Download presentation
Presentation is loading. Please wait.

1
EMT Review Basically everything you need to know without outwardly giving you all the answers

2
Legalities Scope of Practice Standard of Care Duty to Act Abandonment
Assault Battery 5150

3
Legalities Negligence Duty to Act Breach of Duty to Act
Proximate Cause Compensatable Injury

4
Legalities Consent Expressed Implied Minor/mentally incompetent

5
Patient Assessment Initial Assessment BSI/Safety Number of patients
MOI/NOI Additional resources Cspine

6
Patient Assessment General Impression AVPU Chief Complaint ABC

7
Respiratory Pulmonary Embolism Acute Pulmonary Edema COPD Asthma
Hyperventilation Pneumonia

8
Emphysema Characterized by the destruction of the alveolar walls and the distention of the alveolar sacs. Patients trap air and are unable to exhale.

9
Emphysema Thin, barrel chest appearance Cough, little sputum
Prolonged exhalation Diminished lung sounds with wheezes Pursed lip breathing Pink complexion (pink puffers) Home oxygen
 Home oxygen.")
10
Chronic Bronchitis Affects primarily the bronchus and the bronchioles.
Characterized by a productive cough that persists for at least 3 consecutive months 2 years in a row.

11
Chronic Bronchitis Typically overweight (blue bloaters)
Chronic cyanotic complexion Dyspnea, but not as bad as emphysema Coarse rhonchi Wheezes and crackles in lungs

12
Asthma A reactive airway disease that affects the bronchial tree and bronchioles An increased sensitivity of the lower airways to irritants and allergens

13
Asthma Bronchospasm Edema of the inner lining of the airways
Increased secretion of mucus that causes plugging of the smaller airways.

14
Pulmonary Embolism An obstruction of blood flow in the pulmonary arteries. Impedes the delivery of oxygenated blood back into the cardiovascular system. Can be caused by blood clots, fat particles, foreign body, or amniotic fluid.

15
Pulmonary Embolism Causes include: Sedentary lifestyle Recent surgery
Long bone fractures Smokers Birth control pills

16
Pulmonary Embolism Signs/Symptoms include:
Sudden onset pinpoint chest pain Shortness of breath Poor skin signs Possible diminished lung sounds

17
Acute Pulmonary Edema Excessive amounts of fluid collect in the spaces between the alveoli and the capillaries. Cardiogenic: increased pressure in the pulmonary veins push fluid out of the capillaries. Non cardiogenic: destruction of capillary beds causes fluid to leak out. (ARDS)
")
18
Acute Pulmonary Edema Signs/Symptoms include: Dyspnea and orthopnea
Frothy sputum Crackles in lungs Cyanosis, or pale wet skins JVD Swollen lower extremeties Hypertension

19
Acute Pulmonary Edema Oxygen via NRB or BVM Sit upright Dangle feet
Rapid transport

20
Hyperventilation Syndrome
Most often caused by anxiety or emotional distress. Can also be caused by: Methanphetamine OD Hyperglycemia ASA OD

21
Hyperventilation Syndrome
Signs/Symptoms include: Dizzy Shortness of breath Numbness/tingling to hands, feet, perioral Spasms of fingers and toes

22
Assessment of Newborn Appearance Pulse Grimace Activity Respiration

23
Appearance Trunk and extremities pink = 2 points
Trunk pink with blue extremities = 1 point Trunk and extremities blue = 0 points

24
Pulse Heart rate over 100 = 2 points Heart rate under 100 = 1 point
Heart rate absent = 0 points

25
Grimace AKA Reflex irritability Facial grimace plus cry = 2 points
Only facial grimace = 1 point No reflex activity = 0 points

26
Activity Active movement = 2 points
Some flexion w/o active movement = 1 point Limp = 0 points

27
Respiration Good respiration + strong cry = 2 points
Slow or irregular breathing = 1 point Apnea = 0 points

28
APGAR Scores 0-3 points = aggressive resuscitation (BVM, CPR, etc.)
4-6 points = Provide stimulation and O2 7-10 points = Provide routine care

