Download presentation
Presentation is loading. Please wait.

1
Surgical Core Curriculum - Gyn Onc
Amreen Husain, M.D.

2
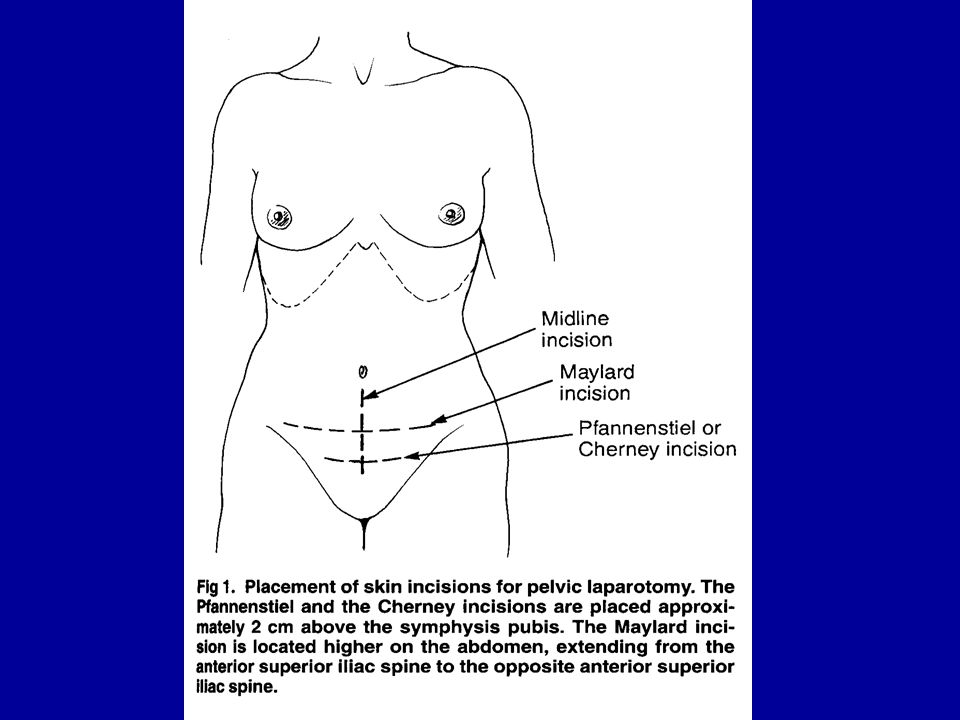
Abdominal Wall Determine best incision for planned surgery
Several layers depending on the orientation of incision Course of vessels in abdominal wall. Potential need for preservation of epigastric vessels Potential placement of stoma

3
Abdomen Landmarks to note Costal margins Xiphoid process Umbilicus
Anterior superior iliac spines Inguinal creases Pubis

4
Layers of abdominal wall
Skin Superficial fascia External and internal obliques Transversus abdominis muscles, Aponeurosis and fascia Rectus muscles and sheaths Preperitoneal fat Parietal peritoneum

