: Weight Gain is NOT the goal in first 2 weeks. Thiamine (B1) is essential coenzyme in CHO metabolism. The symptoms of thiamine deficiency (Wernickes encephalopathy) can be precipitated by feeding with CHO in a vitamin B depleted patient
 No more than 150 to 200 gm of glucose gm of protein per kg actual bodyweight % of calories from fat. PS: Weight Gain is NOT the goal in first 2 weeks. Thiamine (B1) is essential coenzyme in CHO metabolism. The symptoms of thiamine deficiency (Wernickes encephalopathy) can be precipitated by feeding with CHO in a vitamin B depleted patient.")
26
Hypo-phosphataemia verses initial feed rate
Feed-rate kcal / kg

27
Managing refeeding syndrome
Pabrinex (high dose thiamine) and balanced multivitamin/mineral supplement ORAL: Thiamine 200 – 300 mgs + Vit B Co Strong 1-2 tabs TDS X 10 days IV: Pabrinex OD X 10 Days. first dose being administered at least 30 minutes before starting feeding. Thiamine (B1) is essential coenzyme in CHO metabolism. The symptoms of thiamine deficiency (Wernickes encephalopathy) can be precipitated by feeding with CHO in a vitamin B depleted patient
 and balanced multivitamin/mineral supplement. ORAL: Thiamine 200 – 300 mgs + Vit B Co Strong 1-2 tabs TDS X 10 days. IV: Pabrinex OD X 10 Days. first dose being administered at least 30 minutes before starting feeding. Thiamine (B1) is essential coenzyme in CHO metabolism. The symptoms of thiamine deficiency (Wernickes encephalopathy) can be precipitated by feeding with CHO in a vitamin B depleted patient.")
28
Electrolytes in Refeeding: phosphate
Oral One tablet = 16.1mmolPO4, 20.4mmol Na, 3.1mmol K) i.v. (phosphate polyfuser) 500ml = 50mmol PO4, 81mmol Na, 9.5mmol K+) Mild ↓ PO4 ( mmol/l) Phosphate Sandoz (16mmol each) - 2 tds 15mmol PO4 Polyfusor (150ml) over 12hrs peripherally Moderate ↓ PO4 ( mmol/l) Preferred route - i.v. 25mmol PO4 Polyfusor (250ml) over 12hrs peripherally Severe ↓ PO4 (<0.3 mmol/l) Not recommended 50mmol PO4 Polyfusor (500ml) over 24hrs peripherally, measuringPO4 at 12hrs.
 i.v. (phosphate polyfuser) 500ml = 50mmol PO4, 81mmol Na, 9.5mmol K+) Mild ↓ PO4 ( mmol/l) Phosphate Sandoz (16mmol each) - 2 tds. 15mmol PO4 Polyfusor (150ml) over 12hrs peripherally. Moderate. ↓ PO4 ( mmol/l) Preferred route - i.v. 25mmol PO4 Polyfusor (250ml) over 12hrs peripherally. Severe ↓ PO4 (<0.3 mmol/l) Not recommended. 50mmol PO4 Polyfusor (500ml) over 24hrs peripherally, measuringPO4 at 12hrs.")
29
Precautions Renal impairment – Half initial dose in significant renal impairment + monitor levels carefully Low calcium levels - Phosphate administration can cause hypocalcaemia Rapid IV infusion may cause metastatic soft tissue calcification CCF, hypertension : High sodium content of Phosphate-Sandoz® and Phosphates Polyfusor® Oral Mg, Ca or Al containing products – binds oral PO4 and prevent its absorption