29
Spontaneous Abortion AKA Miscarraige Can occur for many reasons
Viability usually considered after 20 weeks Check for severe lower abdominal pain, severe vaginal bleeding, passing of tissue or blood clots

30
Pre-Eclampsia Last trimester emergency, usually first pregnancy, with a history of hypertension or diabetes Characterized by high blood pressure and swelling of the extremities Seizures from pre-eclampsia is called Eclampsia

31
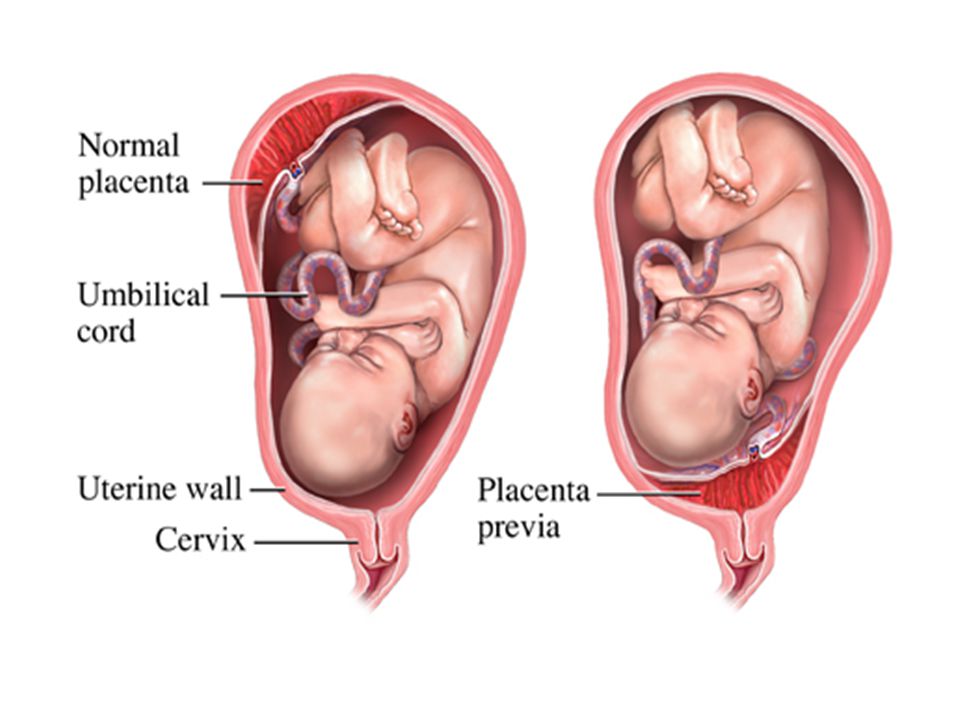
Placenta Previa The placenta attaches itself to the uterus over the cervix Fetus pushes on placenta, causing severe bleeding, but little or no pain