5
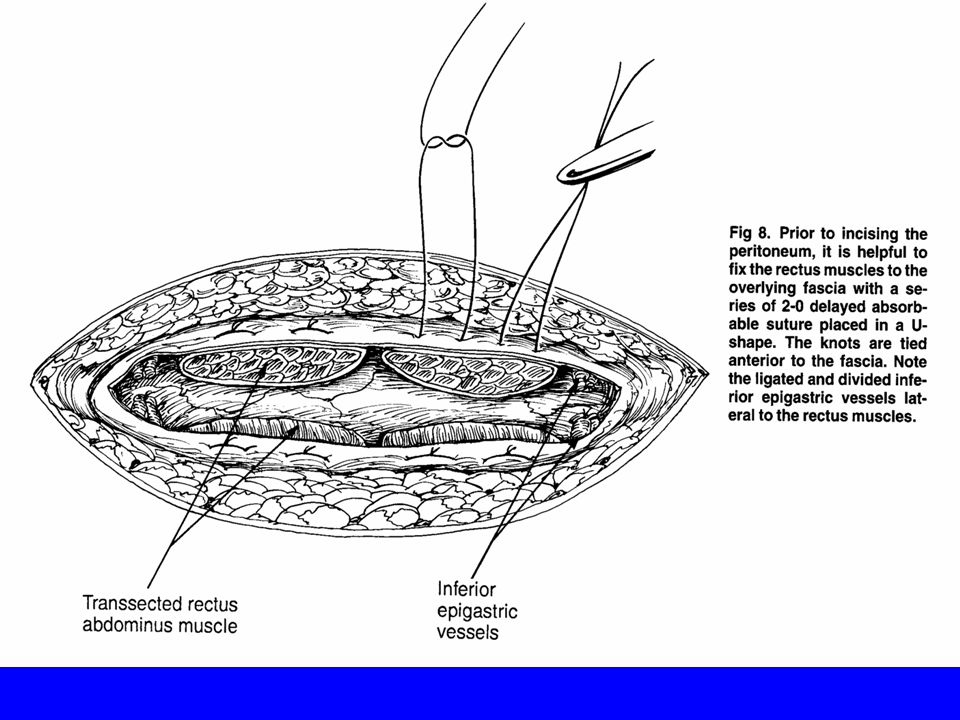
Rectus muscle Blood supply derived from sup epigastric artery (branch of int mammary or thoracic artery) and inf epigastric artery (branch of external iliac artery. Nerve supply from anterior rami of thoracic nerves from T6-T12 which enter posteriorly then divide ant, medial and lateral. Denervation occurs if muslce is divided longitudinally or freed laterally
 and inf epigastric artery (branch of external iliac artery. Nerve supply from anterior rami of thoracic nerves from T6-T12 which enter posteriorly then divide ant, medial and lateral. Denervation occurs if muslce is divided longitudinally or freed laterally.")
11
The Pelvis Surrounded by bony structures:
Sacrum, ischium, ilium and pubic bones Floor is composed of muscles: Piriformis, coccygeus and levator ani

12
The Pelvis Divided into an anterior and posterior component by the transversely oriented broad ligament in the center of which is the uterus Broad ligament has two layers : anterior and posterior leaves, round ligament runs anterolateral in the broad ligament to the pelvic wall

13
The Pelvis Ovaries attached to posterior leaf of the broad ligament by meso-ovarium, to the uterus by the ovarian ligament and to the pelvic wall by the infidibulo-pelvic ligament which contains the ovarian vessels and lymphatics Adnexal triangle an important landmark – bounded ant by round ligament, post by IP ligament and laterally by peritoneal reflection over psoas. Allows easy access to the retroperitoneum

15
Surgical Anatomy of the Pelvis
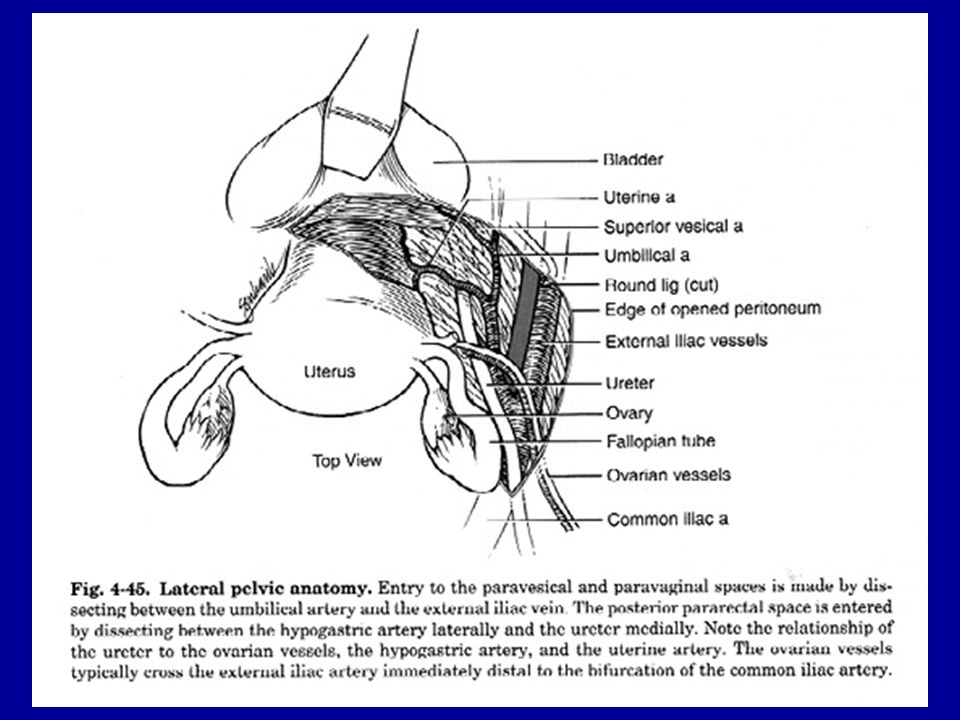
Pelvic organs include the uterus, cervix and vagina, ovaries and Fallopian tubes, bladder, pelvic ureters, rectum and portion of the sigmoid Eight tissue planes which are avascular two dimensional potential spaces until developed by the surgeon Three pairs of fibrovascular ligaments