30
Electrolytes in Refeeding: Potassium
Mantainance requirement 2-4 mmol/Kg/Day ORAL (not preferred) I.V. Mild ↓ K+ (3.0 – 3.5 mmol/l) Sando K (12mmol each) 1 tds OR Kay-Cee L 10 mls TDS (1mmol/ml) KCl 20mmol in 1000 mls normal saline or 5% dextrose over 8hrs. Moderate ↓ K+ ( 2.5 – 2.9 mmol / l) Sando K (12mmol each) 2 – 3 tds KCl 40mmol in 1000 mls normal saline or 5% dextrose over 8hrs. Severe ( <2.5 mmol / l) Sando K (12mmol each) 3 – 4 tds (However prefer i.v. replacement) KCl 40mmol in 1000 mls normal saline or 5% dextrose over 4 hrs. Retest before repeating Concentration must not exceed 40mmol/l peripherally. Maximum infusion rate is 20mmol/hr unless via a central line with ECG monitoring. CORRECT ↓ Mg+
 I.V. Mild ↓ K+ (3.0 – 3.5 mmol/l) Sando K (12mmol each) 1 tds OR. Kay-Cee L 10 mls TDS (1mmol/ml) KCl 20mmol in 1000 mls normal saline or 5% dextrose over 8hrs. Moderate. ↓ K+ ( 2.5 – 2.9 mmol / l) Sando K (12mmol each) 2 – 3 tds. KCl 40mmol in 1000 mls normal saline or 5% dextrose over 8hrs. Severe. ( <2.5 mmol / l) Sando K (12mmol each) 3 – 4 tds (However prefer i.v. replacement) KCl 40mmol in 1000 mls normal saline or 5% dextrose over 4 hrs. Retest before repeating. Concentration must not exceed 40mmol/l peripherally. Maximum infusion rate is 20mmol/hr unless via a central line with ECG monitoring. CORRECT ↓ Mg+")
31
Electrolytes in Refeeding: Magnesium
Maintenance requirement = 0.2 mmol/kg/day i.v. (or 0.4 mmol/kg/day orally ) Requirement i.v. oral Mild to moderate hypomagnesaemia ( mmol/l) Initially 0.5 mmol/kg/day over 24 hours iv, then 0.25 mmol/kg/day for 5 days i.v. 2 gms (8 mmol) MgSO4 in 100 mls N.S. Over 3 hrs. (1 gm MgSO4 = 4 mmol Mg+) -Magnesium Glycerophosphate 2 tds (4mmol/tab) -Magnaspartate 1 (6.5gm) sachet bd (10mmol/sachet) -Magnesium oxide (160mgs) 3.9 mmol per capsule 2 tds Severe hypomagnesaemia (<0.5 mmol/l) 24 mmol over 6 hours i.v. then as for mild to moderate ↓ Mg. 3 grams MgSO4 (12 mmol) in 100 mls N.S. Over 3 hrs. (x2 infusions) BMJ. Jun 28, 2008; 336(7659): 1495–1498
 Requirement. i.v. oral. Mild to moderate hypomagnesaemia ( mmol/l) Initially 0.5 mmol/kg/day over 24 hours iv, then 0.25 mmol/kg/day for 5 days i.v. 2 gms (8 mmol) MgSO4 in 100 mls N.S. Over 3 hrs. (1 gm MgSO4 = 4 mmol Mg+) -Magnesium Glycerophosphate 2 tds (4mmol/tab) -Magnaspartate 1 (6.5gm) sachet bd (10mmol/sachet) -Magnesium oxide (160mgs) 3.9 mmol per capsule 2 tds. Severe hypomagnesaemia (<0.5 mmol/l) 24 mmol over 6 hours i.v. then as for mild to moderate ↓ Mg. 3 grams MgSO4 (12 mmol) in 100 mls N.S. Over 3 hrs. (x2 infusions) BMJ. Jun 28, 2008; 336(7659): 1495–1498.")
32
Electrolytes in Refeeding : Calcium
10-20 mmol calcium ( 40-80ml of Calcium Gluconate 10%) in 500ml of Normal Saline 0.9% over 6-8 hours
 in 500ml of Normal Saline 0.9% over 6-8 hours.")
33
Electrolytes in Refeeding : Sodium
Sodium must be given carefully to prevent overexpansion of the extracellular fluid Upon refeeding, renal sodium losses stop Hence Sodium and water retention Restrict Sodium <1 mmol/Kg/day

34
Fluid in Refeeding Refeeding results in expansion of the extracellular space and fluid must be given carefully Aim for fluid replacement 20 – 30 mls/Kg/Day Weight gain greater than 1 kg the first week is due to fluid retention Fluid may need to be restricted to 800 to 1000 mls/day Increases in blood pressure, heart rate and respiratory rate may be early signs of fluid excess

35
Monitoring K+ - check daily. Once or twice weekly once stable.
Mg2+ and Po43- daily monitoring. Once weekly when stable. BMs 4 times a day – beware hyperglycaemia.

36
Priorities – Only one cannula!!
Aim to correct potassium Then bring magnesium and calcium to safe levels, not necessarily in the normal range Then bring phosphate levels up to a safe, not necessarily normal value This may need to be done in stages to allow for further calcium or magnesium infusions

37
Priorities – Only one cannula!!
Aim to correct potassium Then bring magnesium and calcium to safe levels, not necessarily in the normal range Then bring phosphate levels up to a safe, not necessarily normal value This may need to be done in stages to allow for further calcium or magnesium infusions. Can we mix the KCl with MgSO4 and or Cal Gluconate??

38
Summary Points Characterized by hypophosphatemia
Patients at high risk: undernourished, little or no energy intake for > 10 days Start refeeding at low levels Correction of electrolyte & fluid imbalances before feeding is not necessary (do not delay feeding)
")
39
Questions

Similar presentations











 Integumentary System (chapters 44- 46)>")