33
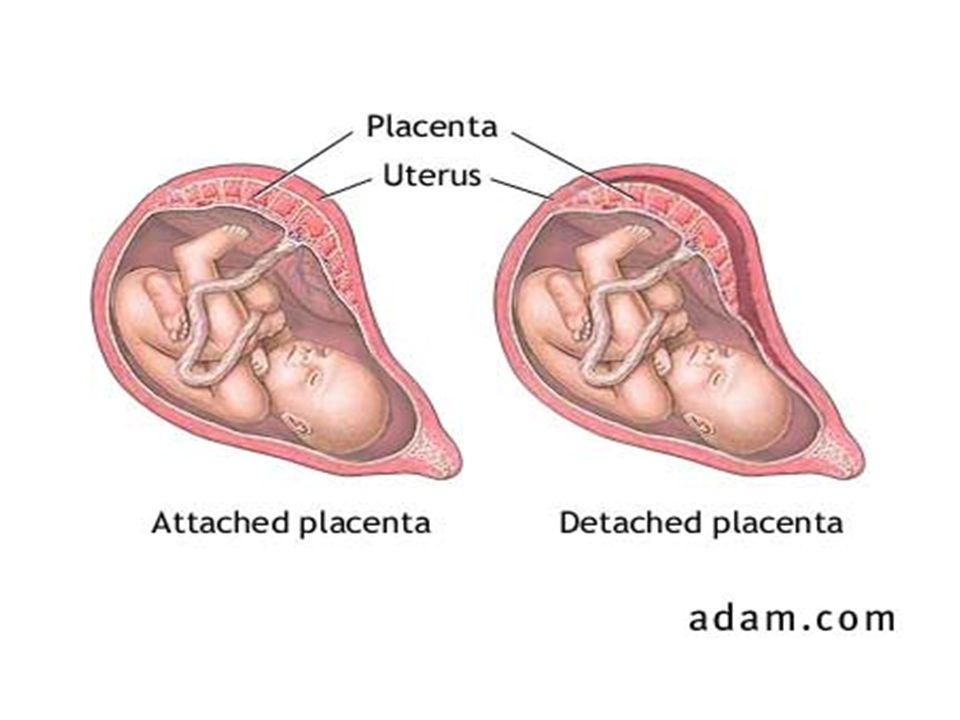
Abruptio Placentae When the placenta tears away from the uterine wall prematurely Causes fetal distress due to poor gas and nutrient exchange Severe abdominal pain, although little or no external bleeding may occur.

35
Ruptured Uterus As the uterus expands and thins out, especially around the cervix, can cause spontaneous or traumatic rupture. Usually more than 2 previous pregnancies, or history of C-section. Mothers mortality rate is 5-20%, Fetal mortality rate is 50%. Severe pain, minor vaginal bleeding.

36
Ectopic Pregnancy When the ovum is implanted outside the uterus.
90% fallopian tube 6% in peritoneum 1% in cervix

37
Acute Coronary Syndromes: Angina Pectoris
Literally “pain in chest” From a decrease of oxygen to the cardiac tissues (cardiac tissue ischemia) Normally from an increased workload on the heart Will feel a crushing or squeezing type pain radiating to the jaw, arm, or back Normally relieved with rest, O2, NTG
 Normally from an increased workload on the heart. Will feel a crushing or squeezing type pain radiating to the jaw, arm, or back. Normally relieved with rest, O2, NTG.")
38
Acute Coronary Syndrome: Myocardial Infarction
A portion of the heart muscle dies from the lack of an adequate supply of oxygenated blood. Usually from coronary artery disease. Heart muscle dies, leading to a build up of lactic acid, which causes the “pain.” Can cause irregular heart rhythms and sudden death.

39
Assessment of ACS (O)nset: Sudden or Gradual?
(P)rovocation: What caused the pain? (Q)uality: What does it feel like? (R)egion: Where does it hurt? (R)adiation: Does the pain travel? (R)eoccurance: Have you had before? (S)everity: Rate on 1-10 scale (T)ime: How long have you had pain?
rovocation: What caused the pain (Q)uality: What does it feel like (R)egion: Where does it hurt (R)adiation: Does the pain travel (R)eoccurance: Have you had before (S)everity: Rate on 1-10 scale. (T)ime: How long have you had pain")
40
Pertinent Negatives of ACS
Nausea Vomiting Diaphoresis Dizziness Weakness Syncope Palpitations Shortness of Breath

41
Acute Coronary Syndromes: Treatment
Rest. Do not make your patient move more than they have to. O2 15l/m NRB Nitroglycerin SL ASA

42
Nitroglycerin (NTG) Class: Nitrate
Action: Dilates Coronary Arteries allowing blood to oxygenate ischemic tissues. Dose: 1 on SO, to a max of 3 on BHO Side Effects: Headache, hypotension, tachycardia Contraindications: Use of sexual enhancing drugs in last 48 hours

43
Aspirin (ASA) Class: Platelet Aggregation Inhibitor
Action: Reduces the ability of the platelets to bind to eachother.