16
Avascular Tissue Planes
Paired Spaces: Paravesical/paravaginal spaces Pararectal spaces Unpaired spaces: Prevesical (retropubic) space of Retzius Vesicovginal space Rectovaginal space Presacral (retrorectal) space
 space of Retzius. Vesicovginal space. Rectovaginal space. Presacral (retrorectal) space.")
18
Fibrovascular ligaments
Cardinal ligaments Constitute the thickened posterior most portion of broad ligament Arises from endopelvic fascia of the lateral cervix and extends to pelvic sidewall where it inserts into the endopelvic fascia Posterior portion contains a major component of the autonomic nerve supply to the bladder and rectum Contains the uterine, vaginal, inferior vesical and middle rectal arteries and veins as well as lymphatics Ureter penetrates upper portion just below uterine artery 1-2 cm lateral to the isthmus of the uterus

19
Fibrovascular ligaments
Uterosacral ligaments with rectal pillars Posterolateral thickenings which originate from posterolateral aspect of the cervix and run to anterolateral aspect of the rectum they straddle the posterior cul-de-sac Rectal pillars are longitudinal fibrovasuclar bundle btwn vagina and rectum, run the length of the vagina

20
Fibrovascular ligaments
Bladder pillars Paired longitudinal fibrovascular bundles that run the length of the vagina anteriorly and form the lateral limits of the vesicovaginal space Upper end connects to the lower half of the cervix forming the vesico-uterine ligament

22
The Ureter Crossing Retroperitoneal during its entire passage from the kidney to the bladder. Enters the pelvis by crossing over the vessels at or just proximal to the bifurcation of the common iliac artery On the left it passes under the proximal sigmoid colon and on the right passes under the cecum and terminal ileum

23
The Ureter As the ureter enters the pelvis it becomes attached to the lateral pelvic wall peritoneum and continues till it reaches the level of the uterosacral ligament and the posterior leaf of the broad ligament Ureter then contiunues through the cardinal ligament to the bladder going under the uterine artery

26
Arteries and Veins Ovarian vessels
Ovarian arteries arise from the abdominal aorta 2-3 cm below the renal arteries Ovarian vein on the right enters the vena cava below the right renal vein; the ovarian vein on the left enters the renal vein lateral to the vena cava

27
Arteries and Veins Common iliac vessels
Common iliac artery begins at the lower end of L4 and follows the pelvic brim laterally terminating over the sacroiliac joint by dividing into the external iliac and hypogastric (internal) iliac arteries Ureter crosses both common iliac arteries near their bifurcation Common iliac veins lie posterior to the artery, the left common iliac vein passes under the proximal part of the right common iliac artery
 iliac arteries. Ureter crosses both common iliac arteries near their bifurcation. Common iliac veins lie posterior to the artery, the left common iliac vein passes under the proximal part of the right common iliac artery.")
28
Arteries and Veins External iliac vessels
External iliac vein arises at lumbosacral joint and ends by passing under the inguinal ligament to become the femoral artery Main branches are the deep circumflex and inferior epigastric vessels External iliac veins are positioned inferiomedial to the arteries