44
Heart Failure AKA “CHF”
Inability for one or both Ventricles to pump blood effectively Several Causes

45
Heart Failure Main Causes: AMI Hypertension Valve disorders
Pulmonary Embolism Drug use

46
Right Heart Failure Right ventricle accepts de-oxygenated blood and ejects it to the lungs for oxygenation. Fluid (blood) backs up in the venous system causing JVD, Liver enlargement, peripheral edema. Normally not an emergent condition.
 backs up in the venous system causing JVD, Liver enlargement, peripheral edema. Normally not an emergent condition.")
47
Left Heart Failure Left ventricle accepts oxygenated blood from the lungs, and ejects it out to the bodies arteries. Left ventricle cannot eject all its blood, which causes a build up of pressure. The pressure causes Pulmonary Edema Left Ventricular failure is an emergent condition

48
Signs of Heart Failure Severe Shortness of breath with crackles
Tachycardia and Tachypnea Orthopnea and PND Fatigue with little movement Pale, cool, sweaty skins Cyanosis Severe hypertension JVD

49
Treatment for Heart Failure
Sit patient upright and dangle legs O2 15l/m by NRB or BVM Positive Pressure Ventilation

50
Diabetes mellitus types
Type I—Insulin dependent diabetes mellitus Type II—Non-insulin dependent diabetes mellitus The two that you will most often find in the prehospital environment are Type I diabetes and Type II diabetes. Type I is also referred to as insulin-dependent diabetes mellitus (IDDM), since these patients are required to inject insulin to regulate their blood glucose levels. The Type I patient’s pancreas usually does not secrete any insulin. These patients are typically younger when the diabetes occurs, most commonly under the age of 40. The peak age for onset of Type I diabetes mellitus is 10 to 14 years. The patients are typically lean from weight loss. Their blood glucose levels are extremely high if untreated. These patients will suffer from the three Ps. Type I diabetics often have difficulty keeping their blood glucose level within the normal range, with the possibility of having too high or too low a blood glucose level. Therefore, they are prone to suffering from a hyperglycemic condition called diabetic ketoacidosis (DKA). They may also suffer from hypoglycemia (low blood glucose). Type I diabetes is less common. Type II diabetes is also referred to as non-insulin-dependant diabetes mellitus (NIDDM), because Type II patients usually do not have to inject insulin. However, they do have to regulate their diet and exercise and take oral drugs to help the pancreas secrete more insulin or to make the insulin that is secreted more effective in facilitating movement of glucose into the cells. Type II diabetic patients are usually middle-aged or older. They are typically overweight. Like Type I diabetics, they suffer from high blood glucose levels if untreated. Like Type I diabetics, they will also present with a history of suffering from the three Ps. These patients are prone to a hyperglycemic condition called hyperglycemic hyperosmolar nonketotic syndrome (HHNS).
, since these patients are required to inject insulin to regulate their blood glucose levels. The Type I patient’s pancreas usually does not secrete any insulin. These patients are typically younger when the diabetes occurs, most commonly under the age of 40. The peak age for onset of Type I diabetes mellitus is 10 to 14 years. The patients are typically lean from weight loss. Their blood glucose levels are extremely high if untreated. These patients will suffer from the three Ps. Type I diabetics often have difficulty keeping their blood glucose level within the normal range, with the possibility of having too high or too low a blood glucose level. Therefore, they are prone to suffering from a hyperglycemic condition called diabetic ketoacidosis (DKA). They may also suffer from hypoglycemia (low blood glucose). Type I diabetes is less common. Type II diabetes is also referred to as non-insulin-dependant diabetes mellitus (NIDDM), because Type II patients usually do not have to inject insulin. However, they do have to regulate their diet and exercise and take oral drugs to help the pancreas secrete more insulin or to make the insulin that is secreted more effective in facilitating movement of glucose into the cells. Type II diabetic patients are usually middle-aged or older. They are typically overweight. Like Type I diabetics, they suffer from high blood glucose levels if untreated. Like Type I diabetics, they will also present with a history of suffering from the three Ps. These patients are prone to a hyperglycemic condition called hyperglycemic hyperosmolar nonketotic syndrome (HHNS).")
51
Hypoglycemia Emergencies related to diabetes mellitus
More common with Type I diabetics Most dangerous complication of diabetes mellitus Most common cause of coma in the diabetic patient Hypoglycemia is a condition where a diabetic patient is suffering from a low blood glucose level (hypo = low, glyco = glucose, emia = blood). This condition is more common in Type I IDDM patients than in Type II NIDDM patients. Hypoglycemia is the most dangerous acute complication of diabetes mellitus. It is estimated that 9 to 120 episodes of hypoglycemia will occur per 100 diabetic patients per year. It is one of the most common causes of coma in the diabetic patient.
. This condition is more common in Type I IDDM patients than in Type II NIDDM patients. Hypoglycemia is the most dangerous acute complication of diabetes mellitus. It is estimated that 9 to 120 episodes of hypoglycemia will occur per 100 diabetic patients per year. It is one of the most common causes of coma in the diabetic patient.")
52
Causes/Signs & Symptoms Insulin Shock
Too much insulin Too little food Too much exercise or stress May be precipitated by increased ETOH without CHO intake Review findings consistent with diabetics.

53
Hyperglycemia Emergencies related to diabetes mellitus
Usually presents as either DKA or HHNS Both syndromes have elevated BGL in the body DKA usually > 350 mg/dl HHNS usually > 600 mg/dl Altered physiology leads to dehydration and acidosis Hyperglycemia is a condition where a diabetic patient is suffering from a high blood glucose level (hyper = high, glyco = glucose, emia = blood) There are two different conditions a patient may suffer from becoming extremely hyperglycemic: diabetic ketoacidosis (DKA) and hyperglycemic hyperosmolar nonketotic syndrome (HHNS). As noted earlier, DKA is more commonly seen in the Type I diabetic, whereas HHNS is more common in the Type II diabetic. In both conditions, the blood glucose level increases drastically. Unlike hypoglycemia, where there is a lack of glucose in the blood, in hyperglycemic conditions there is a lack of insulin and an excessive amount of glucose in the blood. In hyperglycemic conditions, the brain has more glucose than it knows what to do with.
 There are two different conditions a patient may suffer from becoming extremely hyperglycemic: diabetic ketoacidosis (DKA) and hyperglycemic hyperosmolar nonketotic syndrome (HHNS). As noted earlier, DKA is more commonly seen in the Type I diabetic, whereas HHNS is more common in the Type II diabetic. In both conditions, the blood glucose level increases drastically. Unlike hypoglycemia, where there is a lack of glucose in the blood, in hyperglycemic conditions there is a lack of insulin and an excessive amount of glucose in the blood. In hyperglycemic conditions, the brain has more glucose than it knows what to do with.")
54
Causes/Signs & Symptoms
Too little insulin Too much food Illness Infection

55
Transient Ischemic Attack (TIA)
A TIA looks just like a CVA symptomatically TIA disappears within 24 hours of onset, without any permanent neurological changes Usually, symptoms subside within 15–30 minutes Patients who experience transient ischemic attack (TIA) develop most of the same signs and symptoms as those who are experiencing a stroke. The key difference between a stroke and a TIA is that the signs and symptoms of a TIA disappear within typically ten to fifteen minutes, but almost always within one hour of the onset of the signs and symptoms. The TIA always resolves within 24 hours without causing any permanent neurologic disability. Ischemia, which refers to an oxygen deficit in the tissues, affects the brain and causes the stroke-like signs and symptoms to appear. Reversal of the ischemia leads to disappearance of the stroke-like signs and symptoms. Most commonly, the signs and symptoms of TIAs last less than 15 minutes. It is unusual for them to last longer than 30 minutes. Thus, the patient may present with typical signs and symptoms of a stroke, but they progressively disappear.
 develop most of the same signs and symptoms as those who are experiencing a stroke. The key difference between a stroke and a TIA is that the signs and symptoms of a TIA disappear within typically ten to fifteen minutes, but almost always within one hour of the onset of the signs and symptoms. The TIA always resolves within 24 hours without causing any permanent neurologic disability. Ischemia, which refers to an oxygen deficit in the tissues, affects the brain and causes the stroke-like signs and symptoms to appear. Reversal of the ischemia leads to disappearance of the stroke-like signs and symptoms. Most commonly, the signs and symptoms of TIAs last less than 15 minutes. It is unusual for them to last longer than 30 minutes. Thus, the patient may present with typical signs and symptoms of a stroke, but they progressively disappear.")
56
Cerebral Vascular Accident (CVA)
General signs and symptoms of a stroke or TIA Progressive worsening of symptoms as stroke evolves Review findings of an acute stroke.