29
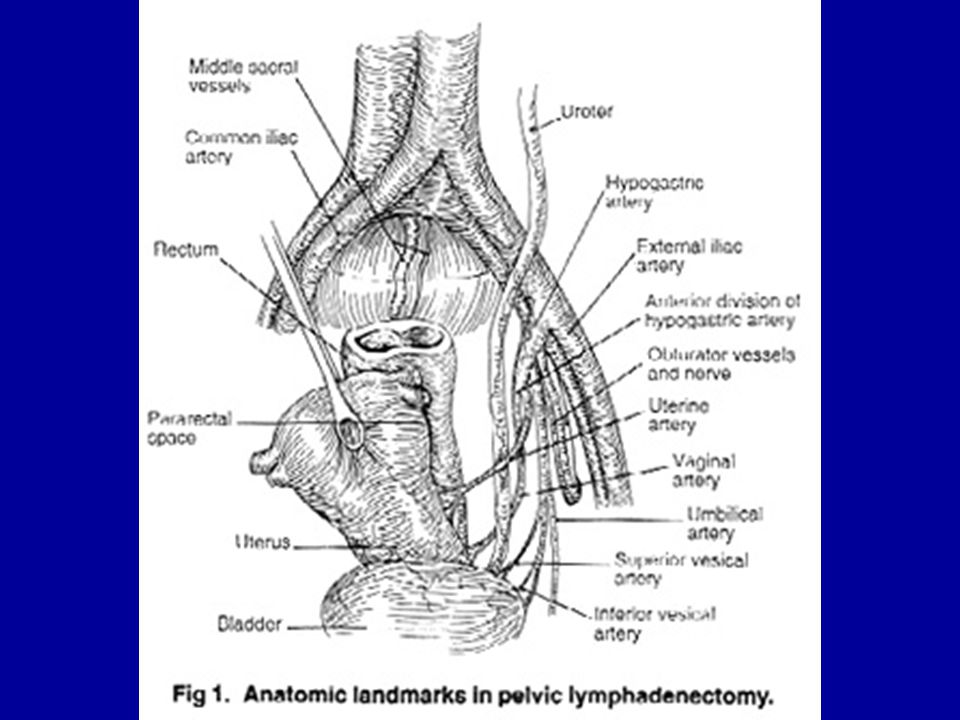
Arteries and Veins Hypogastric Arteries
Posterior and Anterior divisions at 4 cm from its origin Anterior Trunk : Six primary branches in order Common branch giving rise to the uterine, umbilical, superior vesical and sometimes vagina Obturator, Inferior vesical, middle Rectal, internal pudendal and inferior gluteal Posterior Trunk Four branches none of which supply pelvic viscera Iliolumbar, superior and inferior lateral sacral, superior gluteal

33
The Groin Femoral Triangle
Bounded superiorly by the inguinal ligament, laterally by the medial border of the sartorius muscle and medially by the adductor longus muscle Structures passing via the subinguinal space from the pelvis to the leg from lateral to medial are the lateral femoral cutaneous nerve, iliopsoas muscle, femoral nerve, then the femoral artery, femoral vein, femoral canal w/ lymphatics and femoral branch of the genitofemoral nerve

35
The Small Intestine Jejunum and Ileum combined average 22 ft in length of which the jejunum accounts for 40%. Jejunum and ileum differ in that the jejunum is thicker, has thicker mucosal folds, the mesenteric fat extends onto the wall of the ileum but not the jejunum, the vasa recta are shorter in the ileum

36
The Small Intestine Arterial Supply
Entire blood supply derived from the superior mesenteric artery (SMA) a ventral midline branch of the aorta. SMA enters the base of the mesentery as it emerges from between the duodenum and pancreas Branches are : Common inferior pancreaticoduodenal a., the middle and right colic a., ileocolic a., series of jejunal and ileal branches which anastomose with each other forming arcades.
 a ventral midline branch of the aorta. SMA enters the base of the mesentery as it emerges from between the duodenum and pancreas. Branches are : Common inferior pancreaticoduodenal a., the middle and right colic a., ileocolic a., series of jejunal and ileal branches which anastomose with each other forming arcades.")
37
The Large Intestine 4-6ft in length from ileocecal junction to the anus. Divisible into the cecum and appendix; the ascending, transverse, descending and sigmoid colon; Rectum and anus Ascending and descending colon are retroperitoneal while transverse and sigmoid colons have distinct mesenteries