57
Types of seizures Primary seizures Secondary seizures Seizure disorder
Insult to body Fever Infection Hypoxia Hypoglycemia Hyperglycemia Drug intoxication Drug withdrawal Eclampsia in pregnancy Degenerative brain diseases Imbalances in the electrolytes in the body Cardiac arrest Generally full body seizures Seizures are categorized as either primary seizures or secondary (reactive) seizures. Primary seizures in adults are usually due to a genetic or unknown cause. Primary seizures are categorized as generalized or partial seizures. The partial seizures are either simple or complex. Generalized seizures involve both hemispheres of the brain, which typically results in a loss of consciousness. The seizure activity is usually rhythmic, tonic-clonic muscle contractions (convulsions). Partial seizures are typically related to abnormal activity in one cerebral hemisphere. A patient who is suffering a simple partial seizure will remain conscious, whereas a complex partial seizure will normally produce an altered mental status or unresponsiveness. Secondary or reactive seizures do not result from a genetic cause but occur from an insult to the body, such as fever, infection, hypoxia, hypoglycemia, hyperglycemia, drug intoxication, drug withdrawal, eclampsia in pregnancy, degenerative brain diseases, and imbalances in the electrolytes in the body. As a rule of thumb, secondary or reactive seizures are generalized in nature and do not produce partial-type seizures. Thus, the patient suffering a seizure from some type of insult to the body will suffer a full convulsive-type seizure. The key with this type of seizure is to treat the underlying cause of the seizure activity. For example, if the seizure activity is due to hypoxia resulting from inadequate breathing, the most important emergency care you can provide that will stop the seizure and prevent it from recurring is to establish an airway and provide effective positive pressure ventilation with oxygen supplement. Reactive or secondary generalized seizures that are due to an insult to the body are extremely dangerous and can result in death if not treated promptly. These are totally different from those seizures that are primary, in which the patient has a diagnosed history of a seizure disorder.
 seizures. Primary seizures in adults are usually due to a genetic or unknown cause. Primary seizures are categorized as generalized or partial seizures. The partial seizures are either simple or complex. Generalized seizures involve both hemispheres of the brain, which typically results in a loss of consciousness. The seizure activity is usually rhythmic, tonic-clonic muscle contractions (convulsions). Partial seizures are typically related to abnormal activity in one cerebral hemisphere. A patient who is suffering a simple partial seizure will remain conscious, whereas a complex partial seizure will normally produce an altered mental status or unresponsiveness. Secondary or reactive seizures do not result from a genetic cause but occur from an insult to the body, such as fever, infection, hypoxia, hypoglycemia, hyperglycemia, drug intoxication, drug withdrawal, eclampsia in pregnancy, degenerative brain diseases, and imbalances in the electrolytes in the body. As a rule of thumb, secondary or reactive seizures are generalized in nature and do not produce partial-type seizures. Thus, the patient suffering a seizure from some type of insult to the body will suffer a full convulsive-type seizure. The key with this type of seizure is to treat the underlying cause of the seizure activity. For example, if the seizure activity is due to hypoxia resulting from inadequate breathing, the most important emergency care you can provide that will stop the seizure and prevent it from recurring is to establish an airway and provide effective positive pressure ventilation with oxygen supplement. Reactive or secondary generalized seizures that are due to an insult to the body are extremely dangerous and can result in death if not treated promptly. These are totally different from those seizures that are primary, in which the patient has a diagnosed history of a seizure disorder.")
58
Generalized tonic-clonic
Grand Mal What we most commonly think of Most self limiting Occurs in phases Aura Tonic phase Hypertonic phase Clonic phase Postictal phase Status Greater than 5 minutes Recurrent with no lucid interval The signs and symptoms and emergency care for the most common type of seizure, the generalized tonic-clonic seizure, or grand mal seizure, were discussed earlier, in the main part of this presentation.

59
Partial Seizures Simple partial seizure
Focal motor or Jacksonian seizure Patient is usually awake Results in an area of the body (face, arm, leg, or body) demonstrating the seizure-like motions May progress to grand mal seizure Complex partial seizure Psychomotor or temporal lobe seizure Due to the region of the brain involved with the seizure, the patient’s orientation may be altered Usually lasts 1-2 minutes, characterized by repetitive type motions Post-seizure confusion usually longer than seizure itself A simple partial seizure is also known as a focal motor seizure or Jacksonian motor seizure. This type of seizure generally produces jerky muscle activity in one area of the body, arm, leg, or face. The patient cannot control the jerky movement but remains awake and aware of the seizure activity. The seizure activity may spread from one area of the body to another, and sometimes progresses to a generalized tonic-clonic seizure. You should document where the seizure activity began and how it progressed. This information may be extremely helpful in identifying a cause and in the long-term treatment of the patient.
 demonstrating the seizure-like motions. May progress to grand mal seizure. Complex partial seizure. Psychomotor or temporal lobe seizure. Due to the region of the brain involved with the seizure, the patient’s orientation may be altered. Usually lasts 1-2 minutes, characterized by repetitive type motions. Post-seizure confusion usually longer than seizure itself. A simple partial seizure is also known as a focal motor seizure or Jacksonian motor seizure. This type of seizure generally produces jerky muscle activity in one area of the body, arm, leg, or face. The patient cannot control the jerky movement but remains awake and aware of the seizure activity. The seizure activity may spread from one area of the body to another, and sometimes progresses to a generalized tonic-clonic seizure. You should document where the seizure activity began and how it progressed. This information may be extremely helpful in identifying a cause and in the long-term treatment of the patient.")
60
Absence or petit mal seizure
Most common in children Characterized by a blank stare Rarely necessitates emergency care Absence or petit mal seizures, most common in children, are characterized by a blank stare, beginning and ending abruptly, and only lasting a few seconds. There may be rapid blinking, chewing, and lack of attention. The child is unaware of what is occurring during the seizure but then quickly returns to full awareness. No emergency care is necessary for the absence seizure. If this is a first time observation of the seizure, medical evaluation should be recommended.

61
Febrile seizure Common to kids 6 months to 6 years
Usually self limiting Due to rapid rise or fall of temperature Gentle cooling Febrile seizures, caused by high fever, are most common in children between 6 months and 6 years of age. About 5 percent of children who have a fever will develop febrile seizures. These secondary or reactive generalized seizures are often very short and may not require emergency care; however, always assume that these seizures are serious, because you may not be able to make the diagnosis.

62
Routes of Exposure Ingestion Inhalation Injection Absorption

63
CNS Stimulants S/S Excitability Agitation Tachycardias Tachypnea
Dilated Pupils Hypertension Lack of sleep

64
CNS Depressants S/S Euphoria Drowsiness Hypoventilation Bradycardias
Hypotension Dilated, sluggish pupils

65
Narcotics S/S Hypotension Bradycardia Inadequate respirations
Cool, clammy skins Pinpoint Pupils

66
Withdrawal S/S Anxiety Confusion Tremors Sweating Elevated V/S
Hallucinations Abdominal Pain

67
Delerium Tremens Occurs 1-14 days after the patients last drink
An episode may last 1-3 days S/S p. 589

68
Causes of Shock Fluid loss (not just blood loss) Pump Failure
Vasodilation Hypoxia

69
Hypovolemic Shock Results from a decrease of the volume of blood available for perfusion to the body’s organs. External or Internal Bleeding (hemorrhagic shock) Plasma loss from burns Dehydration from vomiting or diarrhea
 Plasma loss from burns. Dehydration from vomiting or diarrhea.")
70
Obstructive Shock Mechanical obstruction or compression that prevents blood from reaching the heart. Pulmonary embolism Tension pneumothorax Cardiac tamponade

71
Distributive Shock Abnormal distribution of blood in the vessels or throughout the body. Causes and insufficient amount of blood to reach the heart. Massive dilation of vessels or leakage of fluid from the capillaries. Neurogenic Anaphylactic Septic

72
Neurogenic Shock Also known as Vasogenic Shock
Usually the result of a spinal cord or severe head injury. Causes the nervous system to lose control of the vascular system. Blood pools in the periphery.