39
The Large Intestine Arterial Supply
Derived from superior and inferior mesenteric arteries Marginal artery of Drummond is a scalloped continuous vessel formed by anastomosing arcades of the ileo-colic, right, middle, left colic and sigmoidal arteries Inferior mesenteric artery (IMA) arises from the aorta at L# about 3-4 cm from bifurcation, Branches to the left colic artery, sigmoidal arteries (2-4), becomes the superior rectal artery in the pelvis
 arises from the aorta at L# about 3-4 cm from bifurcation, Branches to the left colic artery, sigmoidal arteries (2-4), becomes the superior rectal artery in the pelvis.")
41
Ureteral Injuries Incidence is 0.1% - 1.5% in pelvic surgery
75% during gynecologic surgery ¾ during abd surgery ¼ during laparoscopic surgery Most common causes of litigations against gyn surgeons

42
Anatomy of the Ureter Retroperitoneal
25-30cm in length : divided into abdominal and pelvic segments by the pelvic brim Three layers : mucosa lined with transitional epithelium muscularis made up of interweaving smooth muscle fibers Adventitia containing intercommunicating network of blood vessels

43
Embryology Close proximity to reproductive organs due to proximity of mesonephric ducts and mullerian system Congenital anomalies occur concomitantly % of the time Most common is ureteral duplication – 1% of women

44
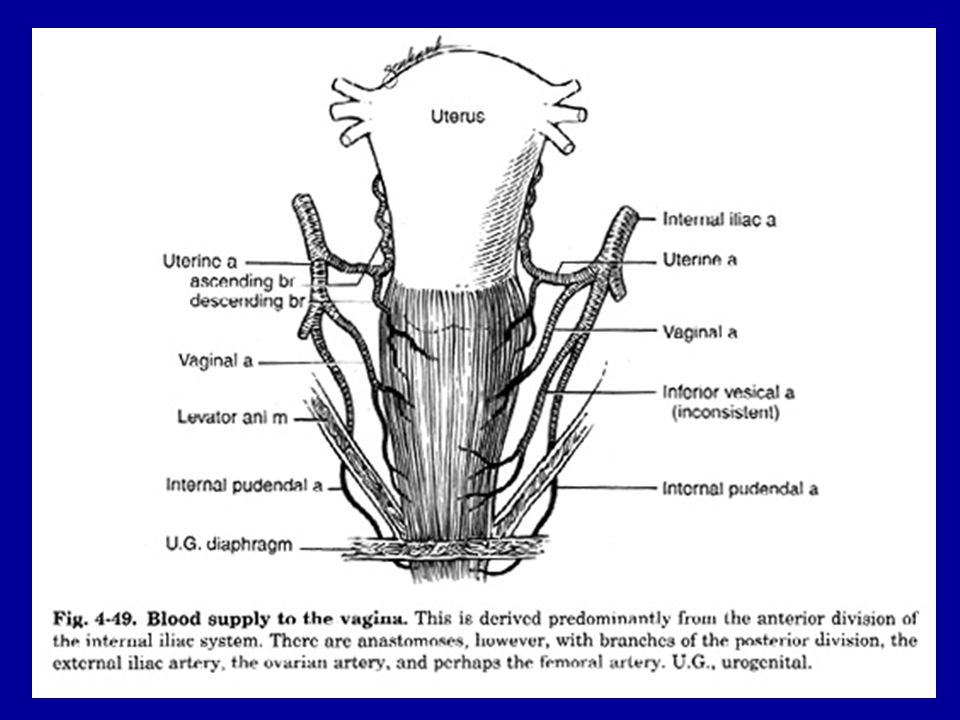
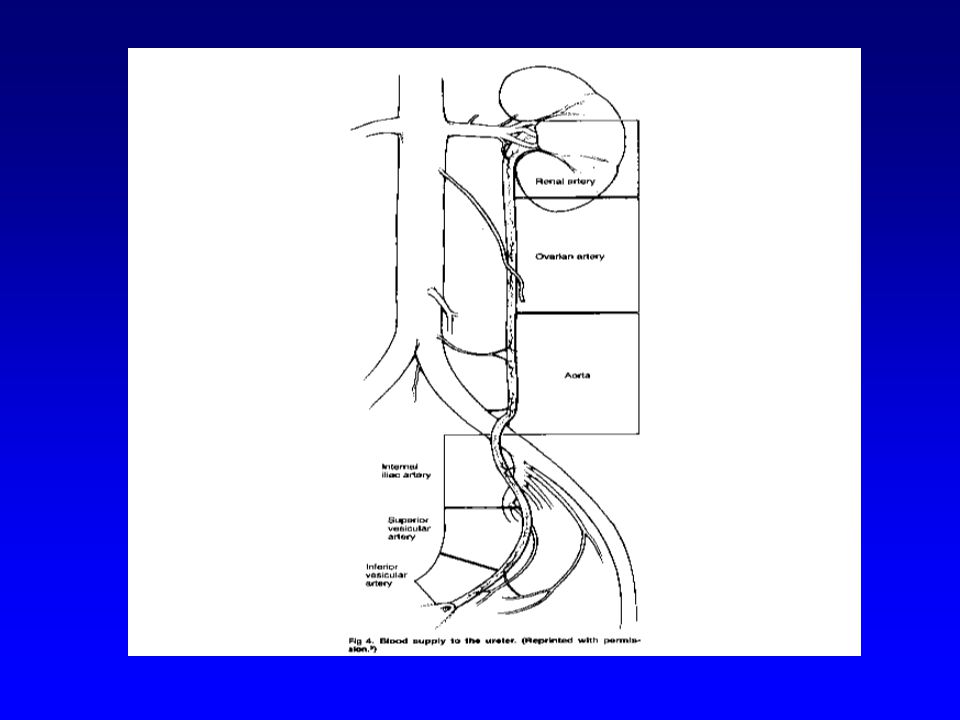
Blood supply Segmental with much anastomising
Cephalad – supplied by branches of renal and ovarian arteries Middle – form aortic and common iliac branches Pelvic – from hypogastric, rectal and vaginal arteries

46
Path of the ureter Abdominal ureter : runs along anterior surface of the psoas muscle and posterior to the ovarian vessels Crosses pelvic brim anterior to common iliac at its bifurcation

47
Path of the Ureter Pelvic ureter: travels along the pelvic sidewall lateral to the sacrum and anterior to the hypogastric. Veers medial as it passes beneath the uterine artery approx 1.5cm lateral to the internal os then passes into the tunnel of the cardinal ligament and travels medially and anteriorly over the vaginal fornix to enter the bladder. Travels 2cm within bladder wall before exiting

48
Location of ureteral injuries
Cardinal ligaments where uterine artery and ureter cross or at the ureteral tunnel Infundibulopelvic ligament Lateral pelvic sidewall along the uterosacral ligaments Intramural portion of ureter

49
Types of injuries Crushing from a clamp Ligation Transection
Angulation with secondary obstruction Ischemia due to thermal injury Resection

50
Prevention Identification and visualization
After dividing round ligament enter broad ligament along psoas muscle and dissect retroperitoneal space, ureter is attached to the medial leaf of the broad ligament No benefit to preop IVP or stenting Can also be palpated (with experience!!) Can also be identified as it crosses iliac
 Can also be identified as it crosses iliac.")
52
Basic steps - TAH Routine identification before clamping IP
Mobilize bladder from vaginal cuff for at least 1cm Clamp uterine artery at the internal os and at right angles to the uterus Clamp inside prior pedicles once the uterine artery has been clamped

53
Basic steps - TVH Develop vesico-vaginal space with retraction of the bladder anteriorly Palpation of the ureter Small pedicle bites medial to where ureter is palpated

54
Recognition of uerteral injury
70% not identified until post –op Morbidity due to : Necrosis w/ extravasation Fistula formation Stenosis w/ hydronephrosis and renal loss Uremia and death with bilat obstruction (rare)
")
55
Signs and Symptoms Flank pain Fever Persistent Ileus
Ascites or retroperitoneal fluid collection Rise by 0.8 in Creatinine Fistula formation 8-10 days post-op Usually subtle – high index of suspicion U/S normal in 20% - CT-IVP is standard test

56
Management of ureteral injury
Antegrade or retrograde stent placement If stent placement unsuccessful decide between immediate repair vs PCN and delayed repair < 72hrs – immediate repair >2wks – PCN and repair in 6-8 wks, obtain IVP prior to repair as spontaneous healing can occur in upto 80%

57
Principles of Repair Atraumatic handling
Healthy mucosa-to-mucosa approximation Minimal mobilization and dissection Tension free Stent placement Epithelial healing in 2 weeks Normal peristalsis in 4 weeks

58
Ureteroneocystotomy Ureteral injuries 5-6cm from bladder
Non-tunneled reimplantation into bladder Mobilize proximal ureter Mobilize bladder Perform cystotomy in tranverse fashion