73
Anaphylactic Shock Results from the body’s abnormal reaction to a foreign protein. Normally from bee stings, foods, certain medications. The body releases chemicals causing the blood vessels to dilate and leak. Bronchioles constrict. Without immediate care, the patient will die.

74
Septic Shock Results from toxins produced by a severe infection (usually bacterial). Toxins cause a reaction that dilates the blood vessels and allows blood to pool in the extremities and fluid to leak from the vessels.

75
Cardiogenic Shock Results from inadequate pumping of the heart. CAD
AMI Heart rhythm abnormalities Heart valve disease CHF

76
Stages of Shock Compensatory Decompensated (progressive) Irreversible
 Irreversible")
77
Treatment of Shock Recognition is the most important key.
Lay patient flat. Elevate legs inches (shock position) Keep patient warm. O2 15l/m NRB Treat patient gently.
 Keep patient warm. O2 15l/m NRB. Treat patient gently.")
78
Pneumothorax Defined as an accumulation of air in the pleural cavity, causing collapse of a portion of the lung. Causes? Results in a decrease in gas available within the alveoli. Signs and symptoms include: chest pain worse with inspiration, tachypnea, decreased or absent breath sounds.

79
Open Pneumothorax AKA “Sucking Chest Wound”
Caused by an open wound to the chest. Treatment includes immediate occlusion to the opening with a 3 sided occlusive dressing.

80
Tension Pneumothorax An immediately life-threatening condition.
Results from a pneumothorax that continues to trap air in the thoracic cavity with no release of the air. Air accumulates in the thoracic cavity on the injured side. The lung completely collapses and compresses and shifts the mediastinum to the uninjured side.

81
Tension Pneumothorax Uninjured lung, heart, and large veins are compressed, resulting in reduced CO, ineffective ventilations, and severe hypoxia. Signs include: cyanosis, unequal movement of the chest, distended neck veins, deviation of the trachea to the uninjured side. Can this be caused by an open chest wound?

82
Pericardial Tamponade
Trauma causes bleeding in the pericardium. The pericardium cannot expand, so the blood causes pressure on the heart, resulting in reduced CO, blood backup into the venous system. This is a life threatening condition. Signs similar to a tension pneumothorax, but with normal breath sounds.

83
Pericardial Tamponade
Signs include: JVD, shock, tachycardia, hypotension, narrowing pulse pressures, weak pulses. Symptoms progressively worse as the pericardium continues to fill with blood. Normally causes from a penetrating injury.

84
Heat Cramps Caused by electrolyte imbalances by over-exerting muscles
Normally in the large flexor muscle groups: abdominal, gluteus, hamstrings

85
Heat Exhaustion The body has maximized its heat-dissipating mechanisms and is beginning to shut down Pale and very sweaty Mild aloc, dizzy Normal body temperature

86
Heat Stroke The Body’s heat dissipating systems shut down
Body becomes over heated, and keeps heating Damages brain cells, causes seizures Hot, red skin. May or may not sweat (50%) Up to 80% mortality rate if not treated
 Up to 80% mortality rate if not treated.")
87
Major Signs/Symptoms Elevated Core Temperature Muscle Cramps
Weakness/Exhaustion Dizziness Tachycardia Tachypnea Nausea/Vomiting Seizures Headache ALOC

88
Care and Treatment Normal to Cool skin Move to cool place Oxygen
Remove clothing Apply cold compresses Shock position Fluids

89
Care and Treatment Hot/dry skin Remove from heat Remove clothing
Oxygen Cold packs to groin, neck, armpits, behind knees Spray tepid water on patient Fan patient Keep skin wet

Similar presentations