60
Additional length Psoas hitch – bladder stretched to reach Psoas and attached to the muscle Boari flap – segment of bladder made into a tunnel

62
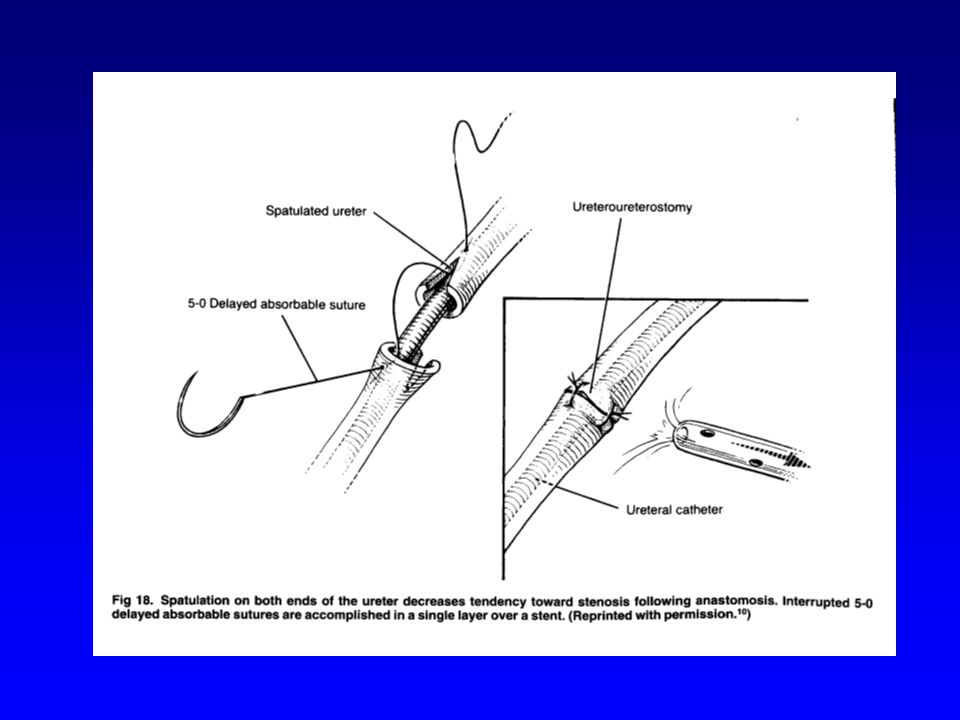
Ureterouretorostomy Injuries above the pelvic brim Freshen edges
Cheatle incision on either end Reapproxiamte with 5-6 stitches using 4-0 Vicryl, place all stitches then tie Stent

65
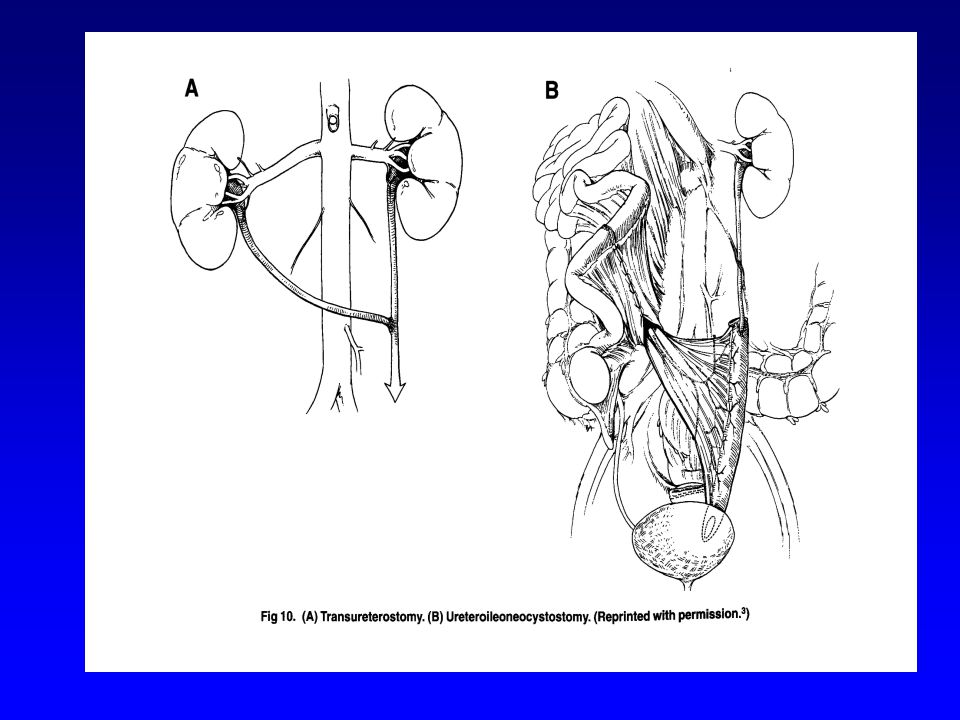
Other Techniques Transureterouretrostomy
Transposition of segment of ileum Mobilization of kidney

67
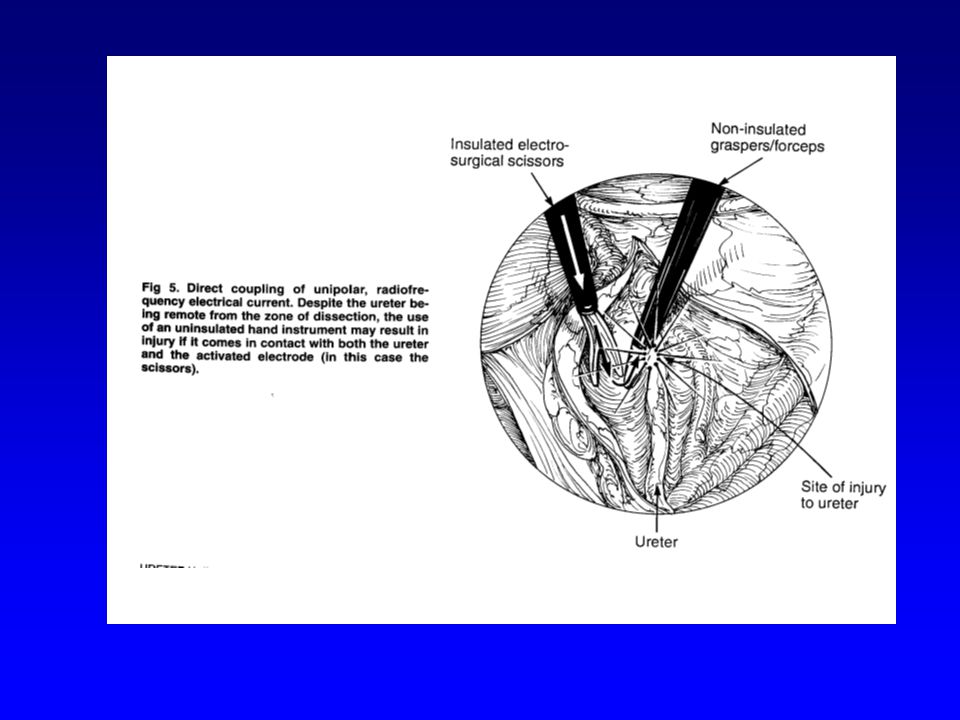
Laparoscopy and ureteral injuries
Incidence about 0.5% Usually due to electrocautery and eqaully divided between mono and bipolar Also commonly due to stapling device when used on uterine arteries or IP as width of device is 1.2cm Particular care when anatomy is distorted

69
Cystotomy and Repair Most common urinary tract injury during hysterectomy Avoid by sharply dissecting bladder of cervix and anterior vagina Trigone is only part that is fixed and not easily distensible, adjacent to upper vagina in the anterior vgainal fornuix Injury near vaginal cuff or cervix is always close to or at trigone

70
Repair of bladder dome injury
Identify entire length and ends of defect Use 3-0 or 4-0 Vicryl as 3weeks required for complete healing and chromic only maintains strength for 4-5days Running suture through mucosa and muscularis, important to invert and reapproximate mucosa 2nd layer of imbricating interrupteds Can be closed in any direction Drain for 5-7 days in healthy tissue

71
Repair of trigone injury
Visulize ureteral orifices Keep in mind ureters travel within bladder wall 2cm laterally, can be palpated Two layer closure, maintain suture lines in direction away from ureters and trigone Retrograde filling and Cystoscopy at end Drain for min10-14 days

Similar presentations